
Abstract
Objective:
To ascertain brachial-ankle pulse wave velocity (baPWV) and ankle-brachial index (ABI) and their usefulness as an additional indicator of idiopathic sudden sensorineural hearing loss (ISSNHL) etiology and prognosis.
Methods:
We retrospectively analyzed 89 adult patients with unilateral ISSNHL and 89 age-matched controls. Patients were classified into good- or poor-prognosis groups based on hearing recovery. All participants accepted the examinations of baPWV, ABI, and pure-tone audiometry testing. Other clinical variables were also collected. Multiple linear regression analysis was used to assess the associations between arterial stiffness factors and pure-tone average; univariate logistic regression was used to evaluate predictors of prognosis.
Results:
ISSNHL patients showed significantly higher baPWV than controls (P < .001). Elevated baPWV was associated with increased air-conduction (β = .244, P = .040) and bone-conduction threshold (β = .286, P = .014), and was also associated with poor prognosis (P = .015).
Conclusions:
BaPWV was related to the incidence of ISSNHL and may serve as a useful indicator of disease severity. Its potential relevance to hearing outcomes requires further validation in larger prospective studies.
Keywords
Introduction
Idiopathic sudden sensorineural hearing loss (ISSNHL) is an abruptly appearing hearing loss occurring within a short time, which is considered an otolaryngological emergency, and that persistence seriously affects patients’ quality of life. A 2013 study reported that the estimated incidence of ISSNHL in the USA was 11 to 77 per 100 000 people annually. 1 Recent epidemiological investigations showed that the incidence of ISSNHL has exhibited a consistent upward trajectory over the years. 2
The exact causes of ISSNHL remain unclear. Reports presented potential causes include vascular disorders, 3 viral infections, 4 and autoimmune, 5 among others. In recent years, vascular disorders are considered as the primary cause of ISSNHL, as the inner ear is exclusively supplied by 1 or 2 labyrinthine arteries arising from the anterior inferior cerebellar artery. 6 Besides, some studies showed a positive association between ISSNHL and stroke, which further supporting the potential vascular pathogenesis.7,8
Arterial stiffness leads to global cerebral vascular injury, including small and medium-to-large arteries, and reduces brain perfusion. 9 The ankle-brachial index (ABI) and pulse wave velocity (PWV) are widely used noninvasive modalities to evaluate arterial stiffness. PWV is one of the most established indexes for evaluating arterial stiffness. PWV can be measured between 2 sites along an arterial tree, such as aortic PWV, carotid-femoral PWV, or brachial-ankle pulse wave velocity (baPWV), with higher values indicating stiffer arteries. 10 The ABI is the ratio of systolic blood pressure measured at the ankle to that measured at the brachial artery in the arms by Doppler. Previous studies have reported that the ABI and baPWV potentially reflect cerebrovascular risk in normal subjects. People with low ABI values have a significantly greater risk of developing future stroke than subjects with normal values, 11 and baPWV has been shown to be related to silent cerebral infarction and intracranial stenosis.12,13 However, ABI and baPWV, as the measurement of arterial stiffness, their role in ISSNHL has rarely been described. In this study, therefore, we investigated the clinical significance of ABI and baPWV in the development and prognosis of idiopathic ISSNHL. Because hypertension, diabetes, and dyslipidemia can potentially accelerate the process of ISSNHL, 14 our study eliminated the impact of the aforementioned factors in order to enhance the reliability of the outcomes.
Patients and Methods
Participants
The current retrospective study collected 89 patients (cases) with diagnosed ISSNHL and 89 healthy volunteers at the Otolaryngology Department between September 2023 and 2025. Controls were healthy volunteers without otology or neurological disorders who matched for age (±3 years) and gender of the patients. The diagnostic criteria of ISSNHL according to the American Academy of Otolaryngology—Head and Neck Surgery Foundation’s guidelines 2 and the Guidelines for sudden deafness established by the Chinese Society of Otolaryngology—Head and Neck Surgery 15 were adopted. The diagnosis was based on the patient’s medical history and clinical examination. The inclusion criteria of patients were as follows: (1) sudden onset of sensorineural hearing loss of ≥30 dB over 3 consecutive frequencies that occurred within 72 hours; (2) no identifiable cause despite adequate investigation; (3) first onset of illness without having undergone any treatment; (4) retro-cochlear pathologies were excluded by a head magnetic resonance imagingn (MRI). Exclusion criteria of patients included (1) known etiologies for hearing loss, including acoustic trauma, ototoxicity deafness, noise-induced deafness, acoustic neuroma, and other middle ear and inner ear diseases; (2) a previous history of otology or neurological diseases; (3) bilateral and recurrent ISSNHL.
