
Abstract
Introduction:
Motion sickness (MS) has traditionally been attributed to visual-sensory mismatch. Research on the cause-and-effect relationship between postural instability and MS has emerged, although evidence remains scarce.
Methods:
A literature review from inception to December 31, 2024, was conducted to understand the relationship between MS and postural instability by searching several databases over a 1-month period in January 2025. The search was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. The included studies investigated various forms of MS, including car sickness, virtual reality (VR), simulator sickness, cybersickness, travel-related sickness, and space MS.
Results:
A total of 16 articles were identified, encompassing 1518 participants with ages ranging from 9 to 63 years. Most studies used force platforms and balance boards to assess postural instability, and 13 studies reported a relationship between postural instability and MS. These findings were consistent across VR, simulator, and transport-based motion paradigms. In contrast, 3 studies reported no consistent relationship between sway magnitude and symptom development.
Conclusions:
Although postural instability precedes MS, the quality of evidence is inadequate to determine the cause-and-effect relationship between MS and postural instability until extensive, multicentre, randomised controlled studies are conducted.
Keywords
Introduction
Motion sickness (MS) is a complex physiological response triggered by real or perceived motion, commonly presenting with symptoms such as nausea, dizziness, pallor, headache, and gastrointestinal discomfort. It can significantly impair daily functioning and quality of life, especially in children and adolescents who may be more susceptible due to their ongoing neurodevelopmental maturation.1 -4
The widely accepted Sensory Conflict Theory (SCT) explains MS as arising from a mismatch between signals received from the visual, vestibular, and proprioceptive systems. However, this theory has limitations in explaining individual susceptibility. An alternative framework, the postural instability theory (PIT), suggests that MS results when individuals are unable to maintain postural stability in response to a challenging environment.1,2 According to this model, prolonged instability is not merely a symptom but a causal precursor of MS. Several studies have been conducted to test this newer theory. However, we have noted that there are literature gaps which show inconsistent empirical support for PIT across modalities, the lack of pediatric-focused research, and the limited use of standardised diagnostic criteria (Bárány Society). This review aims to better understand and synthesize evidence on the association between MS and postural instability, evaluate methodological heterogeneity, and identify directions for future research.
Material and Methods
A systematic review of the literature was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline to identify studies that investigate the relationship between MS and postural stability.
Eligibility Criteria
We included studies investigating the relationship between MS and postural stability across all age groups. Conference abstracts, letters to editors, commentaries, review articles, publications without peer review, and grey literature were excluded. As the present evidence is limited, no restrictions on sample size are placed.
Exclusion Criteria
Non-relevant designs such as case reports and editorials, unretrievable reports, non-English publications, studies with a high risk of bias or insufficient methodological details, studies not reporting the primary or secondary outcomes defined in the reviews, and studies published outside the review period.
Data Sources and Searches
PubMed, Embase, and Scopus databases were searched to identify studies published from inception to December 31, 2024 using combinations of relevant terms relating to MS “motion sickness” OR “motion-sickness” OR “cybersickness” OR “cyber-sickness” OR “simulator sickness” OR “simulator-sickness” OR “visually induced motion sickness” OR “VIMS” OR “travel sickness” OR “sea sickness” OR “car sickness”) AND postural instability (“postural instability” OR “postural sway” OR “postural control” OR “postural stability” OR “balance” OR “center of pressure” OR “CoP” OR “sensory re-weighting”).
Only articles published in the English language were included. Complete details of the search strategy are in Figure 1. To ensure a robust search strategy, references of the included studies were included. We excluded duplicate studies using EndNote X8 software (Clarivate Analytics, Philadelphia, PA, USA). The search was conducted over a period of 1 month (January 2025) in accordance with PRISMA guidelines.
