
Abstract
Background:
Drooling is a prevalent and disabling condition leading to serious psychosocial and health ramifications. The aim of this study is to analyze the efficacy and safety of 4- versus 2-duct ligation in treating anterior drooling.
Methods:
A systematic review of the CINAHL, PubMed, and Embase databases was conducted from inception to September 13, 2025. Inclusion criteria were the analysis of both the success rate and associated complications of 2-duct ligation or 4-duct ligation as an independent treatment strategy for anterior drooling.
Results:
4-duct ligation showed a higher success rate risk difference (RD) 0.47 (95% CI [0.25, 0.68]), risk ratio (RR) 2.99 ([2.15, 4.15]) than 2-duct ligation with a comparable or lower complication rate. Reported complications included ranula, infection, bleeding, dryness, pain and swelling, anesthesia complications, and others. The most common complication seen in both types of duct ligation was infection.
Conclusion:
Ductal ligation serves as a safe and effective surgical treatment option for patients with anterior drooling. The high success rate, low operative morbidity, and non-invasive nature of the procedure make it a favorable intervention. Due to the small and variable sample sizes of each intervention, an accurate comparison for efficacy and safety cannot be made between 2- and 4-duct ligations.
Introduction
Chronic anterior drooling is a common and serious disorder seen in neurodevelopmentally disabled children. It results primarily from dysfunction of the swallowing mechanism rather than overproduction of saliva. 1 Drooling can be classified as anterior or posterior. Anterior drooling is defined as the visible spillage of saliva from the oral cavity, wetting the mouth and chin, and soiling clothing. In posterior drooling, saliva collects in the hypopharynx. 2 While anterior drooling is very common in young children, it is considered pathologic if it persists beyond 4 years of age. 3
Various physical and psychosocial stressors accompany chronic drooling, severely impairing patient and caregiver quality of life. Physically, affected children may encounter speech difficulties, increased frequency of perioral infections, and dehydration due to fluid and electrolyte loss. Serious health concerns, such as difficulty feeding and aspiration pneumonia, may result from posterior drooling. Psychologically, anterior drooling often leads to significant distress with feelings of embarrassment, low self-esteem, and social isolation.2-4
First-line treatment for drooling is conservative therapy, such as behavioral and feeding modification programs, speech therapy, physical therapy, and pharmacotherapy. 4 If drooling continues, botulinum toxin injection is the subsequent course of action followed by surgical intervention. A variety of surgical procedures exist to correct excessive drooling, including salivary gland excision, duct relocation, duct ligation, and tympanic neurectomy. These procedures can be performed alone or in conjunction with one another. 5 Disagreement persists regarding the most successful management strategy.
Duct ligation is an effective, uncomplicated, and non-invasive treatment with low morbidity. This procedure targets the submandibular and/or parotid glands. 2-duct ligation consists of bilateral clipping of both submandibular or both parotid gland ducts.5-7 3-duct ligation involves bilateral ligation of the submandibular glands and single ligation of a parotid gland. Lastly, 4-duct ligation entails bilateral ligation of both the parotid and submandibular glands.2-4 While 4-duct ligation appears to be a reasonable approach for reducing saliva pooling and aspiration in patients with posterior drooling, data analyzing duct ligation as remediation for chronic anterior drooling is heterogeneous and inconsistent. 6 Although it might seem intuitively more effective than 2-duct ligation, 4-duct ligation likely carries a higher risk of complications, such as xerostomia. 2 This systematic review aims to assess the efficacy and safety of 2- and 4-duct ligations in treating anterior drooling as well as report on potential complications of the procedures.
Methods
A systematic review of the CINAHL, PubMed, and Embase databases was conducted from inception to September 13, 2025, with the help of a senior medical librarian. The search strategy used variations in text words found in the title, abstract, or keyword fields, and relevant subject headings to retrieve articles pertaining to duct ligation in children with excessive drooling. The full search strategies can be found in the appendix.
Screening was conducted by four independent reviewers; no automation tools were used, and conflicts were resolved by consensus. Studies were eligible if they analyzed treatment success and/or complication rates of 2- or 4-duct ligation performed as a solitary intervention for anterior drooling. Studies were excluded if they investigated duct ligation exclusively for posterior drooling, focused solely on complications or efficacy without reporting both outcomes, or evaluated duct ligation in combination with other procedures (e.g., combined submandibular gland excision and parotid duct ligation). Clinically relevant patient characteristics, including mobility, posture, oral motor function, and comorbidities, were extracted when reported; however, these variables were inconsistently described across the nine included studies and were therefore not incorporated into comparative analyses. Meta-analysis was not performed due to clinical and methodological heterogeneity, including overlapping patient populations, variable outcome definitions, and inconsistent reporting of summary statistics. 6
Data extraction was performed independently by three reviewers, with discrepancies resolved through discussion and consensus. Studies were grouped according to intervention type (2- vs 4-duct ligation), and each group was synthesized independently. Studies that did not report sufficient summary statistics required for quantitative synthesis were excluded from pooled analyses. No subgroup analyses were performed due to the limited number of included studies and heterogeneity in outcome definitions.