All ISSNHL patients received high-dose steroid therapy. Dexamethasone was given in intravenous of 10 mg per day for 3 days, and extended for another 2 days if effective; combined with extract of ginkgo biloba leaves extract injection 87.5 mg per day for 10 days. Intratympanic steroid injection was used for the salvage treatment.
Data Collection
All participants provided demographic data (age, gender) and underwent comprehensive clinical assessments, including medical history review (hypertension, diabetes), physical examination with body mass index (BMI) measurement, and laboratory tests for total cholesterol (TC), triglycerides. Audiological evaluation, including pure tone air conduction (AC) and bone conduction (BC) threshold testing, was performed. BaPWV and ABI were additionally recorded. This research was carried out in the Department of Otolaryngology with the ethics committee’s approval. Informed consent was obtained from all participants.
Audiological Evaluation
All patients before and after treatment, as well as the control group, received pure-tone audiometry testing. The testing assessed thresholds of AC and BC at frequencies of .25, .5, 1, 2, 4, and 8 kHz. To quantify the hearing levels of patients and controls, the pure-tone average (PTA) was introduced, termed as the arithmetic mean threshold at 0.5, 1, 2, and 4 kHz. The level of hearing recovery was classified dependent on multicenter clinical study of sudden deafness in Chinese typing treatment 16 : complete recovery, defined as the average hearing threshold improvement of the affected frequencies to normal level (PTA ≤ 20 dB) or to pre-illness level (the self-reported hearing level before onset); marked improvement, PTA improvement ≥30 dB; slight improvement, 15 dB ≤ PTA improvement <30 dB; and no recovery, PTA improvement <15 dB. We defined good prognosis as complete recovery and marked improvement; poor prognosis was defined as slight improvement and no recovery.
Brachial-Ankle Pulse Wave Velocity
BaPWV was measured using the device of the fully automatic arteriosclerosis tester (BP-203RPEⅢ, Omron, Matsusaka, Japan). The participants were positioned in a supine position in a quiet room, and pressure sensor cuffs were placed on the brachial arteries of both upper arms (the lower edge of the cuff was 2-3 cm from the horizontal line of the cubital fossa) and the posterior tibial artery of both ankles (the lower edge of the cuff was 1-2 cm above the medial malleolus). The sampling time was 10 seconds. The device could automatically calculate the distance between the sensors based on the data of the participants’ height, and calculate the 2-sided baPWV values. The higher baPWV values were used for subsequent analysis.
Ankle-Brachial Index
ABI was measured using the same method as baPWV. ABI is the ratio of the highest systolic pressure of both ankle arteries divided by the highest systolic pressure of both brachial arteries. ABI can be calculated simultaneously when measuring baPWV. An ABI value between .9 and 1.4 is considered normal. Values below .9 suggest the presence of peripheral arterial disease, while values above 1.4 suggest the possibility of arterial calcification. 17
Statistics
Statistical analysis was performed with SPSS 25.0 (IBM Corp, Armonk, NY, USA). Continuous variables were reported as mean ± standard deviation (SD), medians and interquartile ranges. Categorical variables were expressed as numbers and percentages. As for statistical comparisons between groups, we used an independent t-test for continuous variables that followed a normal distribution. The nonparametric Mann–Whitney U test was applied to continuous variables that deviated from a normal distribution. Chi-square analysis was applied to categorical variables. Multiple linear regression analysis was used to evaluate the impacts of baPWV and ABI on PTA, controlling for confounding variables. Univariate logistic regression analysis was used to identify factors associated with prognosis. An receiver operating characteristic (ROC) curve was constructed to assess the predictive effect of positive factors. A P-value of <.05 was considered statistically significant.