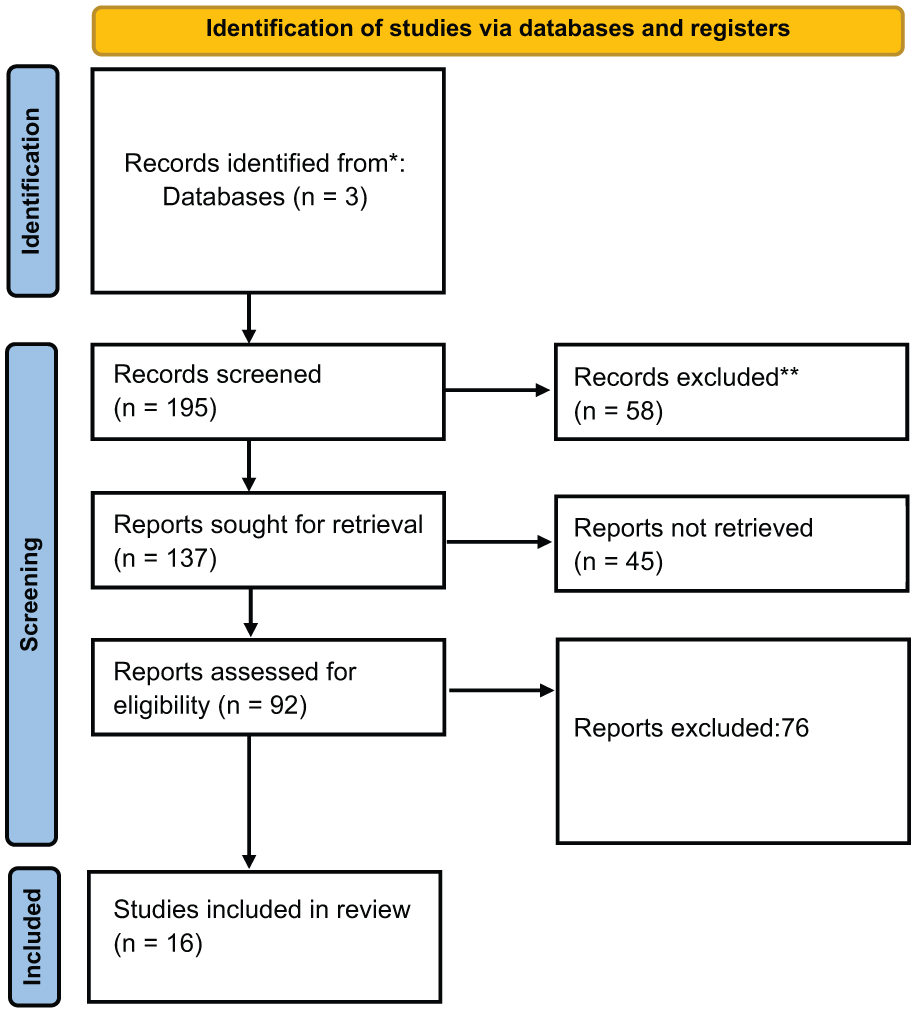
Search strategy.
Sixteen original clinical research articles were selected after being scrutinised by the panel members (L.R. and J.S). Any disagreements regarding the inclusion of articles were discussed and resolved by consensus.
Data extraction was done independently by 2 authors (L.R. and J.S.). We extracted the following information from each eligible study and entered it into a predefined Excel spreadsheet.
Ethical Consideration
The study was performed in accordance with ethical standards. The authors declare no conflict of interest.
Results
A total of 16 studies published from inception to December 31, 2024, were identified after an initial literature search, removal of duplicates, abstract screening, and full-text review, which met the inclusion criteria, as summarised in Table 1. All included studies were experimental or cross-sectional in design, except for 2 review articles.
Summary of Main Findings (Types of MS, Comorbids, Objective).
