
Abstract
Background:
Congenital pyriform fossa malformations (CPFM) are rare types of branchial anomalies. The management approach was previously anatomical, based on outlining the complete surgical excision of the vestige tract. Endoscopic obliteration of the pharyngeal opening of the tract evolved as an alternative to less invasive treatment. Although different techniques have been reported, long-term follow-up data are relatively deficient.
Methods:
This is a retrospective analysis of patients with CPFM treated in a tertiary referral hospital. Direct laryngoscopy was the only diagnostic method used. Endoscopic radiofrequency ablation was done as described. Patients with at least 24 months of follow-up were included.
Results:
Fourteen patients met inclusion criteria, 10 males and 4 females, with a mean age of 8 years. Only one patient had an external cervical component. All patients had the pharyngeal opening in the left pyriform fossa except for one. Average follow-up period was 41.5 months. No complications or recurrences were reported during the follow-up period.
Conclusion:
Endoscopic radiofrequency cauterization can be described as a safe, effective sole treatment of CPFM. The approach we adopted is simple, less demanding with long-term reliability.
Introduction
Third and fourth branchial cleft anomalies represent only 2% to 8% and 1% of the brachial malformations, respectively; however, they may present with significant morbidity due to deep neck infections. 1 These anomalies result from aberrant embryologic development and persistence of epithelial-lined tracts, leading to cysts, sinuses, or fistulas. 2
The most common presentation of third and fourth brachial cleft anomalies is acute suppurative thyroiditis or neck abscess, usually without pre-existing neck swelling or an external opening.2 -4 This is presumably associated with a sinus tract with a pharyngeal opening being the portal for organisms causing infection. With non-pathognomonic presentation, misdiagnosis or delayed diagnosis is common, and recurrence of infection usually occurs after non-specific management.2,3
Although the embryologic tracts of third and fourth branchial cleft sinuses differ anatomically, both share an internal opening in the pyriform fossa. 5 With more attention paid to the pharyngeal opening, third and fourth branchial sinuses have been collectively termed congenital pyriform fossa malformations (CPFM) or equivalent nomenclatures.3,5 -7
Due to the rarity of CPFM, standardized management guidelines are lacking. Open surgical excision of the whole embryological tract was considered the standard treatment. This is associated with variable rates of surgical complications including recurrent laryngeal nerve injury, infection, and scarring, with variable success rates.2,3,8,9
Jordan et al 10 first reported endoscopic cauterization of the internal opening of the fourth branchial cleft sinuses; since then, multiple studies have explored endoscopic techniques using various modalities, often with short-term follow-up.6,7 Recurrence of infection after endoscopic treatment is presumed to be due to recanalization of the cauterized internal opening, which may occur months or years later.
We aimed to evaluate the long-term outcomes of endoscopic radiofrequency ablation for CPFM with a simple diagnostic approach and purely endoscopic treatment strategy.
Patients and Methods
We performed a retrospective review of clinical data of patients diagnosed with CPFM and managed in the Department of Otolaryngology-Head and Neck Surgery, Tanta University, Egypt, between July 2019 and January 2023.
The inclusion criteria were:
Patient presented with history of neck infection/suppurative thyroiditis “regardless of number of attacks” typical for infected CPFM.
Established diagnosis of CPFM by identification of a pharyngeal opening in the pyriform fossa by direct laryngoscopy with or without associated external skin components.
Patients underwent radiofrequency ablation of diagnosed CPFM in our department.
Patients who were followed up for at least 2 years after treatment.
Patients were excluded if documentation of endoscopic findings was incomplete, if they were lost to follow-up, or if follow-up duration was <2 years.
Patient demographic data, clinical presentation, investigation, management, hospital stay, and follow-up period were recorded. The study protocol was approved by the local ethical committee (approval No 36264PR844/9/24).