Results and Analysis
Characteristics of Patients with Participated
A total of 89 patients with unilateral ISSNHL and 89 controls were included in the present study. The demographic characteristics and clinical data of all participants are shown in Table 1. Patients with ISSNHL had a mean (SD) age of 51.70 (13.85) years, and most of them were female (60.7%). Most affected ears of patients were on the left side (51.7%). Controls had a mean (SD) age of 51.70 (13.70) years, and women accounted for 59.6%. No significant statistical difference was found between age, gender, side of affected ears, hypertension, diabetes, BMI, lipid profile, or ABI on the patients and the controls (P > .05). PTA in affected ears and baPWV were significantly higher in patients than in the controls (P < .001). There was no difference between PTA in unaffected ears and in the controls (P > .05).
Demographic Characteristics and Clinical Data of Patients with ISSNHL and Controls.
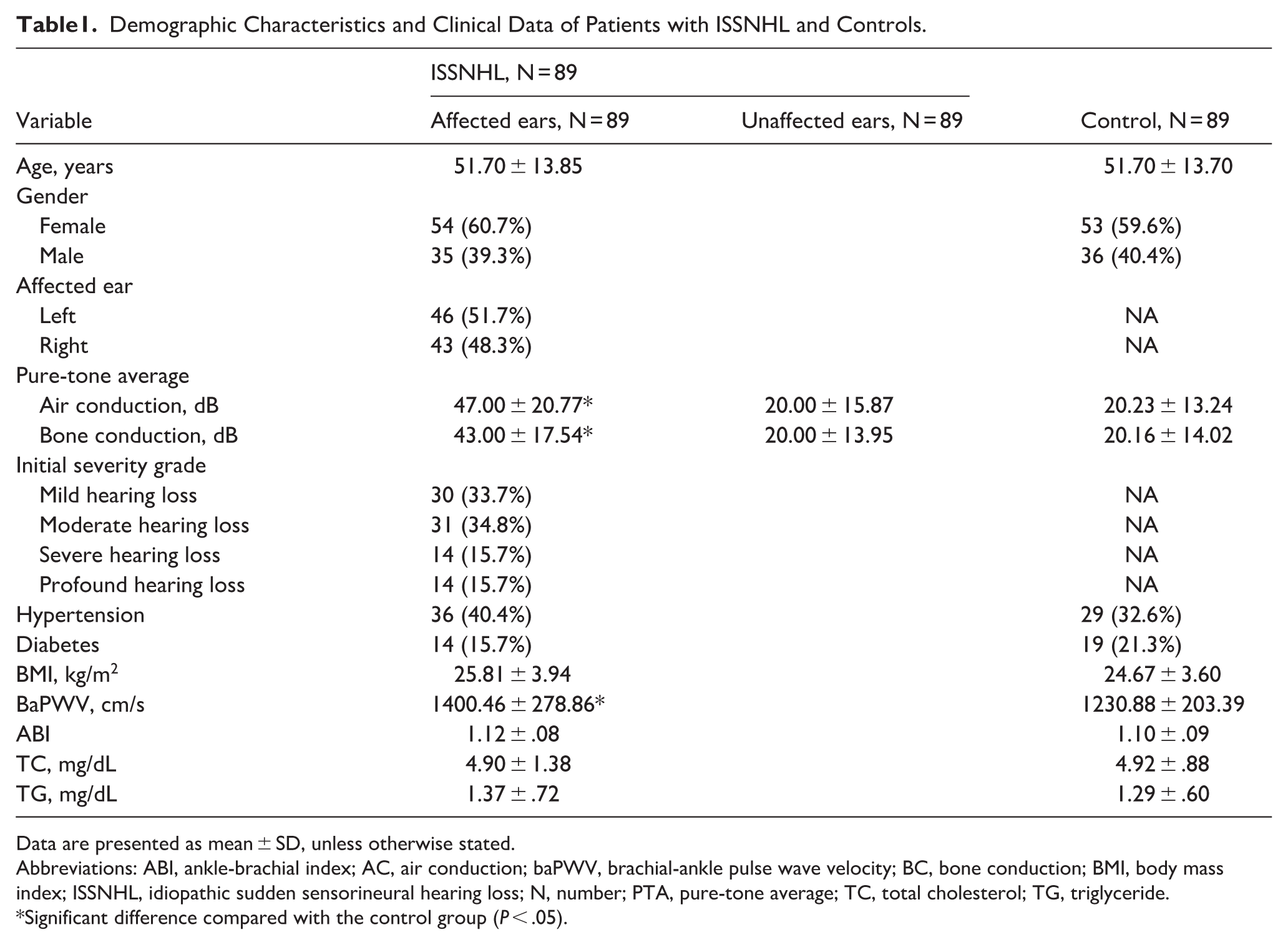
Data are presented as mean ± SD, unless otherwise stated.