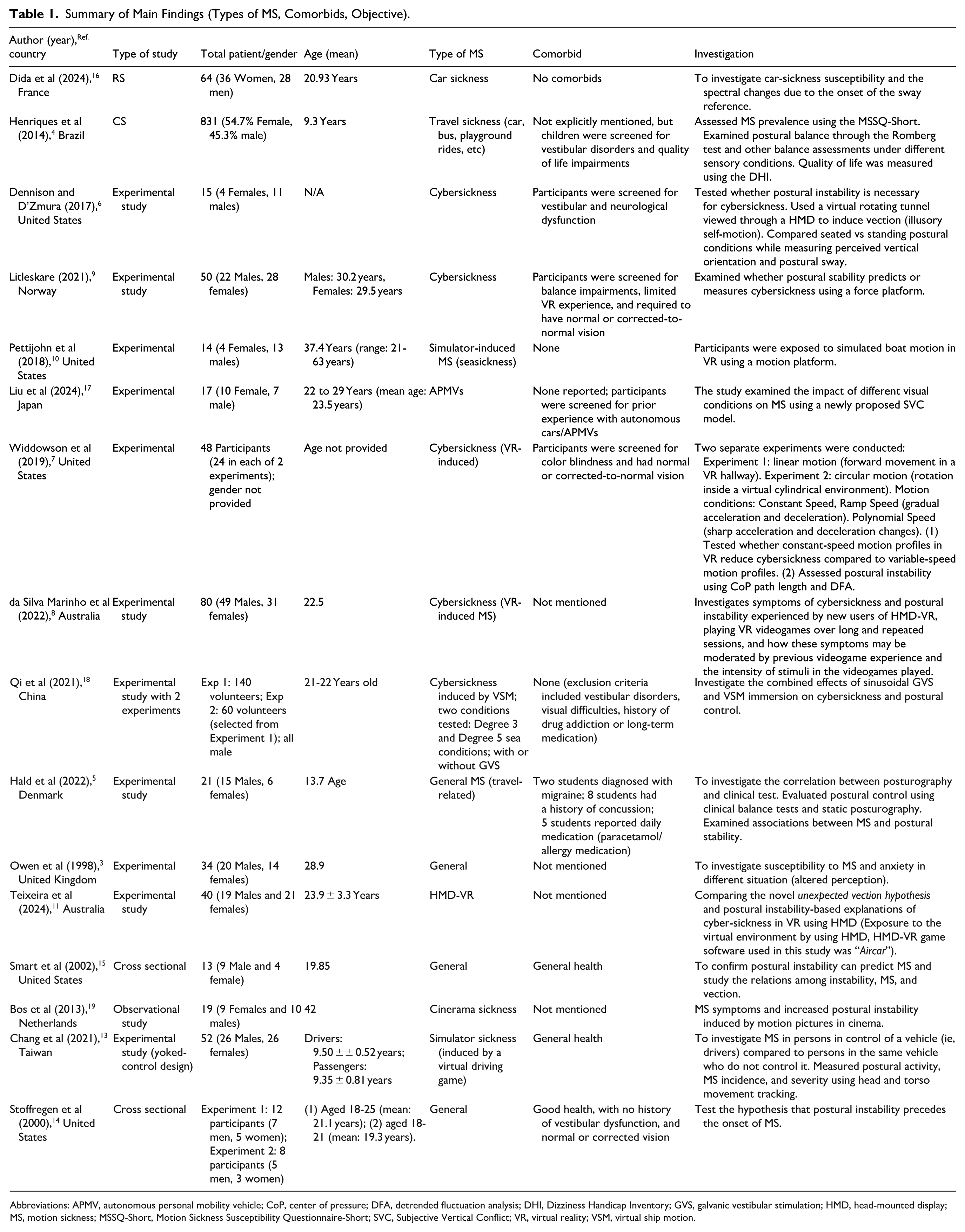
Abbreviations: APMV, autonomous personal mobility vehicle; CoP, center of pressure; DFA, detrended fluctuation analysis; DHI, Dizziness Handicap Inventory; GVS, galvanic vestibular stimulation; HMD, head-mounted display; MS, motion sickness; MSSQ-Short, Motion Sickness Susceptibility Questionnaire-Short; SVC, Subjective Vertical Conflict; VR, virtual reality; VSM, virtual ship motion.
Summary of Main Findings (Tests, Finding, Supporting Findings and Outcomes).
