
Abstract

Significance Statement
Esophageal duplication cysts (EDCs) are rare congenital lesions that can mimic other cystic neck masses, posing diagnostic and therapeutic challenges. This case emphasizes the importance of correlating imaging and histopathologic findings to achieve an accurate diagnosis. Recognizing atypical submental presentations broadens clinicians’ awareness of foregut duplication cysts and supports timely surgical management to prevent potential complications.
Text Proper
A 29 year-old woman presented with a 6 month history of an asymptomatic submental swelling, without dysphagia, dysphonia, fever, or signs of infection. After obtaining written informed consent, a clinical examination was performed. Extraoral evaluation revealed a firm, mobile, and nontender mass. Fine-needle aspiration yielded ~60 mL of hemorrhagic, serous fluid. Computed tomography (CT) demonstrated a well-circumscribed cystic lesion with a thick capsule and central hyperdensity, measuring 6.69 × 5.83 cm, in close relationship to the airway region (Figure 1A–C). The lesion decreased in size following aspiration. Differential diagnoses included dermoid or epidermoid cyst, thyroglossal duct cyst, ranula, and lymphoepithelial cyst.
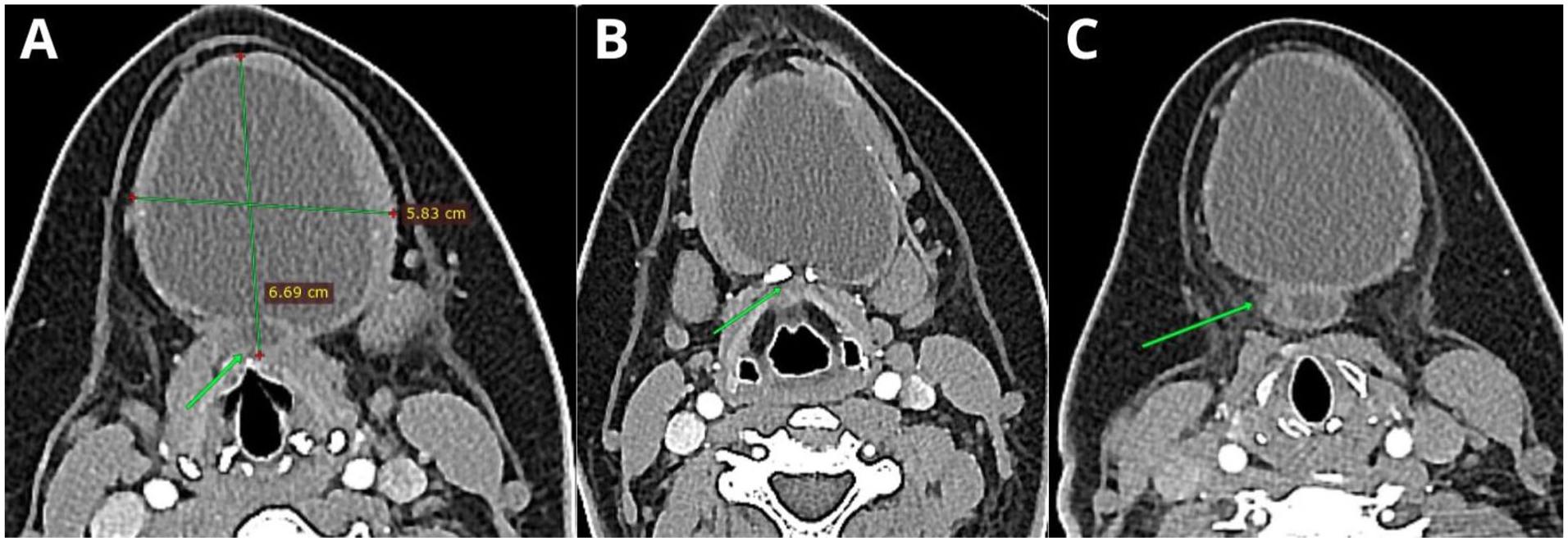
Axial computed tomography images showing a cystic mass involving the upper third of the neck, closely related to the anterior portion of the airway (A, green arrow). The middle part of the lesion exhibits a fenestration through the lower third of the hyoid bone, with a slight capsular projection (B, green arrow). The inferior portion of the lesion demonstrates a tubular cystic extension directed posteriorly (C, green arrow).
Surgical excision was performed via a submental approach (Figure 2). Histopathologic examination revealed a cystic cavity lined predominantly by pseudostratified columnar epithelium with superficial microvilli and goblet cells, with focal transition to a stratified epithelium composed of 1 to 3 cell layers. The connective tissue showed a loose, irregular stroma, a subepithelial eosinophilic hyaline band, discrete perivascular mononuclear lymphocytic infiltrates, and a thin smooth muscle layer interspersed with vasculoneural bundles. Peripheral areas contained striated skeletal muscle fibers and adipose tissue associated with irregular esophageal-type connective tissue. These findings were diagnostic of an EDC (Figure 3A–C). The postoperative course was uneventful, and the patient remains asymptomatic. This case highlights the diagnostic challenges of EDCs and underscores the pivotal role of histopathologic analysis.