During the acute phase, all patients received intravenous antibiotics, analgesia, and anti-inflammatory medications. Ultrasound and/or contrast-enhanced CT were performed. Patients without or with small collection were treated medically. A collection larger than 2 ml was an indication for ultrasound-guided aspiration or incision and drainage (I&D) under general anesthesia (Figure 1). After 4 to 6 weeks of resolution of the last attack of acute infection, patients were listed for suspension direct laryngoscopy. Patients’ guardians were informed that this was primarily a diagnostic procedure, with consent for immediate intervention if indicated.
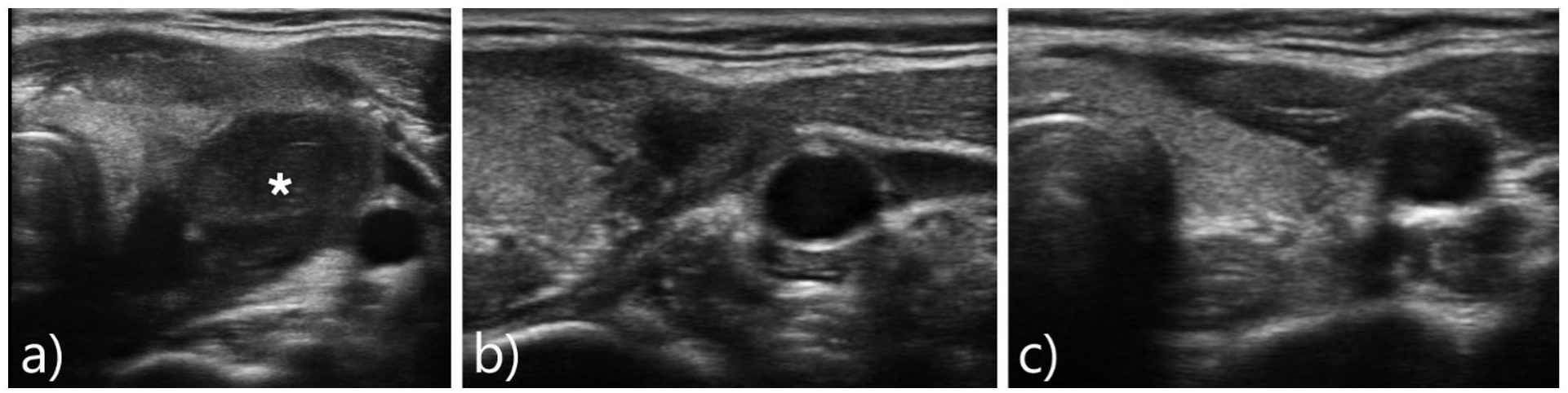
Neck ultrasound of a patient with CPFM presented with acute neck swelling showing (A) abscess collection involving left thyroid lobe (asterisk). (B) Collapse of the abscess cavity after ultrasound-guided aspiration. (C) Complete resolution 3 months after endoscopic cauterization with normal appearance of left thyroid lobe. CPFM, congenital pyriform fossa malformations.
Operative Technique
All patients were treated under general anesthesia with orotracheal intubation. In our approach, an anterior commissure laryngoscope with the proper size (for the patient’s age) was used to spread open the pyriform fossa on both sides. Both pyriform fossae were inspected with 5 mm, 0-degree telescope.
Once the internal opening was identified, the suspension was installed for full exposure of the opening and the Betz fold (Figure 2). For sinus and pharyngeal opening cauterization, we used high-frequency radio wave electrosurgical generator, Ellman Surgitron Dual RF unit (Ellman International, Inc, Hewlett, NY, USA) with medium power setting of 5 (of 9), coagulation mode. The radiofrequency energy was applied by Steiner insulated suction coagulation cannula (Karl Storz, Tuttlingen, Germany) with a 2-mm tip. The suction cannula was gently pushed into the pharyngeal opening as far as resistance was encountered. Monopolar radiofrequency energy was then applied inside and then to the surface of the pharyngeal opening with minimal involvement of the surrounding mucosa (5 mm of blanching mucosa around) (Figure 3).