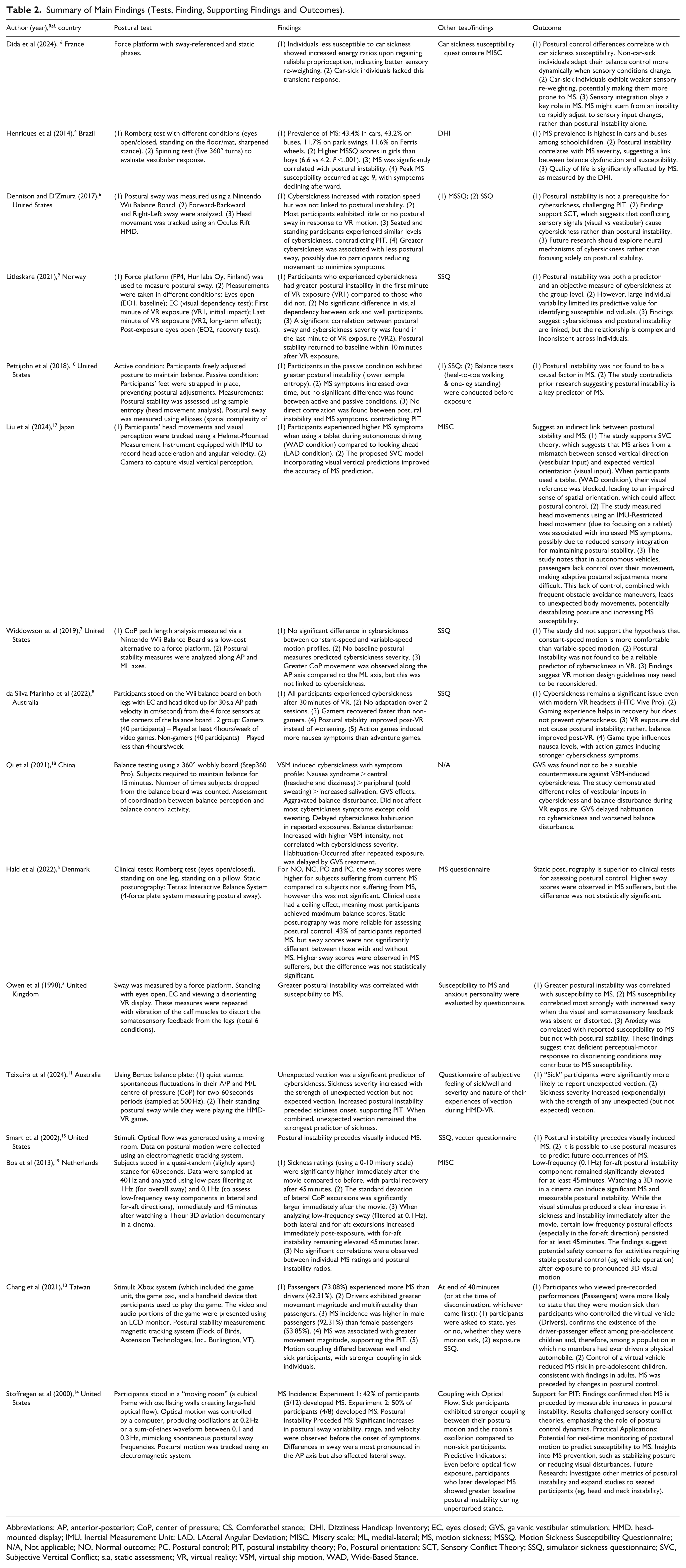
Abbreviations: AP, anterior-posterior; CoP, center of pressure; CS, Comforatbel stance; DHI, Dizziness Handicap Inventory; EC, eyes closed; GVS, galvanic vestibular stimulation; HMD, head-mounted display; IMU, Inertial Measurement Unit; LAD, LAteral Angular Deviation; MISC, Misery scale; ML, medial-lateral; MS, motion sickness; MSSQ, Motion Sickness Susceptibility Questionnaire; N/A, Not applicable; NO, Normal outcome; PC, Postural control; PIT, postural instability theory; Po, Postural orientation; SCT, Sensory Conflict Theory; SSQ, simulator sickness questionnaire; SVC, Subjective Vertical Conflict; s.a, static assessment; VR, virtual reality; VSM, virtual ship motion, WAD, Wide-Based Stance.