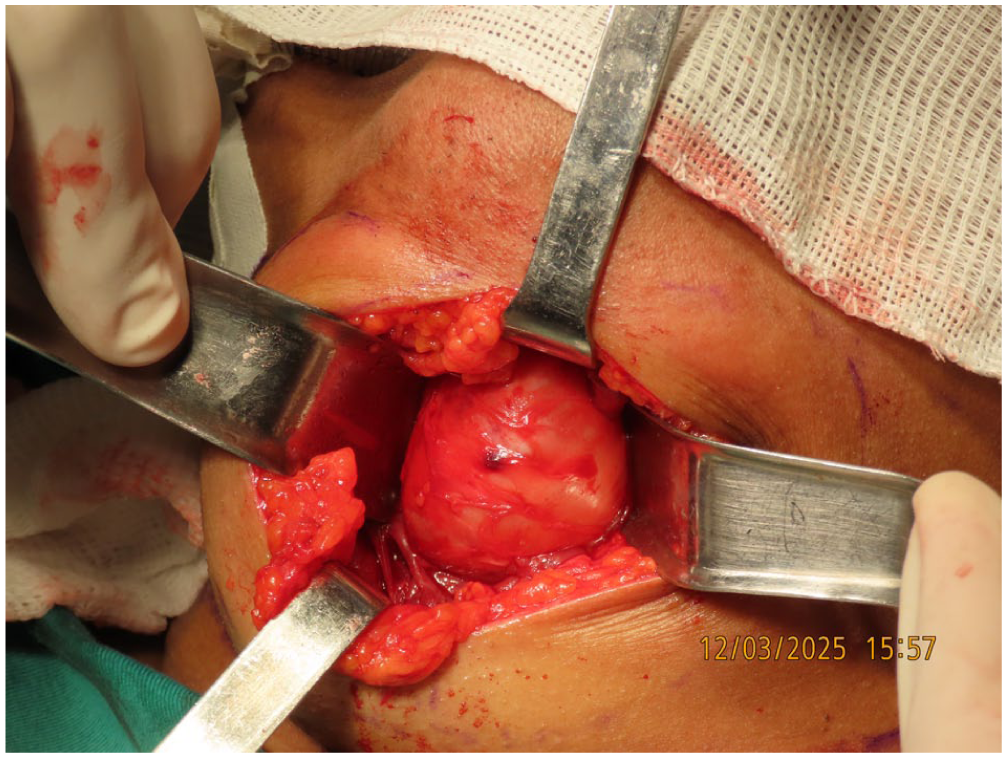
Submental surgical access showing the macroscopic appearance of the cystic lesion.
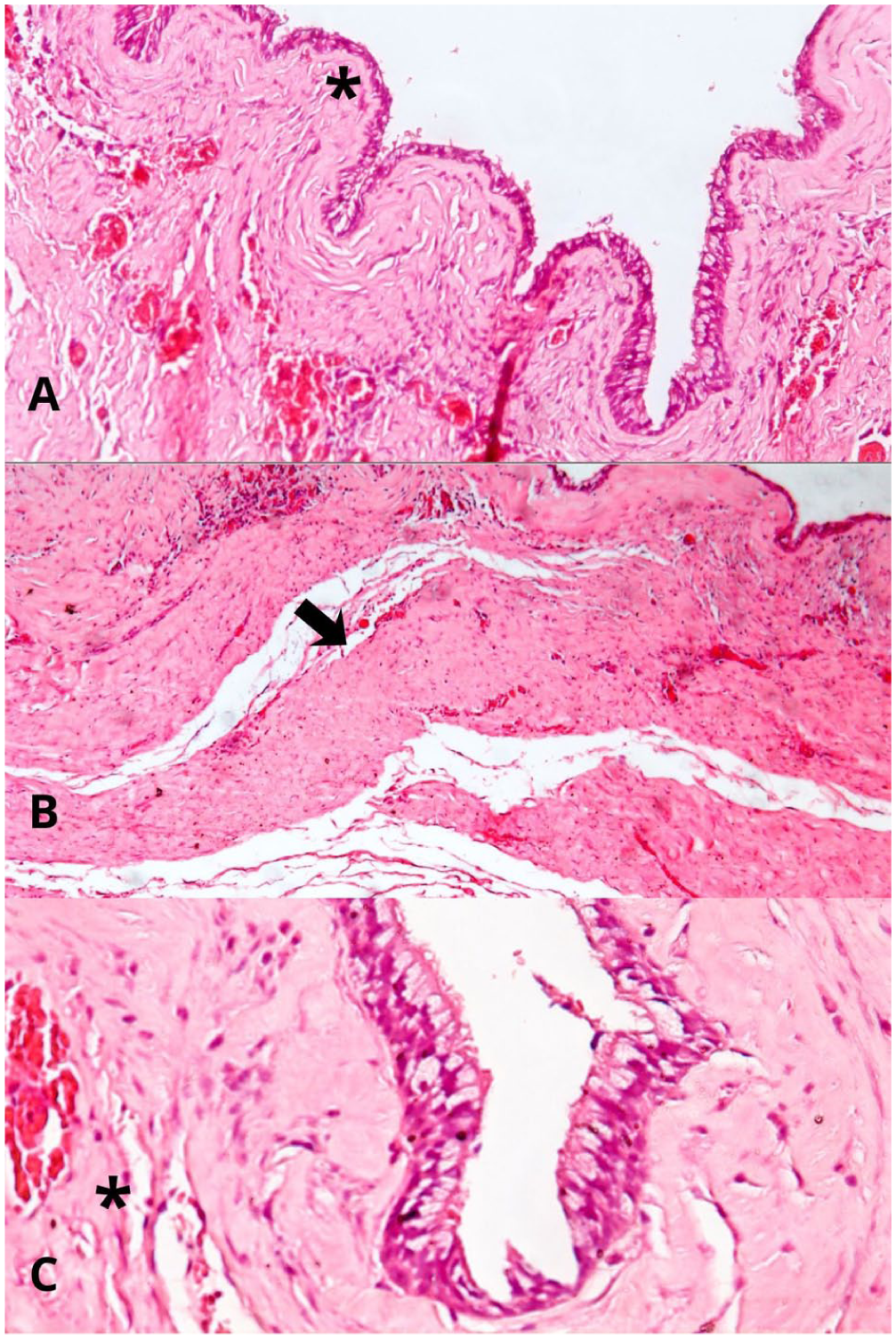
Histopathologic examination showing a cystic cavity lined by pseudostratified columnar epithelium with superficial microvilli and scattered goblet cells, gradually transitioning to a stratified epithelium composed of 1 to 3 cell layers (A, hematoxylin and eosin stain, ×100, asterisk). The underlying connective tissue is loose and irregular, exhibiting a subepithelial eosinophilic hyaline band and focal, mild perivascular lymphohistiocytic infiltrates (arrow). A thin smooth muscle layer containing interspersed vasculoneural bundles is also identified. At the periphery, bundles of striated skeletal muscle fibers and adipose tissue are present, associated with the loose, irregular connective tissue of the esophageal serosa (asterisk; B, C, hematoxylin and eosin stain, ×100).
Foregut duplication cysts are classified into bronchogenic cysts, EDCs, and enteric duplication cysts, according to their epithelial type and associated histological features. For diagnosis, at least 3 criteria must be met: (1) the lesion is surrounded by a smooth muscle layer; (2) it contains foregut-derived epithelium; and (3) it is attached to a portion of the foregut. These cysts are typically asymptomatic and slow-growing; however, larger lesions may present with odynophagia, feeding difficulties, sore throat, dysphagia, or dyspnea.1,2
On magnetic resonance imaging, they generally exhibit hyperintensity on T2-weighted sequences and variable signal intensity on T1-weighted sequences. CT usually reveals well-defined, well-circumscribed lesions with a thick capsule. In larger cysts, a posteriorly directed tubular extension may also be observed. In the head and neck, these cysts most frequently occur in the anterior oral cavity, particularly the floor of the mouth and the tongue.3,4