Collected data consisted of treatment success rates, complication rates, and reported postoperative complications; no additional study-level or patient-level data were sought. Study-specific definitions of treatment success and complication are listed in Table 1. For dichotomous outcomes, effect measures included risk ratios (RRs) and risk differences (RDs), each reported with corresponding 95% confidence intervals. A fixed-effects model (Figures 1 and 2) was applied when statistical heterogeneity was low (I² = 0%), assuming a single true effect size across studies, whereas a random-effects model (Figures 3 and 4) was used when heterogeneity was substantial (I² = 76%), accounting for between-study variability in treatment effects. Results of individual studies and pooled syntheses are presented using forest plots and summary tables. All analyses and forest plots were generated using Review Manager (RevMan) version 5.4.1.
Definitions of Treatment Success and Complication Criteria.
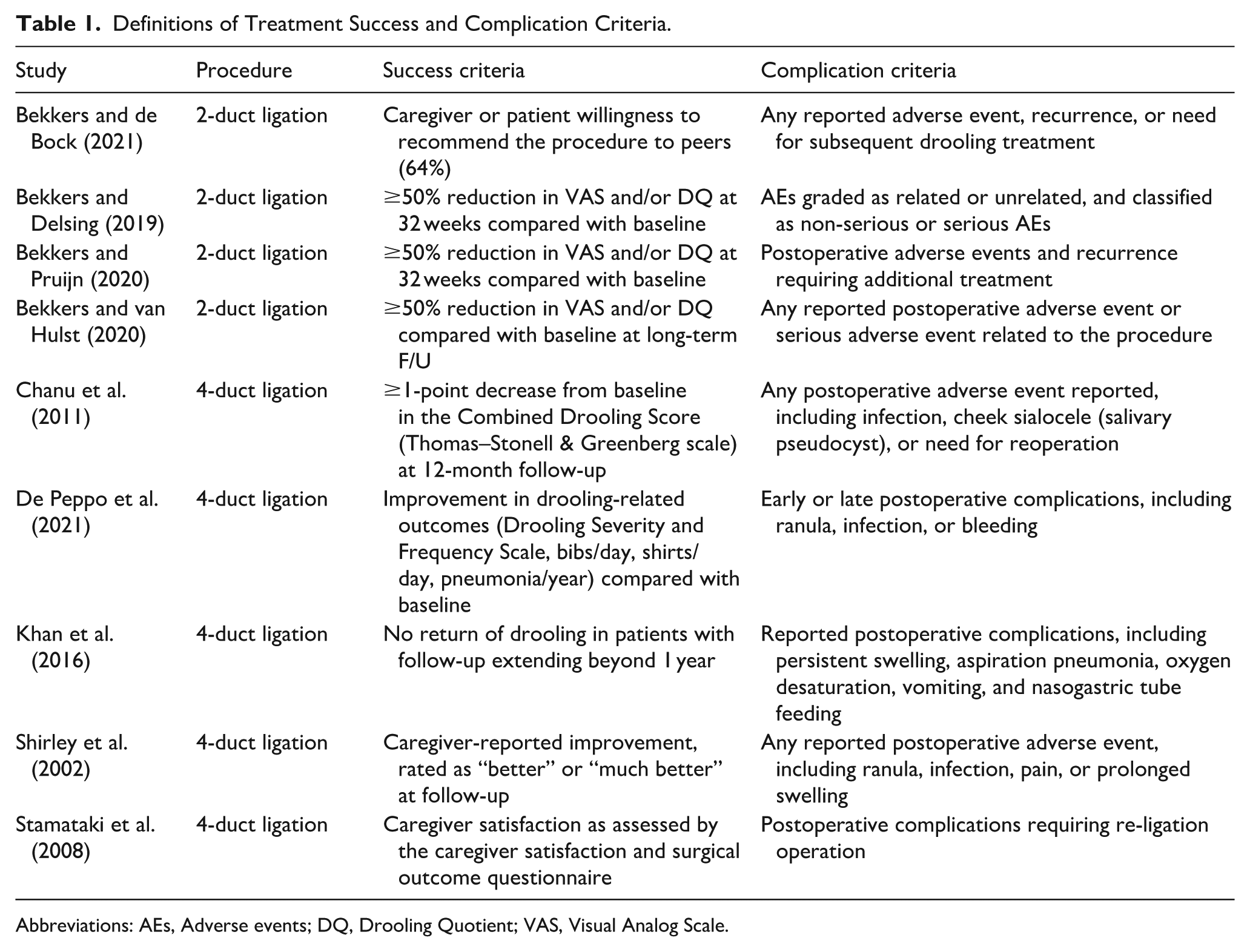
Abbreviations: AEs, Adverse events; DQ, Drooling Quotient; VAS, Visual Analog Scale.