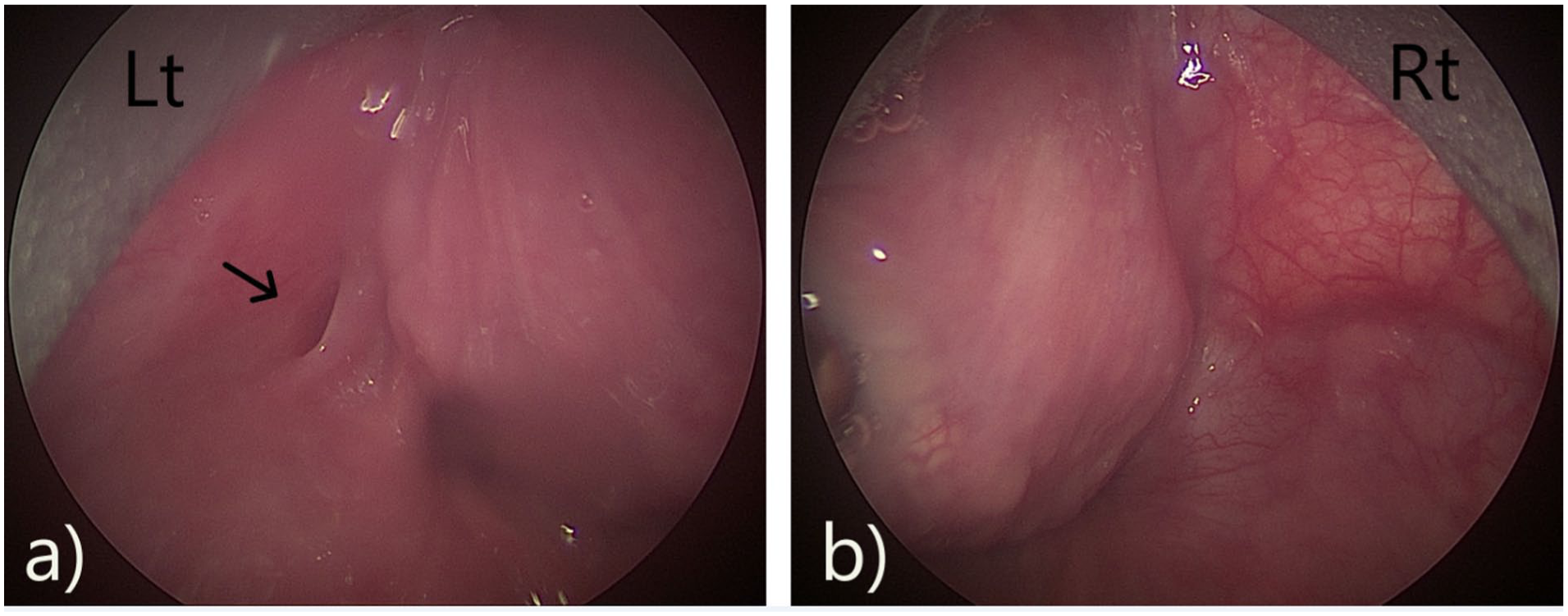
Direct laryngoscopy view. (A) Sinus opening in the left pyriform fossa with Betz fold (black arrow). (B) Normal right pyriform.