Complete surgical excision remains the treatment of choice, with favorable outcomes and minimal risk of complications. Recurrence is rare after excision, although malignant transformation has been reported in long-standing lesions managed conservatively through observation or aspiration. Definitive diagnosis requires histopathologic and, when indicated, immunohistochemical examination. Histologically, foregut cysts may be lined by respiratory, gastrointestinal, or pancreatic-type epithelium, and may include areas of stratified squamous epithelium. When performed, immunohistochemical staining may demonstrate positivity for CK20, CK7, and TTF-1.3,5
This case highlights the diagnostic complexity of submental lesions, which may present with overlapping clinical and radiographic features. Comprehensive imaging, along with histopathologic and, when indicated, immunohistochemical analysis, is essential for establishing an accurate diagnosis and guiding appropriate surgical management.
Footnotes
Consent to Participate
Written informed consent was obtained from the patient.
Author Contributions
Eliandro de Souza Freitas: data acquisition (articles and literature review); senior resident responsible for the case; manuscript conception, writing, and design; data analysis and interpretation; drafting and critical revision of the manuscript; final approval of the version to be published. Tiago Novaes Pinheiro: oral and maxillofacial pathologist responsible for the case; contributed to data analysis and interpretation. Tharcísio Veríssimo Dantas Nóbrega: assistant resident. André Luís Costa Santos de Jesus: assistant resident. Patrick Vilela Paquer: chief surgeon of the case.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.