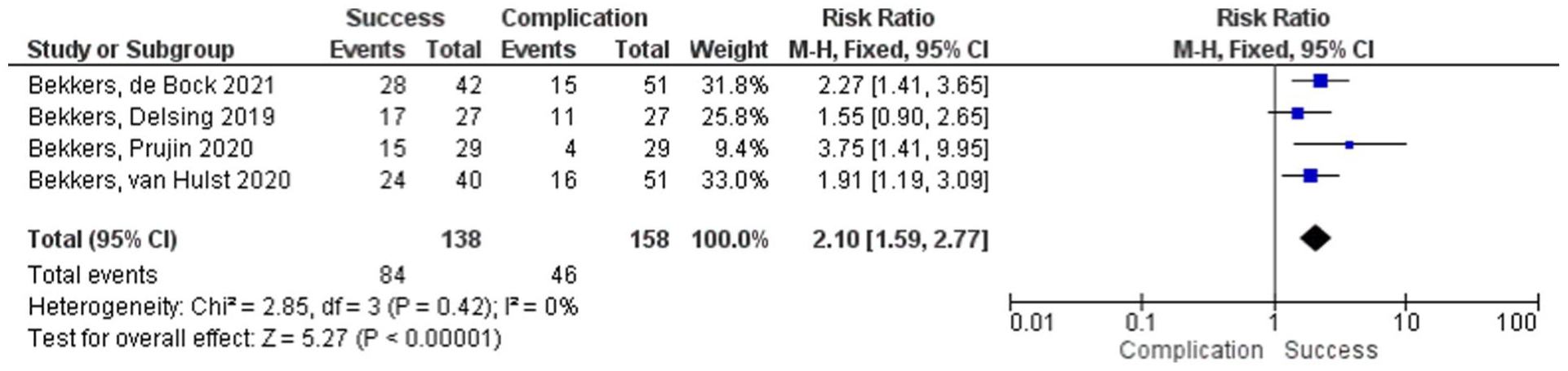
Forest plot of success following 2-duct ligation for anterior drooling, pooled with a fixed-effects model; squares denote study estimates proportional to weight and horizontal lines denote 95% CI; the diamonds indicate the pooled effect; CI = confidence interval; I 2 = heterogeneity index.
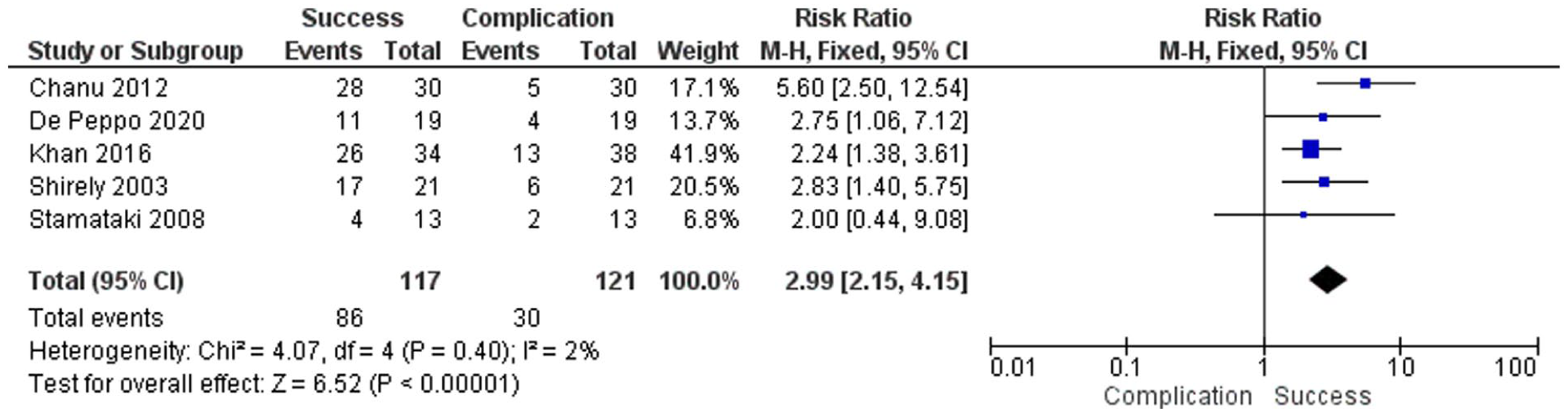
Forest plot of success following 4-duct ligation for anterior drooling, pooled with a fixed-effects model; squares denote study estimates proportional to weight and horizontal lines denote 95% CI; the diamonds indicate the pooled effect; CI = confidence interval; I 2 = heterogeneity index.