A total of 1518 participants were included across all studies, with age ranges spanning from 9 to 63 years. There was a general male predominance in the experimental studies. The studies investigated various forms of MS, including car sickness, simulator sickness, cybersickness, travel-related sickness, and space MS.
Types of Studies
The studies varied in design and methodology, including experimental studies (n = 12), which simulated MS through various methods, including VR, cybersickness, vehicle motion, simulations, and optical flow environments and cross-sectional studies (n = 4), which included population-level investigations or single-time-point analyses of balance and MS.
Comorbidities
Most experimental studies excluded participants with known vestibular, neurological, or visual impairments to reduce confounding. Owen et al 3 noted anxiety levels were correlated with MS susceptibility, although not with postural instability. Comorbid conditions and participant screening varied among these studies. Henriques et al 4 screened children for vestibular disorders and found MS affected quality of life, while Hald et al 5 reported that participants included individuals with migraines, concussions, and regular medication use
Postural Tests and Findings
Postural assessments included a range of clinical and experimental tools (Table 2). The most commonly used tools will be the force platforms and balance boards. The Nintendo Wii Balance Board was used as a low-cost force platform by Dennison and D’Zmura 6 and Widdowson et al 7 and da Silva et al. 8 Tetrax Interactive Balance System and Bertec balance plate were also used for measuring center of pressure displacement and sway dynamics, such as in Hald et al, 5 Litleskare, 9 Pettijohn et al 10 and Teixeira et al 11 Other instruments, such as Step360 Pro, a wobbly board used to simulate visual ship motion in investigating cybersickness by Qi et al 12 in 2020, while Chang et al 13 used an Xbox to simulate a driving game. Romberg test and static posturography were utilised in clinical settings and pediatric populations, Henriques et al 4 and Hald et al 5 Stoffregen et al 14 and Smart et al 15 used virtual perturbation environments, such as moving room paradigms, and simulated large-field optical flow to test sway adaptation. Dida et al used a force platform with sway referenced to demonstrate that non-susceptible individuals displayed effective sensory reweighting upon reintroduction of reliable proprioceptive cues. 16
A total of 14 studies revealed a relationship between postural instability and MS, in support of and challenging the PIT.3 -5,8-11,13 -18 These studies supported the PIT, which posits that postural instability precedes the onset of MS symptoms. Postural instability preceded MS onset in several studies, such as Stoffregen et al, 14 Smart et al, 15 and Teixeira et al, 11 supporting PIT. These studies demonstrated that increased postural sway or instability, especially in anterior-posterior directions, significantly predicted subsequent development of MS. These findings were consistent across VR, simulator, and traditional transport settings.
Three studies reveal contradicting results for the PIT. While Dennison and D’Zmura, 6 Petitjohn et al 10 and Widdowson et al 7 found no consistent link between postural instability and MS, favouring SCT.
Complementing Tests and Findings
Complementary assessments provided further insights, such as MS susceptibility questionnaires (MSSQ – Motion Sickness Susceptibility Questionnaires, SSQ – simulator sickness questionnaires, MISC – Misery scale), which were widely used to evaluate symptom severity and history. Visual vertical perception used by Liu et al 17 using head-mounted display (HMD) to compare perceived against actual vertical orientation, aligning with the Subjective Vertical Conflict (SVC) model. Qi et al 12 used Galvanic vestibular stimulation (GVS), revealing that GVS exacerbated balance disturbances but had minimal effect on nausea. Postural control coupling by Chang et al found that drivers experienced less MS and showed stronger movement control than passive passengers. 13 Teixeira et al showed that unexpected vection was a stronger predictor of cybersickness than instability, indicating that perceptual mismatch may result in MS symptoms. 11
Supporting Outcomes
Through this review, we have also noted other supporting outcomes from the studies. Notably, cybersickness is common in VR-based studies, such as those by da Silva Marinho et al 8 noted postural stability improved after VR exposure in gamers while Teixeira et al 11 highlighted unexpected vection as a primary driver of symptoms. In a study by Henriques et al, high rates of MS were reported in children travelling in cars and buses. 4 Liu et al showed that restricted head movement during tablet use increased symptoms of MS. 17 Bos et al found persistent low-frequency postural instability after watching a 3D film, which resulted in visual MS. 19 Some studies, such as in da Silva Marinho et al, 8 revealed that gamers recovered more rapidly from VR-induced MS, likely due to prior sensory adaptation. In supporting the multifactorial cause of MS, Dida et al highlighted that better reweighting of proprioceptive and vestibular inputs correlated with reduced MS susceptibility. 16
Overall, the findings highlight a complex interplay between sensory processing, postural control, and perceptual mismatch in the development of MS across various environments and populations.