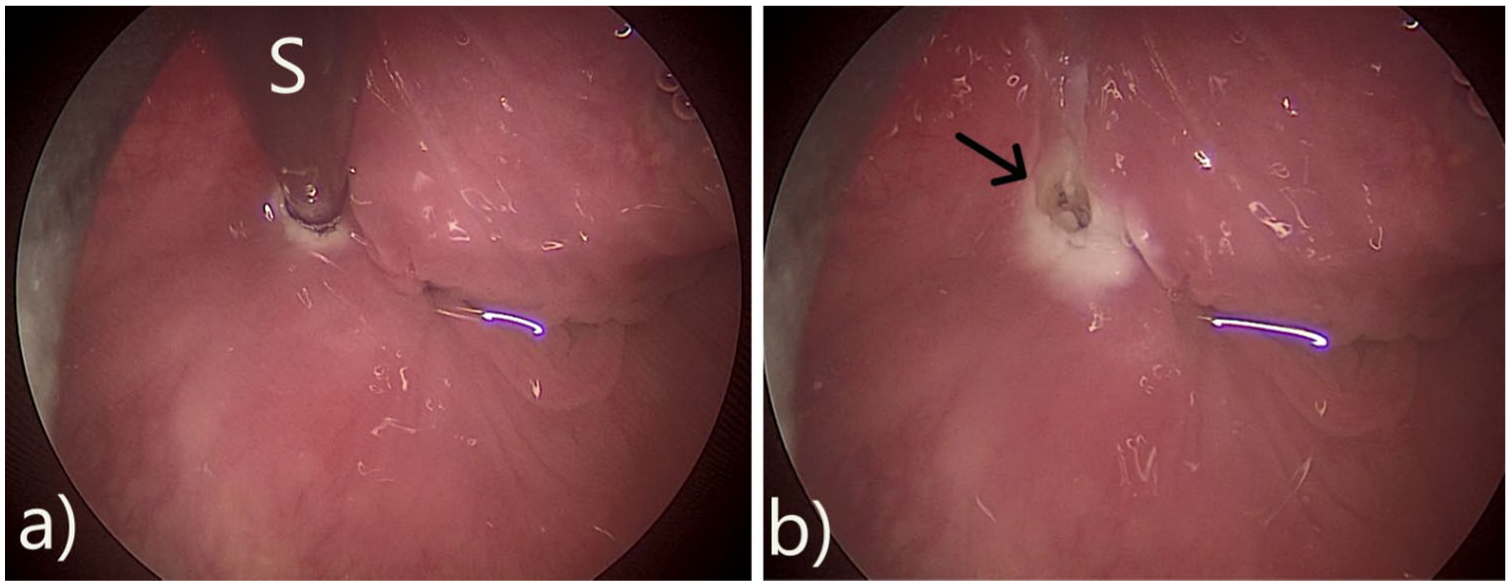
Endoscopic view of the left pyriform fossa. (A) Insertion of the suction coagulation cannula(s) into the sinus tract for cauterization. (B) Sinus opening after cauterization (black arrow).
All patients received perioperative intravenous antibiotics, steroids, and proton pump inhibitors. They were allowed oral liquids and a soft diet on the day of surgery and were discharged on a soft diet with oral continuation of treatment.
Patients were followed weekly for the first month, monthly during the first year, and every 6 months thereafter. The follow-up included history taking, clinical neck examination, and surgeon-performed ultrasound examination for any features of collection or thyroiditis (Figure 1). We advised patients to present to the outpatient clinic or emergency department at any time should symptoms indicative of acute neck infection occur.
Results
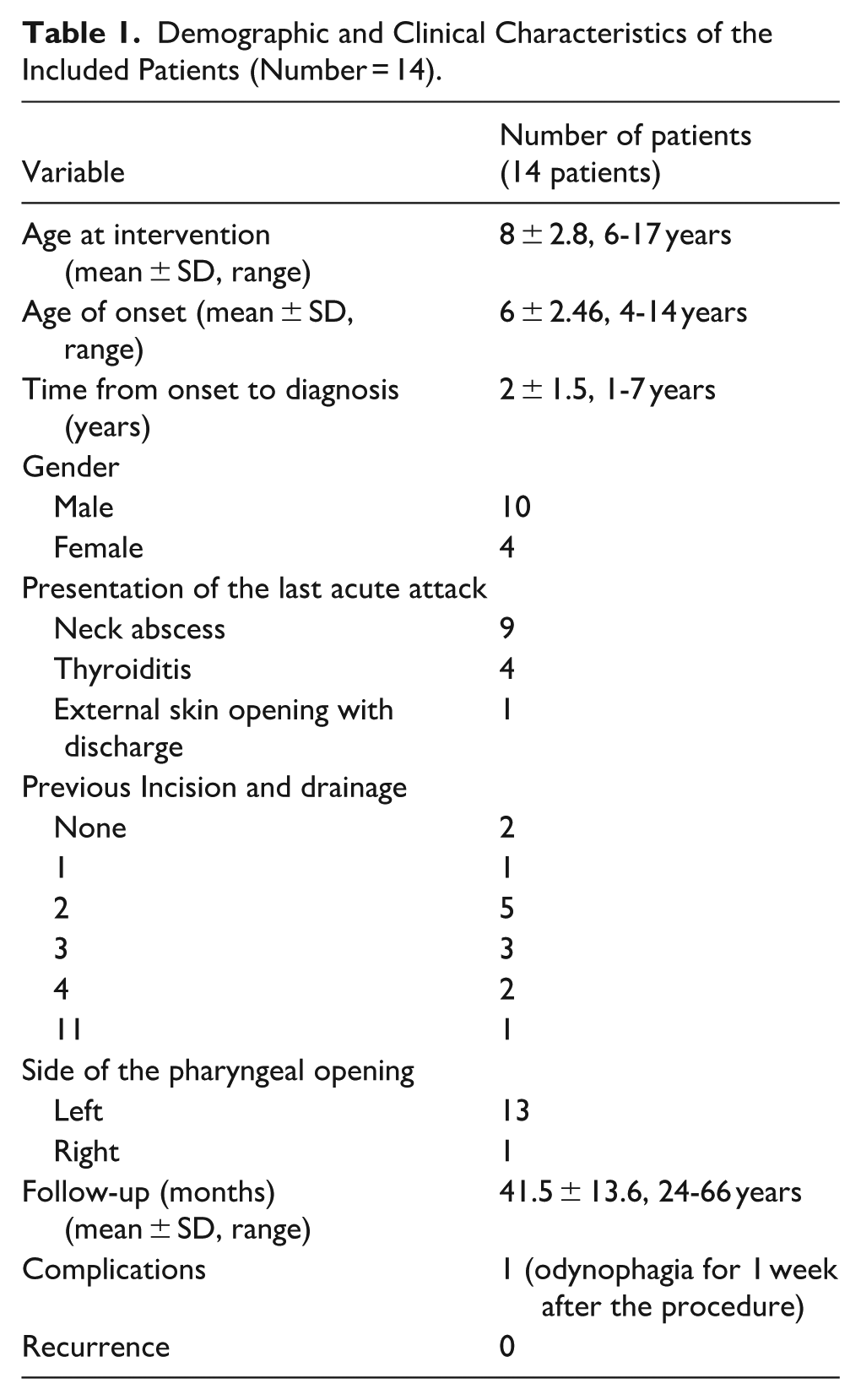
Twenty-three patients with CPFM were treated during the study period. Nine were excluded due to inadequate follow-up, leaving 14 patients (10 males, 4 females). Mean age at diagnosis was 8 years (range 6-17 years) (Table 1). All patients had a history of recurrent neck infections managed at multiple facilities before referral.
Demographic and Clinical Characteristics of the Included Patients (Number = 14).
All patients had neck ultrasound examinations, and 8 patients underwent contrast-enhanced CT scans during the assessment of the last attack of neck infection before diagnosis (Figure 4). Only 2 patients were managed medically without drainage. One patient had an external cervical opening with recurrent mucopurulent discharge (Figure 5); another had a history of recurrent thyroiditis localized to the left side. Twelve patients had undergone I&D of neck abscesses prior to presentation, with a mean of 2.5 drainage procedures (range 1-11). Four patients had neck collection drainage in our department by ultrasound-guided aspiration and two had formal I&D, as shown in Table 1.
