
Abstract
Level of evidence: 5 – expert opinion
Introduction
In the early 1800s, several physicians noted an association between a small jaw (micrognathia) and cleft palate in infants with feeding problems. Almost 100 years passed, however, before the French stomatologist, Pierre Robin provided an anatomic basis and identified the important airway implications of micrognathia and glossoptosis – the sequence that today bears his name. In the early 20th century, mortality among infants with Robin sequence was high, both from airway compromise and failure to thrive. 1 To combat these problems, Robin spent much of his career developing therapeutic solutions that allowed these children to breathe and grow. His work laid the foundation for the modern multidisciplinary approach to treatment.
Beginning in 1923, Robin described glossoptosis as a novel cause of airway obstruction, publishing the first of 17 articles on the subject. He identified the posterior displacement of the tongue (i.e., glossoptosis) as a consequence of mandibular hypoplasia. 2 To correct this “dysmorphic atresia of the mandible,” he proposed a device that helped move the lower jaw forward, resulting in “liberation of the oral pharynx.” 2 Aiming to realign the mandible, this custom-made mandibular advancement device was designed to engage both the maxilla and mandible, repositioning the jaw forward to relieve pharyngeal obstruction. Robin emphasized tailoring the device to each patient’s age and facial structure to achieve maximal relief of upper airway obstruction, anticipating the individualized approach central to modern craniofacial care. Robin’s device foreshadowed mandibular advancement devices now used for obstructive sleep apnea and the skeletal lengthening techniques of distraction osteogenesis. 3 Robin’s recognition that altering mandibular position could transform airway patency was an important conceptual leap forward.
However, not all children could tolerate prosthetic devices, which required careful adjustments and frequent follow-up. In addition, socioeconomic barriers and limited access further constrained widespread adoption of these devices, especially outside major European centers. Thus, throughout the first half of the 20th century, clinicians also experimented with conservative airway strategies. Prone positioning became widespread, as gravity could pull the tongue base forward and improve airflow by relieving glossoptosis. 4 Simple interventions such as nasopharyngeal airways were also adopted to provide a temporary bypass. 1 These approaches reflected Robin’s original warning that airway obstruction posed the greatest threat to infants with Pierre Robin syndrome (Figure 1). 2 Yet conservative methods often proved inadequate in severe cases, where recurrent hypoxia, aspiration, and failure to thrive necessitated more definitive solutions. 5