Discussion
Postural Instability as a Predictor of MS
The PIT proposes that MS arises due to an inability to maintain stable posture in unfamiliar motion environments.11,14,15 Several studies in this review support PIT by demonstrating increased postural sway and delayed postural adaptation in individuals susceptible to MS.
This theory was introduced in the early 1990s and described by Riccio and Stoffregen in a review article as a theory bridging the gap between perception, action, and environmental dynamics by emphasising the role of stability in maintaining effective behaviour. This theory explains that when individuals are unable to maintain stability in response to environmental or self-generated perturbations, MS symptoms arise. PIT is further discussed regarding the source of MS, which is described as a challenge to postural stability. This includes low-frequency vibration in the 0.1 to 1.0 Hz range (eg, on ships or vehicles), which disrupts feedback necessary for stable posture. The body’s natural postural control operates within this frequency range, leading to destabilisation. Other causes are also described, such as weightlessness in microgravity, coriolis forces, such as when the head is rotated during motion, changing gravitoinertial force relationships, causing rapidly changing direction of force, such as in roller coasters, and visual-vestibular mismatches where visual motion is not aligned with physical motion (eg, in simulators or moving rooms). 1
Following the introduction of the new theory of MS, multiple studies have been conducted to analyse the PIT. One of the earlier studies, by Stoffregen et al in 1998 and 2000, showed significant increases in postural sway variability, range, and velocity before the onset of MS symptoms. 2 These findings confirmed that measurable increases in postural instability precede MS.
Vehicular MS and PIT
A total of 6 studies describe the relationship between vehicular MS and PIT.
Henriques et al in 2014 assessed 831 children and found that MS prevalence peaked at age 9, aligning with periods of postural instability during development. This study, which utilises clinical tests (the Romberg test in various conditions and the Spinning test) to assess postural stability, reveals that postural instability is correlated with the severity of MS, and quality of life is also significantly impacted by MS. 4
While Dida et al in 2024 analysed 64 adults and found that individuals who exhibit car sickness have weaker sensory re-weighting, potentially making them more susceptible to MS. This reinforces the idea that failure to adapt to postural control increases the risk of MS. 16
Liu et al conducted a study in Japan on autonomous vehicles, where it was found that when passengers lack control over their movement, making adaptive postural adjustments is more difficult. This lack of control, combined with frequent obstacle avoidance manoeuvres, leads to unexpected body movements, potentially destabilising posture and increasing susceptibility to MS. This study also explores and supports the SVC theory, which suggests that MS arises from a mismatch between the sensed vestibular input and the expected visual input for vertical orientation. 17
While studies such as Smart et al 15 and Owen et al 3 support PIT as a contributor to MS susceptibility, Hald et al 5 in 2022 conducted a study among students with a mean age of 13.7, using clinical tests and static posturography, found no significant correlation between MS and postural control.