Abbreviations: ABI, ankle-brachial index; AC, air conduction; baPWV, brachial-ankle pulse wave velocity; BC, bone conduction; BMI, body mass index; ISSNHL, idiopathic sudden sensorineural hearing loss; N, number; PTA, pure-tone average; TC, total cholesterol; TG, triglyceride.
Significant difference compared with the control group (P < .05).
Impact of Arterial Stiffness on PTA of Patients
In the models (Tables 2 and 3), we assessed the effects of factors on AC and BC thresholds in patients with ISSNHL, respectively. In Tables 2 and 3, the variance inflation factors test with its largest value of 1.531 indicates that there is no multicollinearity problem in the regression model. An F test was performed on both models. The F values were 5.868 in Table 2 and 6.736 in Table 3, and the P-values were both less than .05, indicating that factors affect the AC and BC thresholds in patients with ISSNHL. As presented in Tables 2 and 3, patients with a higher baPWV have higher AC threshold (β = .244, P = .040) and higher BC threshold (β = .286, P = .014). The older age was also independently associated with higher AC threshold (β = .306, P = .006) and higher BC threshold (β = .353, P = .001). No statistical correlation was found between gender, BMI, lipid profile, hypertension, diabetes, or ABI with PTA in patients with ISSNHL (P > .05). A multivariate linear regression analysis was performed for the healthy control group, but no significant statistical correlation between baPWV values and PTA thresholds (P > .05).
Multivariate Linear Regression Results of AC in the Affected Ear.
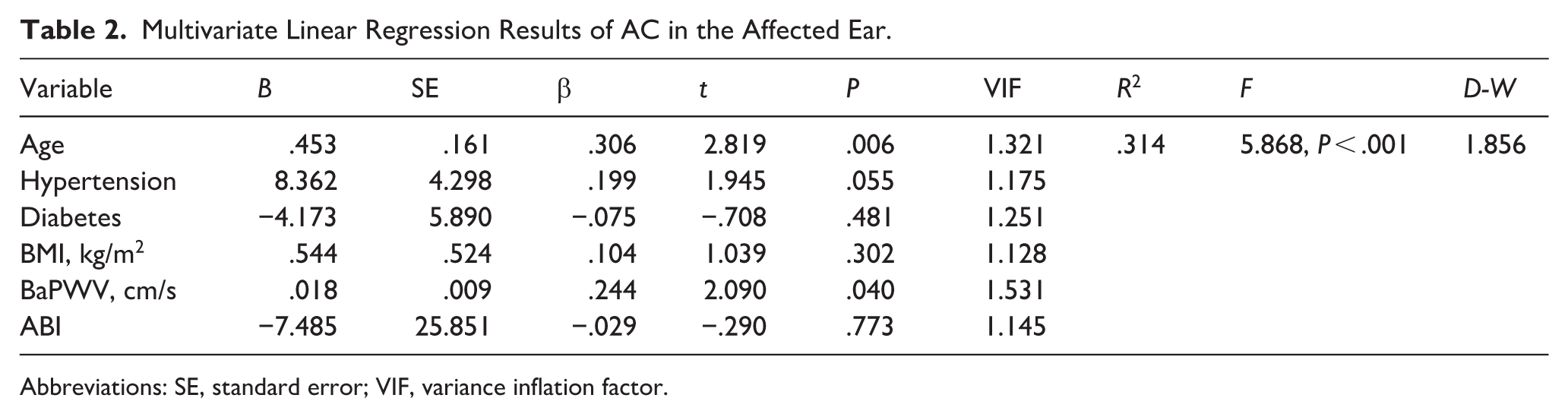
Abbreviations: SE, standard error; VIF, variance inflation factor.