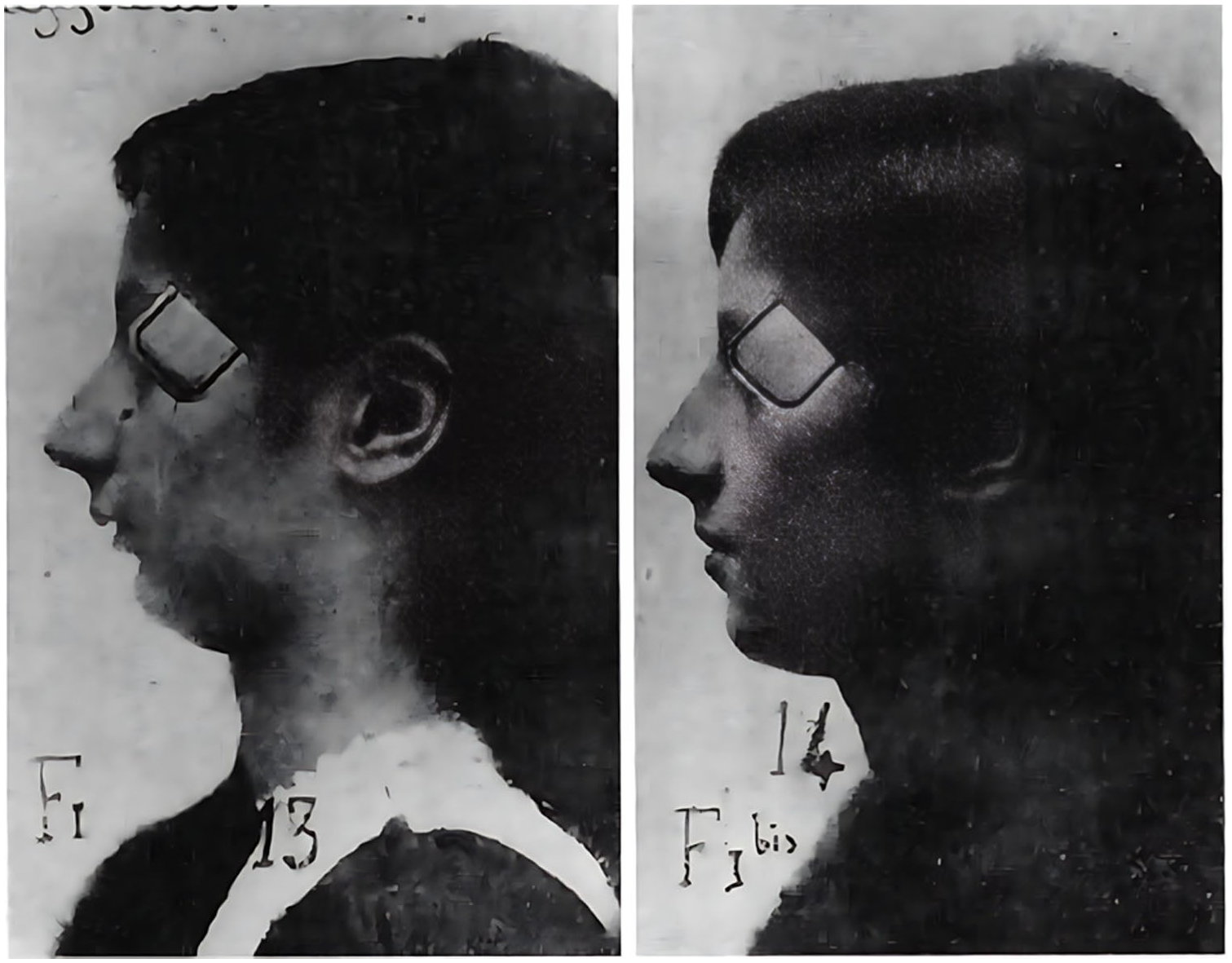
Pierre Robin syndrome treated with mandibular advancement device. 2
By the mid-20th century, surgical interventions gained more traction. Tracheostomy emerged as the most definitive airway procedure. While effective, it carried substantial neonatal morbidity and mortality and had the potential for profound long-term consequences on speech and development. 3 Seeking less invasive alternatives, tongue-lip adhesion, a technique anchoring the tongue anteriorly to prevent posterior collapse, was introduced. Early reports demonstrated that it could reduce reliance on tracheostomy but required careful patient selection given its risks of dehiscence, severe dysphagia, and lip scarring. 6 Though imperfect, tongue-lip adhesion built on Robin’s original principle of manipulating the airway to improve long-term survival.
By the late 20th century, neonatal intensive care, specialized craniofacial teams, and surgical advancements transformed management. The most notable innovation was mandibular distraction osteogenesis, whereby the tongue base is moved anteriorly by its attachments to the distracted mandible. 3 Through a more stable and substantial repositioning of the tongue base, mandibular distraction may allow earlier extubation, more successful oral feeding, and more effective short- and long-term reduction in obstructive sleep apnea. 7 Recently, orthodontic airway plates – composed of intraoral, intrapharyngeal, and extraoral components – have emerged as a non-surgical alternative to help normalize breathing. 8 Yet many modern strategies echo early interventions: positioning remains first-line for mild obstruction, prosthetic and surgical airway adjuncts are still used selectively, with tracheostomy reserved as a last resort for refractory cases. 5
Pierre Robin’s legacy in treatment of Robin sequence extends far beyond nomenclature. Robin was both a diagnostician and an innovator. The evolution of safer, more effective therapies over the last century reflects Robin’s goal of balancing a secure airway with the continuing needs childhood of maxillofacial development (Figures 2 and 3).

A child with Robin sequence and U-shaped cleft palate. A nasogastric feeding is in place for nutrition.

Robin’s 1902 device consisted of a plate with an expansion screw. The appliance stimulated facial muscular activity by changing the position of the jaws (by permission, British Orthodontic Society, https://bos.org.uk/museum-and-archive/appliances-and-equipment/functional-appliances/monobloc/, accessed November 20, 2025). 9
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.