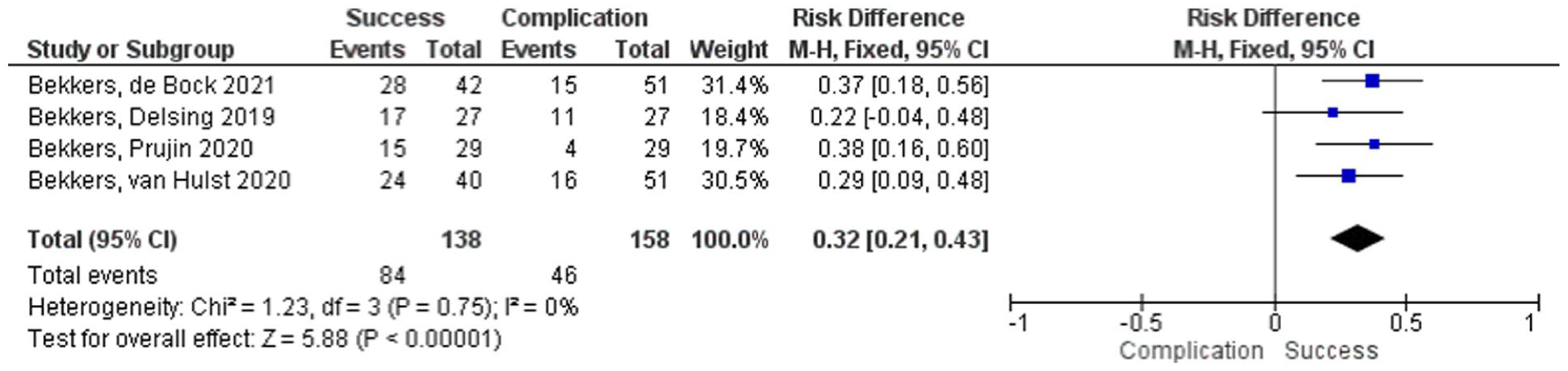
Forest plot of success following 2-duct ligation for anterior drooling, pooled with a random-effects model to account for between-study variability; squares denote study estimates proportional to weight and horizontal lines denote 95% CI; the diamond indicates the pooled effect; CI = confidence interval; I 2 = heterogeneity index.
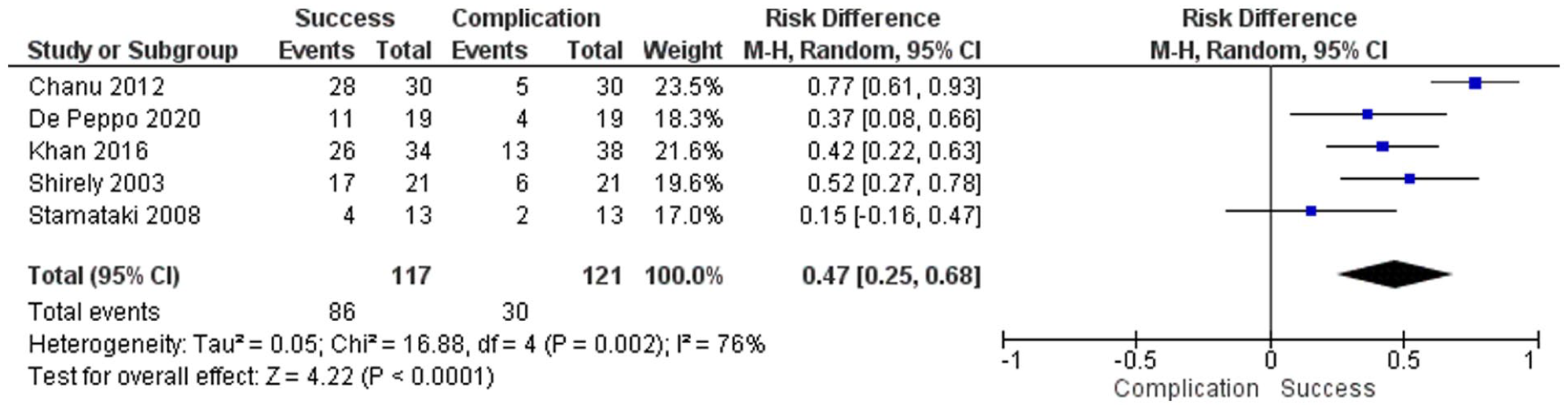
Forest plot of success following 4-duct ligation for anterior drooling, pooled with a random-effects model to account for between-study variability; squares denote study estimates proportional to weight and horizontal lines denote 95% CI; the diamond indicates the pooled effect; CI = confidence interval; I 2 = heterogeneity index.
Results
222 articles were screened, and 9 studies fulfilled the inclusion criteria (Figure 5). 4 of these studies investigated 2-duct ligation7-10 while 5 studies addressed 4-duct ligation.2-4,11,12 Using the Newcastle-Ottawa scale and Cochrane RoB 2 scale (Table 2), the 9 included studies showed low to moderate risk of bias. Most observational studies were judged to have a moderate risk of bias primarily due to a lack of adjusting for confounding variables. 2 of the studies screened fulfill the inclusion and exclusion criteria for this systematic review; however, they do not report the standard deviations or standard errors in their results. In addition, they lack a second variable for compilation rate.13,14 This limited our statistical power to perform a meta-analysis by combining unbiased studies.