Multivariate Linear Regression Results of BC in the Affected Ear.
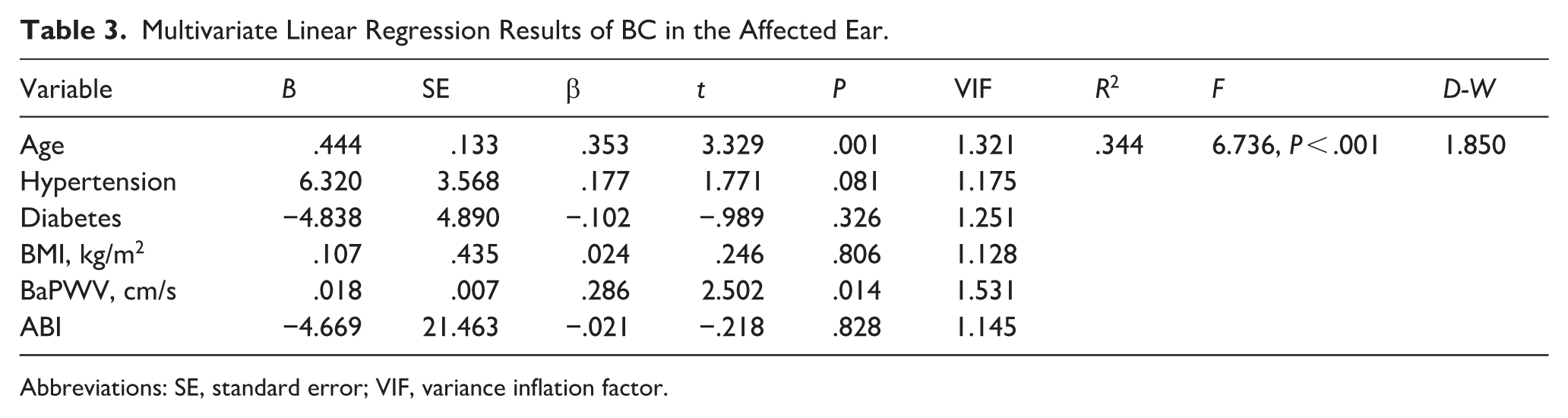
Abbreviations: SE, standard error; VIF, variance inflation factor.
Indicators of Prognosis
The patients were divided into 2 groups: good prognosis and poor prognosis, according to the hearing recovery. The characteristics of 2 groups are showed in Table 4. Among good prognosis group, 28 were complete recovery and 2 were marked improvement, whereas in the poor prognosis group, 17 were slight improvement and 42 were no recovery. The poor prognosis group were older (P = .003), had higher baPWV (P = .001), worse initial hearing threshold (P = .001, P = .004), and more cases of diabetes mellitus (P = .019) and hypertension (P = .005). In univariate logistic regression analysis, age (P = .001), baPWV (P = .008), initial hearing threshold (P = .003, P = .007), and hypertension (P = .007) were associated with poor prognosis in ISSNHL patients. ROC curves (Figure 1) suggested that age showed better predictive performance among the evaluated factors (AUC = .764), while baPWV (AUC = .714) had a comparable predictive value to the initial AC threshold (AUC = .718). Hypertension showed an AUC of .654. There was no significant correlation between gender, the initial severity, lipid profiles, BMI, and ABI to prognosis.
Demographic Characteristics and Clinical Data of Good and Poor Prognosis Groups.