Cybersickness and Simulator-Induced MS and PIT
In VR studies, though findings suggest individual variability in postural adaptation, PIT remains relevant. Litleskare in 2021 examined 50 participants in a VR setting and found that there was a significant correlation between the severity of cybersickness and the change of postural stability from the first to the last minute of VR exposure for trace length (rs = 0.32, P = .027), but not standard deviation velocity (rs = 0.20, P = .187). The deteriorations had returned to baseline levels 10 minutes after exposure. These findings suggest that deterioration of postural stability was both a predictor and an objective measure. However, due to significant individual variations and the limited strength of correlations, deterioration of postural stability has limited practical value as both a predictor and objective measure, suggesting a complicated association. 9
Teixeira et al provided more substantial support for PIT. Participants who developed sickness during HMD-VR exposure exhibited increased postural instability prior to symptom onset. However, the study emphasised the role of unexpected vection, where a mismatch between expected and perceived self-motion is a more robust predictor of sickness. 11
In contrast, Qi et al examined cybersickness induced by virtual ship motion, with and without GVS. While GVS aggravated postural imbalance and delayed habituation, it did not significantly worsen cybersickness symptoms. This decoupling between balance disturbance and symptom severity further undermines a direct causal role for postural instability, offering limited support for PIT and supporting the idea that postural control still relies on peripheral vestibular input during VR immersion. 12
Bos et al in 2013 measured postural sway before and after exposure to a 3D aviation documentary in a cinema simulator setting. The study shows a significant increase in low-frequency sway, especially in the fore-aft direction, up to 45 minutes. The persistence of low-frequency sway suggests a lingering vestibular or sensorimotor disruption; however, no correlation was found between sway magnitude and individual sickness ratings. This suggests that postural instability alone may not be a sufficient predictor for MS. 19
Additional insights from Dennison and D’Zmura et al reinforce this complexity. Using a rotating tunnel simulation in 15 adult participants, the study found that cybersickness occurred despite minimal postural sway. In fact, in contradiction to PIT, those who experienced more severe symptoms often demonstrated less movement, suggesting an adaptive reduction in sway to mitigate discomfort. 6
Likewise, da Silva Marinho et al found that simulator-induced sickness occurred across all VR participants irrespective of gaming experience after prolonged exposure, but postural stability actually improved post-VR exposure for 30 minutes. This improvement, along with the absence of predictive sway data, challenged PIT’s assumption that instability precedes and predicts simulator-induced sickness. 8 Simulator studies, such as a study by Pettijohn et al, exposed participants to simulated boat motion (active patients where subjects could actively adapt their posture, while passive patients had their feet affixed) and observed that MS symptoms increased over time despite varying levels of postural control. However, there was no difference between the active and passive groups. In addition, there were no differences in symptoms and postural instability in both groups, contradicting PIT. 10
In investigating cybersickness, Widdowson et al used 2 VR simulation experiments involving linear and circular motion. Although differences in postural movement patterns were observed, these did not correlate with cybersickness symptoms. 20 Baseline postural stability failed to predict which participants would become sick. 7 In contrast, Chang et al, in a study of preadolescent subjects, provide support for the PIT. In a virtual driving simulation, passengers (who lacked control over the vehicle) experienced a significantly higher incidence of MS compared to drivers. These results support the idea that reduced postural flexibility and control might increase susceptibility to simulator-induced sickness. 13
In this review, we acknowledge the heterogeneity of MS presentations (eg, car sickness, simulator sickness, cybersickness, seasickness, visually induced MS) and measurement tool and that these variations in symptom presentation, environments, and measurement tools across studies may limit direct comparability of findings and contribute to inconsistent conclusions regarding the role of postural instability.
The review highlights consistent signals that postural instability often precedes MS in several paradigms but also shows many null findings; this mixed pattern implies multiple interacting mechanisms (PIT and SCT), not a single universal cause. We recommend the adoption of standardized diagnostic criteria and standardized postural metrics in future studies.
We propose research priorities: (1) prospective pediatric cohort studies using standardized criteria, (2) randomized controlled trials testing balance-training interventions for MS rehabilitation, (3) multimodal studies integrating vestibular, visual-vertical, and postural measures; to get more comprehensive information and work toward intervention, prevention, and rehabilitation of MS.
Conclusion
Although postural instability precedes MS, the quality of evidence is inadequate to determine the cause-and-effect relationship between MS and postural instability until extensive, multicentre, randomised controlled studies are conducted.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Available upon request.