
Abstract

Significance Statement
Pediatric parotidectomy involves higher risks of facial nerve injury due to unique anatomical variations. This case illustrates the successful application of a standardized four-step intraoperative facial neuromonitoring protocol 1 in a child with mucoepidermoid carcinoma. It highlights the clinical importance of routine neuromonitoring to ensure precise nerve identification, minimize surgical morbidity, and optimize long-term functional outcomes in the pediatric population.
Written informed consent was obtained from the patient’s legally authorized representative for the publication of this case report. A 13-year-old girl presented with a 2 cm right parotid mass enlarging for 2 years. Physical examination revealed a firm, immobile, nontender mass without skin adhesion, facial numbness, asymmetry, or cervical lymphadenopathy. Ultrasonography and fine-needle aspiration cytology showed atypia. Neck computed tomography (CT) scan confirmed the lesion (Figure 1A). A right superficial parotidectomy with FNM was scheduled.
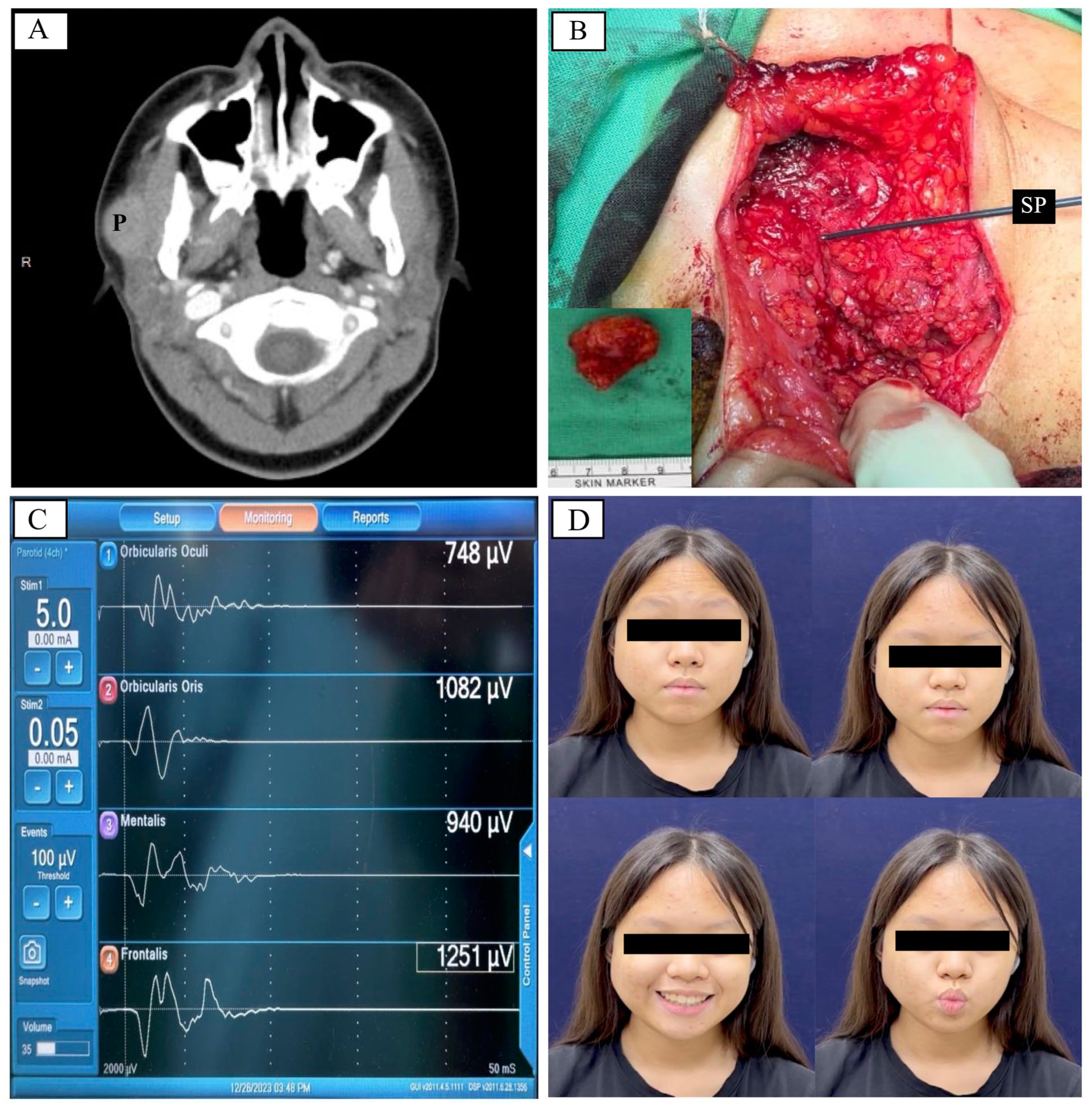
Preoperative and intraoperative findings. (A) Preoperative computed tomography imaging reveals a 2.4 cm right parotid tumor (P) in a 13-year-old girl. The tumor appears as a lobulated and enhanced lesion within the superficial lobe of the right parotid gland. (B) Intraoperative facial neuromonitoring facilitates the parotidectomy, as the stimulation probe (SP) points at the facial nerve branch. The specimen and a scale appear in the corner. (C) Postdissection electromyographic signals from the frontalis, orbicularis oculi, orbicularis oris, and mentalis muscles demonstrate stability. These signals do not show a change greater than 20%. (D) Facial expression assessment at 11 weeks postoperatively shows full symmetry. The patient exhibits no facial movement dysfunction.