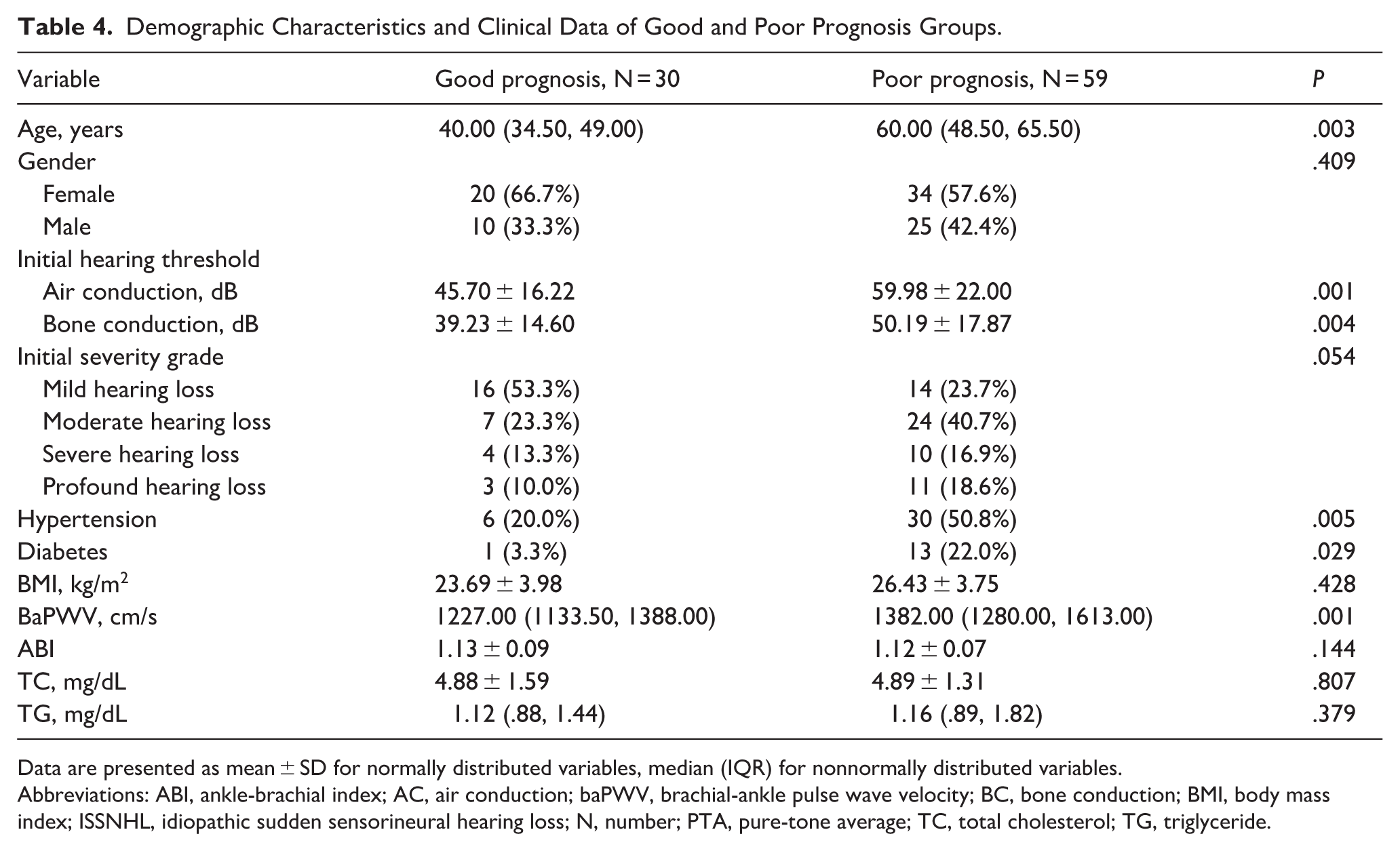
Data are presented as mean ± SD for normally distributed variables, median (IQR) for nonnormally distributed variables.