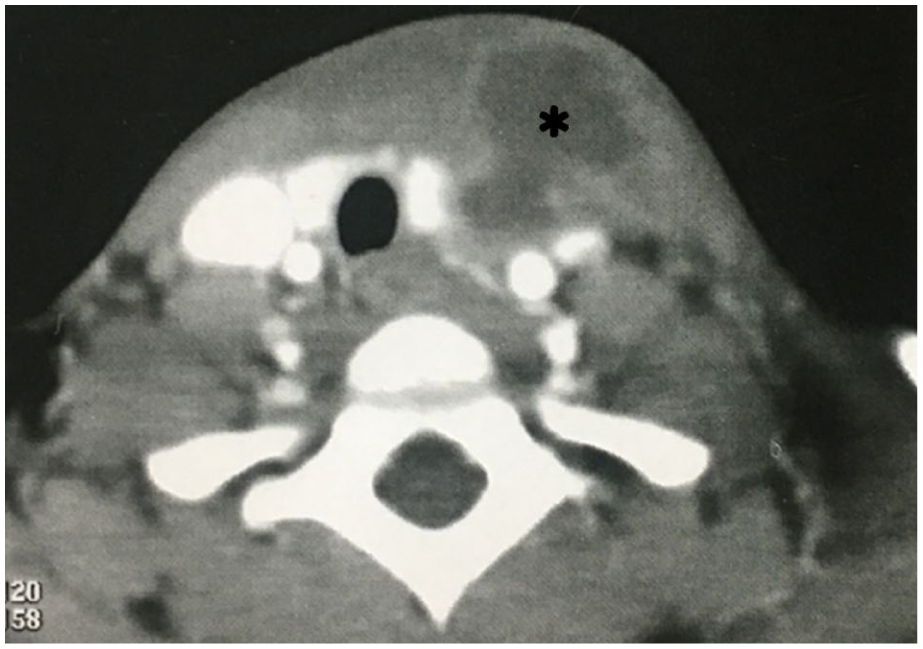
Contrast-enhanced CT of the neck, axial view, of a patient with CPFM presented with acute painful neck swelling. The scan shows a large hypodense collection with an enhanced rim involving the left thyroid lobe (asterisk). CPFM, congenital pyriform fossa malformations.

A patient with CPFM with external skin component. CPFM, congenital pyriform fossa malformations.
Direct laryngoscopy identified the pharyngeal opening in all patients, with typical Betz fold. Thirteen had left-sided openings; one was right-sided. Mean interval between first infection and diagnosis was 2 years (range 6 months to 7 years).
Twelve patients were discharged on the same day; two required overnight observation. One patient developed significant odynophagia for 1 week, resolving conservatively. Otherwise, no surgical complications were reported.
Mean follow-up was 41.5 months (range 24-66 months). One patient developed mild inflammatory symptoms during an upper respiratory infection 3 months postoperatively, with no evidence of collection by ultrasound examination. This was managed with simple oral antibiotics and anti-inflammatory medication and was not reported again during follow-up. No patient experienced recurrent infection comparable to preoperative episodes, and none required repeat endoscopy.
Discussion
The definitive management of CPFM has evolved over the last few decades. Early treatment strategies relied on extensive open surgery, including tract excision with or without hemithyroidectomy.5,11,12Although effective, these procedures pose risks including vocal cord paralysis, salivary fistula, wound complications, and significant scarring. 1
Nicoucar et al reviewed the management of third and fourth branchial anomalies in 2010 and 2009 respectively. They found that patients treated with open surgical excision with or without hemithyroidectomy were 5 to 6 times those treated endoscopically. The role of endoscopy in the management of CPFM graduated from confirming the diagnosis and guiding surgical excision to definitive treatment by cauterization/sealing of the pharyngeal opening of the sinus/fistula tract.1,10,11,13
Because a fully patent third or fourth branchial fistula extending to the skin is rarely encountered clinically, removal of the entire tract may not be necessary to terminate recurrent infections.5,10 Endoscopic closure of the pharyngeal opening of CPFM aims to prevent bacterial or food entry into the sinus tract, thereby reducing infection risk. 10 Endoscopic cauterization gradually gained popularity being safe, less demanding, cost-effective, and associated with recurrence rates comparable to or lower than open surgery.2,3,9
In this case series, we adopted a practical, minimally invasive approach rather than a holistic anatomical approach for the management of CPFM. For the management of acute infections, we opted for ultrasound assessment and guided aspiration of small collections to improve the cosmetic outcomes.