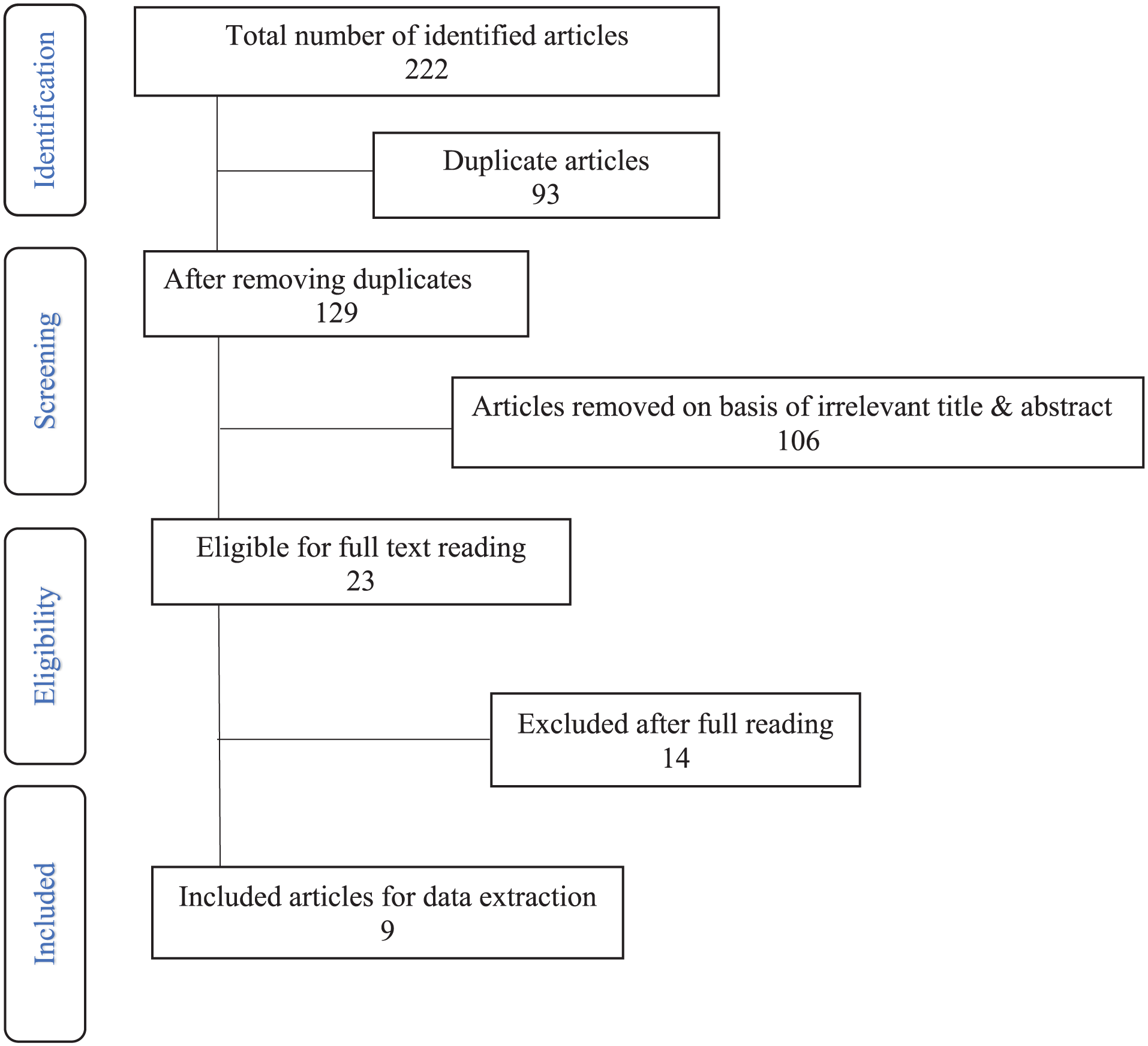
PRISMA 2020 flow diagram for study selection comparing 2- versus 4-duct ligation for anterior drooling; records identified, screened, assessed for eligibility, and included are shown; reasons for exclusions are indicated.
Newcastle-Ottawa Quality Assessment Scale and Cochrane Risk of Bias 2 Scale.