Abbreviations: ABI, ankle-brachial index; AC, air conduction; baPWV, brachial-ankle pulse wave velocity; BC, bone conduction; BMI, body mass index; ISSNHL, idiopathic sudden sensorineural hearing loss; N, number; PTA, pure-tone average; TC, total cholesterol; TG, triglyceride.
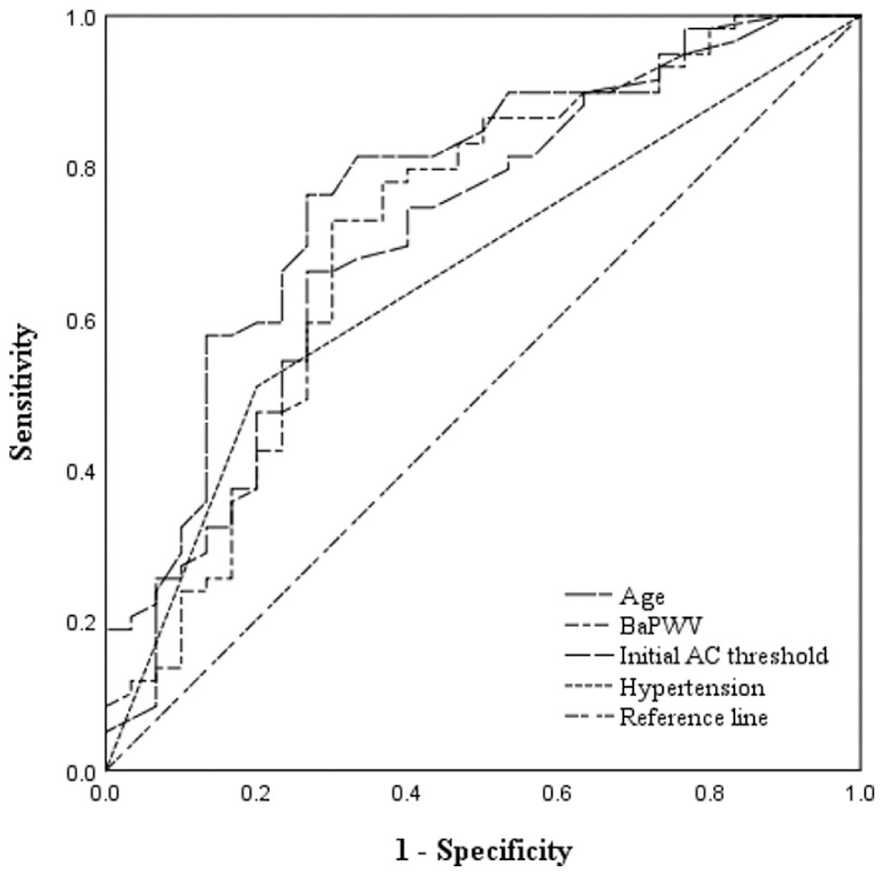
ROC curves for factors in predicting prognosis of ISSNHL.
Discussion
Although the pathogenesis of ISSNHL still remains unknown, a hypothesis has been proposed suggesting that cochlear microcirculation disorder may underlie the various triggering conditions. 18 Given that arterial stiffness precipitates widespread cerebrovascular injuries, which encompass small arterioles and medium-to-large arteries, and concomitantly diminishes brain perfusion, 9 it may play a key determinant in the pathogenesis of circulatory impairment in the inner ear. In our study, we intended to measure the effects of baPWV and ABI, which reflects arterial stiffness, on the incidence, severity, and prognosis of ISSNHL. Aiming to generate reliable results, we excluded the effects of clinical factors such as gender, BMI, hypertension, diabetes, and dyslipidemia on ISSNHL. The main findings were summarized as follows: (1) ISSNHL patients exhibited significantly higher baPWV values compared to the control group; (2) Higher baPWV values were significantly associated with higher thresholds of PTA in ISSNHL patients; (3) While elevated baPWV might be associated with a poorer prognosis in ISSNHL patients, its prognostic value should be interpreted together with older age, hypertension, and initial hearing threshold; (4) No significant correlation was observed between ABI and the incidence, severity, and prognosis of ISSNHL patients.