Intraoperatively, a standardized four-step FNM protocol was implemented 1 :
(1) Verification (V): 10 mA stimulation at the mandibular angle confirmed system functionality.
(2) Localization (L): 5 mA stimulation to precisely identified the FN trunk before dissection (Figure 1B), with extra caution given their superficial course in pediatric patients.
(3) Predissection signals (F1): 3-5 mA stimulation at FN trunk established baseline data. During tumor resection, FNM assisted in tracing FN course, and electromyographic (EMG) signals remained stable without significant change (<20%).
(4) Postdissection signals (F2): 3-5 mA stimulation at the FN trunk after tumor excision (Figure 1C), the comparison between F1/F2 could assess FN function.
The surgery proceeded without complications. The final pathology revealed an intermediate grade mucoepidermoid carcinoma without regional lymph node metastasis. At postoperative 11 weeks, facial dynamic expressions were fully symmetric (Figure 1D). Following adjuvant radiation therapy, she remained no recurrence or abnormal facial expression at the 8-month follow-up.
In pediatric patients, the FN lies more superficially due to underdeveloped mastoid process, resulting in a more horizontal course from the stylomastoid foramen to parotid gland and increasing surgical risk. 2 The standard treatment for parotid mucoepidermoid carcinoma is superficial parotidectomy for superficial-lobe tumors and total parotidectomy for high-grade or deep-lobe disease. 3 FN preservation should remain a priority, as paralysis may significantly influence long-term quality of life.
In pediatric parotidectomy, intraoperative FNM serves as an effective adjunct for unique anatomical challenges. In this case, the V–L–F1–F2 procedure ensured precise FN identification. The superficial location of FN underscores the importance of accurate real-time localization, while quantitative assessment of F1/F2 signals enables early detection of potential injury mechanisms and timely correction of surgical maneuvers. 1 Once adequate stimulation level is confirmed, pediatric surgery can often be performed using lower stimulation currents than in adults, avoiding oversensitivity and allowing rapid and precise mapping.
Pediatric cases require meticulous dissection due to smaller anatomical structures and finer nerves. While extremely fine branches (diameter <1 mm) were not encountered, early recognition is helpful, as preserving parotid tissue outside the oncologic safe margin aids nerve preservation. Whether FNM-assisted parotidectomy in children affects long-term oncologic outcomes requires further study; however, the current surgical approach successfully preserved FN function without postoperative complications or adverse oncologic results.
In conclusion, routine intraoperative FNM in pediatric parotidectomy is strongly recommended to reduce the risk of FN injury and improve surgical results in this population.
Footnotes
Author Contributions
Y.J.C. (Ying-Jyun Chen): Conceptualization, Data collection, Manuscript writing. T.Y.H. (Tzu-Yen Huang): Conceptualization, Data interpretation, Manuscript editing, Supervision. H.Y.K. (How-Yun Ko): Surgery, Supervision, Final approval of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by grants from the National Science and Technology Council, Taiwan (NSTC 114-2314-B-037-074); Kaohsiung Medical University Gangshan Hospital (KMGH-113R004, KMGH-114-R011), Kaohsiung Medical University, Kaohsiung, Taiwan.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.