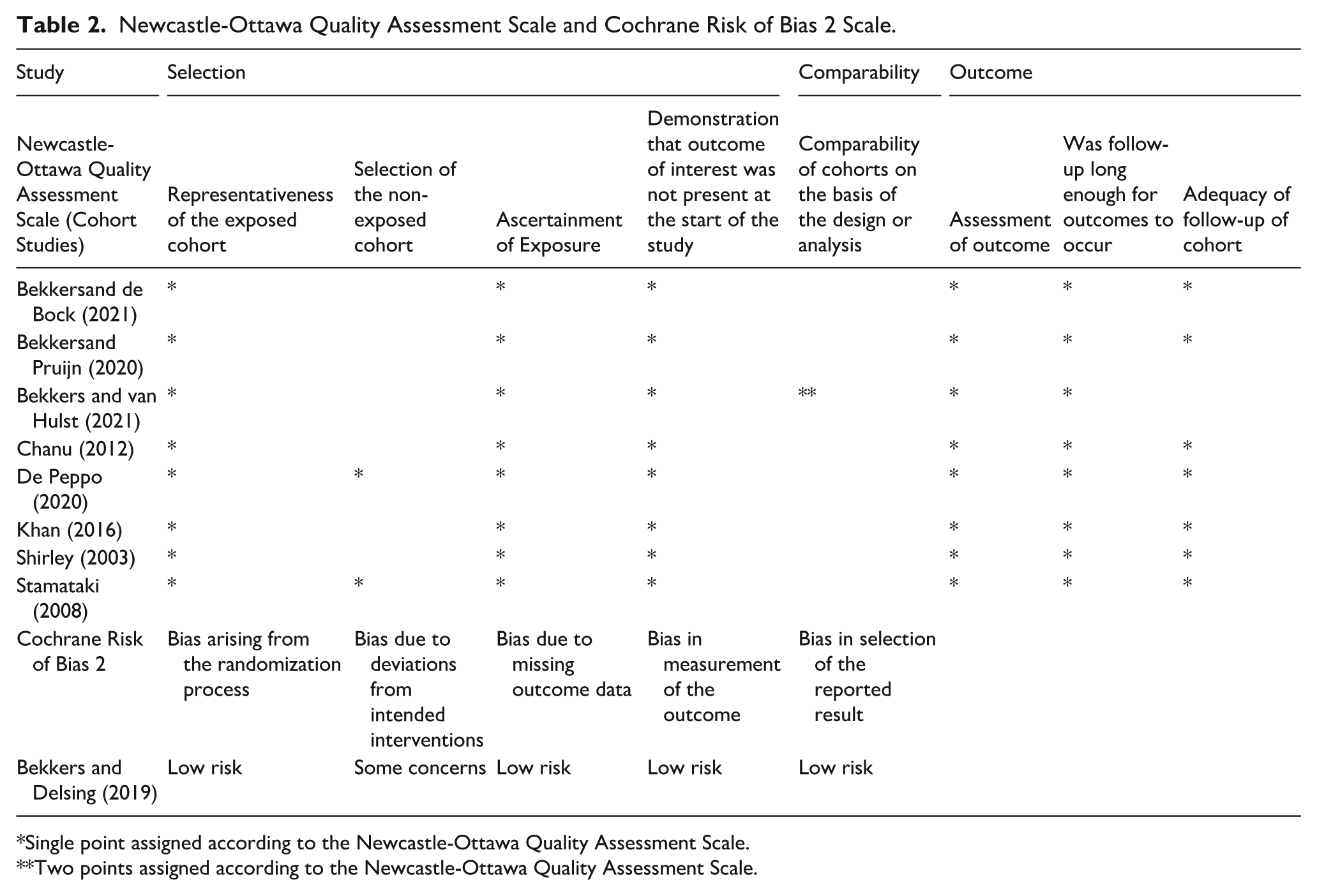
Single point assigned according to the Newcastle-Ottawa Quality Assessment Scale.
Two points assigned according to the Newcastle-Ottawa Quality Assessment Scale.
The total number of patients analyzed across the systematic reviews was 138 for 4-duct ligation and 117 for 2-duct ligation. The success rates for 4- and 2-duct ligation were 73.5% and 61%, respectively. The complication rates of both procedures were 25% for 4-duct ligation and 29% for 2-duct ligation. 4-duct ligation showed a higher success rate RD 0.47 (95% CI [0.25, 0.68]) and RR 2.99 ([2.15, 4.15]) than 2-duct ligations with a comparable or lower complication rate.
Tables 3 and 4 list the adverse events associated with 2- and 4-duct ligations reported by each study. Complications were categorized into 7 categories: ranula, infection, bleeding, xerostomia, pain, swelling, anesthesia complications, and other. Infection was the most common complication for both 2- and 4-duct ligations followed by pain and swelling.
Adverse Events Following 2-Duct Ligation Reported Across Included Studies.