Special emphasis should be placed on our conclusion that a positive correlation existed between arterial stiffness and the onset of ISSNHL, 19 which is consistent with prior studies. For instance, it was confirmed that atherogenic index (ATH index) was higher in ISSNHL patients. 20 A previous study employed intima-media thickness (IMT) of the common carotid artery (CCA) as a surrogate marker for arterial stiffness and reported a greater prevalence of high-IMT (≥.65 mm) among individuals in the ISSNHL group. 21 Moreover, in a retrospective study that compared ISSNHL patients and healthy controls, Mutlu et al 22 discovered that the IMT values of the CCA and internal carotid artery markedly increased in the ISSNHL group relative to the control group. Our findings also demonstrate that higher baPWV values were positively correlated with increased severity of ISSNHL, consistent with what has been concluded in past studies. A study performed in Japan used cardio-ankle vascular index (CAVI) as an indicator of arterial stiffness, with patients being divided into high-and-low CAVI groups. A retrospective analysis of the data from both groups led to the conclusion that the degree of ISSNHL in the high CAVI group tended to be higher compared to the low CAVI group. 23 Another study similarly confirmed that estimated PWV is positive associated with poorer initial hearing threshold. 24 Our study provides further evidence of a potential correlation between arterial stiffness and ISSNHL, suggesting the utility of arterial stiffness as a potential predictor of ISSNHL severity.
In the exploratory prognostic analysis, both age and initial hearing thresholds were significantly associated with prognosis, consistent with previous studies. 25 Similarly, hypertension was found associated with poorer hearing outcomes, in accordance with prior reports. 26 Hypertension can induce malfunction of the stria vascularis, such as the decrease in the cochlear oxygen partial pressure, 27 a reduction of maximum cochlear potential-intensity values, 28 and disturbance of the ionic K + recycling, 29 which may further impair cochlear perfusion and result in poor hearing recovery.
In addition to traditional vascular risk factors, Seo et al 24 reached a similar conclusion to ours, proposing a relation between higher estimated PWV and poor hearing recovery of SSNHL. Similar findings were also reported by Düzer et al 30 who found that the concentration of anti-HSP70 was notably higher than that in patients with poorer prognosis, suggesting that endothelial dysfunction might be associate with the prognosis of ISSNHL. While diabetes showed a significant difference in group comparison but not in regression, this might be partly attributed to the limited number of diabetic cases. Nevertheless, diabetes remains an established vascular risk factor. Hyperglycemia can induce the narrowing of the capillaries in the stria, which may further impair cochlear perfusion and result in poor hearing recovery. 31 Notably, these vascular risk factors are closely interconnected and collectively reflect an elevated vascular burden, rather than the influence of a single isolated factor. Therefore, it is clinically important to control blood pressure and other vascular risk factors, which may help improve cochlear perfusion and optimize treatment outcomes.
Admittedly, several limitations of this study should be noted. First, only baPWV and ABI were used as indicators of arterial stiffness, while cfPWV was not measured in this investigation due to the operator-unfriendly nature of standard existing techniques. The future studies are expected to include additional indicators of arterial stiffness (e.g., cfPWV) that produce concrete evidence to reveal the associations between arterial stiffness and ISSNHL. Second, given the relatively small sample size, the prognosis findings should be considered exploratory. Consequently, future research could expand cohorts and establish standardized protocols to enhance the robustness of the findings.
Conclusion
The study revealed that a positive association exists between baPWV and the incidence and severity of ISSNHL. It suggested a potential link between arterial stiffness and ISSNHL. Monitoring and improving vascular health, particularly the management of arterial stiffness, may be crucial for preventing the further development of ISSNHL.
Footnotes
Author Contributions
Rui Song: Writing – original draft, Visualization, Investigation, Formal analysis. Chunhua Hu: Writing – review & editing, Methodology, Data curation. Yanjun Feng: Resources, Investigation. Jingfan Wang: Investigation. Zhan Yu: Funding acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key R&D Program of China (2020YFC2005200); and Wu Jieping Medical Foundation Special Fund for Clinical Research (320.6750.2024-03-12).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.