Diagnostic Considerations
Many imaging techniques were implicated in the diagnosis of CPFM and outlining the sinus tract in the quiescence stage. Magnetic resonance imaging (MRI) and barium swallow are the most frequently used with high positive predictive values.2,3,8 MRI was found to be more beneficial for assessment of the cystic component of the tract, which is uncommon and was not encountered in our case series.2,3 Ultrasound and CT findings are variable and often nonspecific. 13 Barium swallow, although considered to be the most useful tool, failed to demonstrate the sinus tract in many cases of reported series with sensitivity around 50% and 80% for third and fourth branchial cleft sinuses respectively.8,14 Specific timing, Valsalva maneuver, and using water-soluble contrast material were suggested to enhance sensitivity of contrast swallow studies.2,15 Negative findings of barium swallow did not affect the decision to do diagnostic direct laryngoscopy in patients with typical history suggesting CPFM in many case series.4,11,13,14,16 Based on these reported imaging findings, we relied on direct laryngoscopy alone, being the gold standard for diagnosis of CPFM.4,5,8,13 Also, outlining the course of the tract in positive imaging is irrelevant when endoscopic cauterization is planned as a primary treatment. Our simplified diagnostic algorithm—focusing on clinical history and direct laryngoscopy—reduced radiation exposure, cost, and delays without compromising diagnostic accuracy. We found the CPFM opening to be on the left in 92% of cases which is consistent with findings in the reported series.2,3,6,7
Comparison of Treatment Modalities
Chemical cauterization (silver nitrate, trichloroacetic acid) has been reported with variable success and non-standardized techniques.14,16 -19 Circumferential cauterization with trichloroacetic acid (TCA) was reported with a success rate of the first attempt around 75%.14,18,20 However, TCA concentration and frequency of application were not standardized, even changed within the same study.14,18 Recurrence has been reported after variable periods up to 5 years.18,20,21 In the management of recurrence, the sinus opening was found to have regained patency. 14 Temporary vocal cord paralysis was reported in 2 cases after chemo cauterization with TCA. 22 Although trickling of the chemical material into the sinus adds the advantage of obliterating a longer segment of the sinus tract, possible leakage into the esophagus may lead to dysphagia and risk of stricture.9,14
Although monopolar electrocautery was the first used for endoscopic treatment of CPFM, 10 we opted to use radiofrequency delivered to the depth of the sinus by an insulated suction catheter. Our method employs radiofrequency energy delivered through an insulated suction catheter, allowing controlled ablation along the tract while minimizing thermal injury to surrounding structures, particularly the recurrent laryngeal nerve.13,23
Different types of laser and coblation were used for endoscopic cauterization of the orifice of CPFM with good outcomes.4,6,7,24 Coblation represents a specific form of radiofrequency energy delivery that operates at lower tissue temperatures by generating a plasma field, resulting in more superficial tissue ablation with limited thermal spread. This technology has been utilized by Chen et al 6 to treat pyriform fossa sinus openings with the aim of minimizing collateral tissue injury. In contrast, the monopolar radiofrequency cauterization technique employed in the present study delivers higher thermal energy, allowing deeper coagulative effects and more definitive tract obliteration. While both approaches are endoscopic and minimally invasive, the differences in depth of penetration and tissue effect may influence long-term closure rates and recurrence, particularly in cases with well-formed or fibrotic tracts. LASER and coblation techniques are also inherently limited by availability, trained staff “for laser,” and cost.
Post-Operative Care and Follow-Up
Some protocols involve hospital admission, intravenous therapy, and nasogastric feeding for prolonged periods,4,6,7,18 though these measures have not been shown to reduce recurrence. 25 In our cohort, patients resumed oral feeding the same day and were discharged when adequate intake was confirmed.
Follow-up direct laryngoscopy was systematically performed by some surgeons around 4 to 6 weeks after the procedure to confirm closure of the sinus orifice and re-cauterize persistent sinuses.6,7,14 Few patients were found to have persistent sinus at this stage, and others with apparently closed sinus were not signed off regular clinical follow-up. Being done under general anesthesia, the cost-effectiveness of routine follow-up endoscopy is questionable.