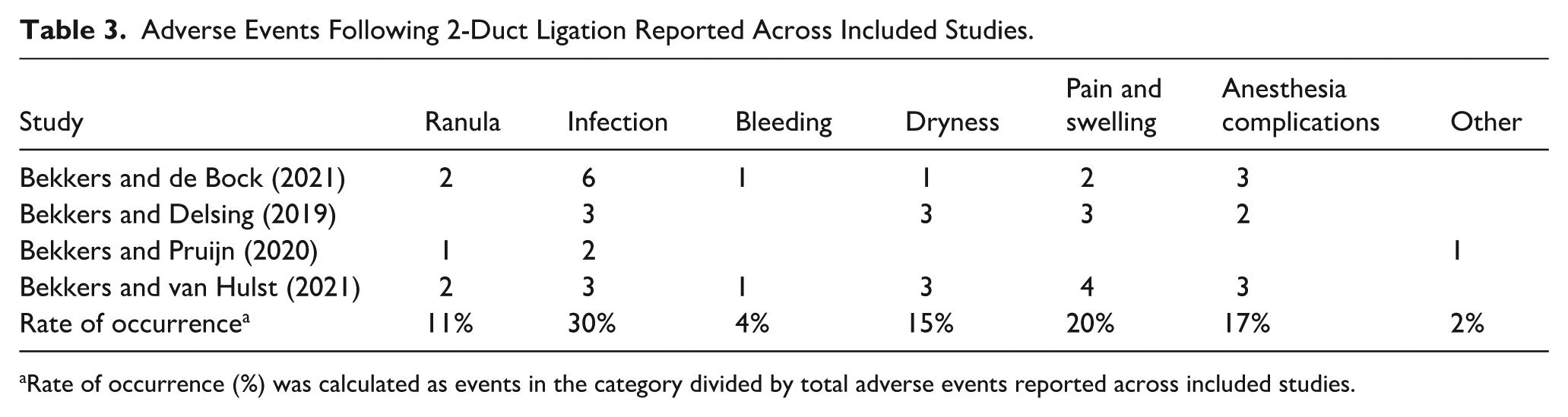
Rate of occurrence (%) was calculated as events in the category divided by total adverse events reported across included studies.
Adverse Events Following 4-Duct Ligation Reported Across Included Studies.
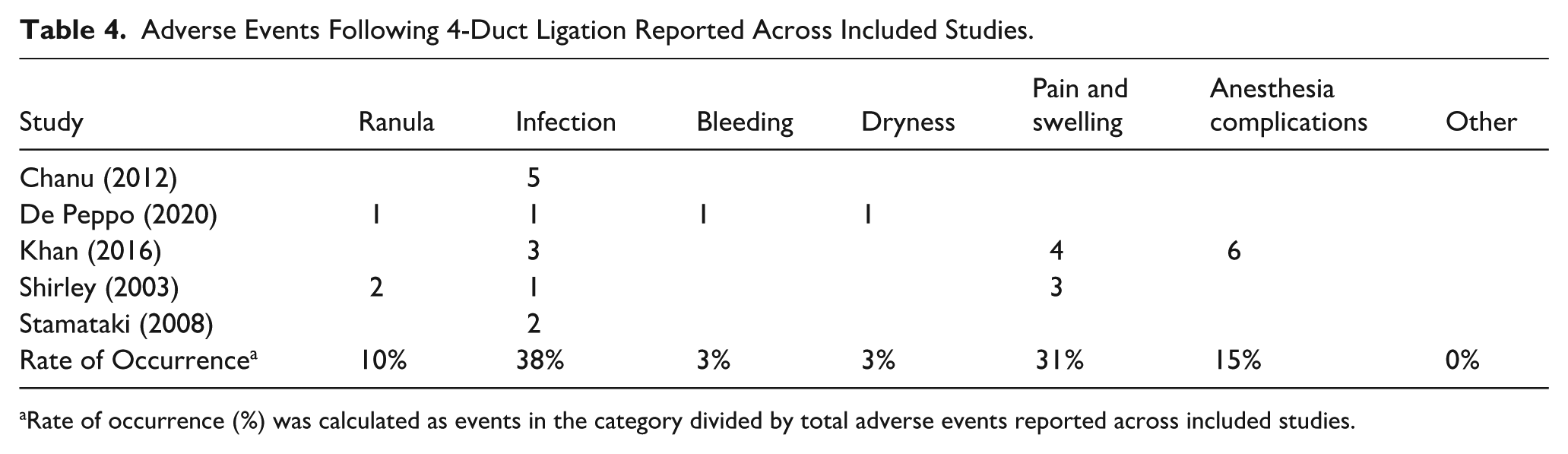
Rate of occurrence (%) was calculated as events in the category divided by total adverse events reported across included studies.
Discussion
Ligation of Wharton’s and/or Stenson’s ducts is a well-established, simple, effective, and minimally invasive treatment modality for the management of excessive drooling. Advantages of this technique include the absence of facial scars and the rapidity of the surgery. A study in a rabbit model demonstrated a reduction in the size of the parotid glands post-ductal ligation. This reduction was due to acinar atrophy and apoptosis of both acinar and ductal cells. 15 Studies have reported on outcomes of various combinations of salivary gland ductal ligations including only the submandibular ducts, only the parotid ducts, two submandibular and one parotid duct, or all four ducts. While several studies have reported a significant reduction in drooling, long-term results analyzed in some studies have been less encouraging.