Using cross-sectional imaging for follow-up was not reported. Cha et al stated that a CT scan may even still show the sinus tract after successful cauterization of the proximal part. 20 The follow-up in our study was mainly clinical, based on symptoms/signs suggesting recurrence of neck infection. We included a surgeon-performed neck ultrasound examination in the follow-up assessment for exclusion of any subclinical collection or thyroiditis (Figure 1). Neck ultrasound, being relatively inexpensive, quick, and radiation-free, was aligned with or time/cost-conscious approach as an objective tool for follow-up. Early symptoms were explained to the patients and their guardians with instructions to report to our service emergency and then to be brought to the attention of the management team.
Our long-term follow-up (mean 41.5 months) exceeds most published series, in which typical follow-up durations are 18 to 24 months.6,7,10,14,16,18 The durability of endoscopic results is best assessed over longer intervals because recanalization may occur several years after treatment.13,25 Lacking long-term outcomes was considered the main weakness in arguing the effectiveness of endoscopic cauterization of CPFM.13,25
Comparison to Other Studies
In a systematic review, the cumulative success of endoscopic cauterization after the first attempt ranged from 66.7% to 100%. 9 Recurrent infection after the first attempt was reported at around 25% for chemical cautery,18,20 2% for coblation, 6 and 44% for CO2 laser. 7 In our series, we did not encounter any recurrent infection that mandates re-endoscopy. Only one patient experienced mild inflammation of the neck that was resolved by simple medical treatment. This was described in other series and was not considered a recurrence.6,7 Another positive side of endoscopic cauterization is being “repeatable” if recurrence occurs without additional risk like with revision open surgery.
Chen et al 6 reported outcomes of 54 pediatric patients treated using endoscopic coblation, with no recurrences over 3 to 28 months. Our findings complement this by demonstrating similarly excellent results using radiofrequency, with the added strength of substantially longer follow-up (mean 41.5 months). Radiofrequency offers advantages of lower cost, wider availability, and deeper controlled ablation through an insulated probe.
Authors designed different algorithms for the management of CPFM according to age, tract anatomy, and previous infections.2,3,19 Based on literature experience, we developed a simple, cost-effective approach, identifying endoscopic radiofrequency ablation (ERFA) as the cheapest procedure for managing CPFM. We emphasize that our intention is not to claim superiority but to present long-term outcomes of a specific technique.
Study Limitations
The main limitations of this study are the small sample size and absence of a comparative group. Congenital pyriform fossa malformations is rare, and most published literature consists of small retrospective series. A randomized comparison is unlikely to be feasible. Endoscopic treatment is also not suitable for patients with restricted mouth opening or limited neck extension.
Conclusion
Endoscopic radiofrequency ablation for the congenital pyriform fossa malformations is a simplified, cost-conscious approach focusing on identification and endoscopic closure of the its pharyngeal opening. It offers a minimally invasive, resource-efficient treatment with excellent long-term outcomes and low morbidity. This strategy may be particularly suitable for healthcare systems prioritizing cost-effectiveness while maintaining high standards of care.
Footnotes
Ethical Considerations
The study protocol was approved by the local ethical committee (approval No 36264PR844/9/24).
Consent to Participate
Informed consent was obtained from all individual participants included in our study.
Author Contributions
All the authors including Mostafa Ammar, Mohamed O. Tomoum, Hazem Elbasty, and Ahmed S. Elhamshary contribute in the following: (a) substantial contributions to the conception, design of the work; and the acquisition, analysis, or interpretation of data for the work; (b) drafting the work and revising it critically for important intellectual content; (c) final approval of the version to be published; and (d) agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All the authors including Mostafa Ammar, Mohamed O. Tomoum, Hazem Elbasty, and Ahmed S. Elhamshary declare that they have no conflict of interest (financial or non-financial).
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.