This systematic review is the first study to comprehensively list the adverse events associated with ductal ligation as remediation for anterior drooling. The results align with published literature reporting on the non-invasive and safe nature of the intervention. The most common complication of both 2- and 4-duct ligations is infection, which can be treated with antibiotics. The senior author managed to decrease the likelihood of sialadenitis by simultaneously injecting botulinum toxin in the salivary glands at the time of ligation. Pain and swelling are the second most reported complications, and therapy consists of analgesics and cold compresses.
The statistically significant results of this study portray 4-duct ligation as superior to 2-duct ligation; however, the reported percentages overestimate the efficacy and safety of the former over the latter. The sample sizes for each type of ligation (N = 138 for 4-duct ligation and N = 117 for 2-duct ligation) are too small and variable to accurately compare the two interventions. In fact, there are advantages and disadvantages to each approach. 4-duct ligation is superior in that it only requires one anesthetic procedure, whereas 2-duct ligations may require an additional ligation procedure if adequate relief is not initially obtained. On the other hand, 4-duct ligation carries a greater incidence of infection, while 2-duct ligation exhibits less associated pain and swelling. The increased risk of Xerostomia found in this study with 2-duct ligation as compared to 4-duct ligation was surprising and could reflect the heterogeneity of the population studied as well as variability in reporting. Both techniques demonstrate distinct advantages and drawbacks, though based on the complication profile, the literature lacks sufficient data to definitively state one type of duct ligation as superior to the other.
There are multiple confounding variables that could have skewed the results of this review. Cerebral palsy, the neurological diagnosis of most patients in this review, is a complex disease with a wide range of severity and associated comorbidities. Baseline differences in the degree of disability could have influenced how well patients responded to treatment. For example, age, adequate posture, and normal speech have previously been analyzed as predictors of success for 2-duct ligation. 10 However, research on this matter is limited and thus proposes an avenue for future investigation and inquiries.
Another limitation of this review is the absence of a standardized definition of treatment success and complication reporting across the included studies. In addition to variability in the instruments used to assess drooling severity and frequency, individual studies applied different thresholds to define “success” limiting the direct comparability of pooled binary outcomes. Some studies2-4 utilized the Thomas-Stonell and Greenberg Drooling Severity and Frequency Scale, while others used surveys to analyze the severity of drooling as judged by the caregiver.7,9,13 The subjective nature of the reported data, combined with heterogeneous success criteria, further complicates the comparison of studies. To improve transparency, study-specific definitions of treatment success and complications were summarized in Table 1. However, inconsistencies in how outcomes were reported, prevented re-analysis of these outcomes using continuous measures. Additionally, differences in surgical techniques across institutions could have confounded the results of the included studies, adding another layer of ambiguity to the conclusions drawn from this systematic review.
Finally, the published literature consists predominantly of retrospective chart reviews. Importantly, the literature on 2-duct ligation originates from a single center, whereas studies evaluating 4-duct ligation are derived from multiple centers. This imbalance introduces the potential for substantial overlap in 2-duct ligation patient populations, which limits the generalizability of comparative findings and raises concerns regarding sampling bias. Additionally, the risk of double-counting adverse events within the 2-duct ligation cohort should be acknowledged; because this overlap cannot be disentangled without access to individual patient identifiers, complication rates should be interpreted descriptively. These limitations underscore the need for further standardized research in this domain. Future studies should prioritize prospective, randomized controlled trials to improve the quality of evidence.
The strength of this systematic review is limited by the minimal amount of research conducted on duct ligation as an independent therapy for anterior drooling as well as the aforementioned barriers. We wish to emphasize that, while these weaknesses hinder the ability to draw robust comparative conclusions, the results of this review are significant, as it is the only study to comprehensively analyze 2- versus 4-duct ligations for anterior drooling.
By systematically consolidating the available data and transparently addressing its limitations, this study underscores the significant gaps in the literature, thus reinforcing the need for future research. This study demonstrates the need for more standardized, prospective research to better inform clinical decision-making in the management of anterior drooling.
Conclusion
Duct ligation is an effective and safe intervention for patients with chronic anterior drooling. There are advantages and disadvantages to both 4-and 2-duct ligations. More research needs to be conducted to definitively compare the two interventions.
Footnotes
Appendix
Ethical Considerations
No new human subjects were involved, and no original data were collected; therefore, institutional ethics approval was not required.
Author Contributions
The study idea was conceived by J.F., A.M., S.D. An independent literature review was conducted by J.F., A.M., G.S., U.K. The data were extracted in Microsoft Excel using a table constructed by J.F., A.M., and U.K. The statistical analysis was performed by statistician S.W. and research assistant R.A. The manuscript was drafted by J.F., A.M., G.S., U.K. The manuscript was critically revised by S.D. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data supporting this review are available in the published literature cited throughout the manuscript.