
Abstract

Significance Statement
Lymphoepithelial cysts (LECs) are rare cystic lesions of the salivary glands. While the parotid gland is the most frequently affected, submandibular region involvement is much less common. They are mostly associated with HIV infection. Even if the localization is rare, clinicians should include LEC in their differential diagnosis for cystic lesions affecting the submandibular region. This case is of particular interest due to its unusual location and the rarity of LECs in HIV-negative individuals. It underscores an important differential diagnosis to consider in cases of submandibular swelling.
Case Presentation
A 58-year-old man, without a medical history, presented with a painless left submandibular swelling that had been evolving over a period of 2 years.
On physical examination, the mass was soft, mobile, and measured 3.5 cm (Figure 1). Contralateral submandibular region and parotid glands examinations were normal. Neck ultrasound revealed a 38 mm cystic lesion within the left submandibular region. Based on the clinical and ultrasound findings, the main suggested diagnoses were salivary duct retention cyst, metastatic lymph node, and branchial cleft cyst. Fine needle aspiration yielded fluid content with no nucleated cells. HIV serology and Sjögren’s disease screening tests were negative.

A left submandibular soft mass (yellow arrow).
The patient underwent an excision of the cyst, which was found to be extraglandular (Figure 2). The adjacent submandibular gland was macroscopically normal. No postoperative complications were noted.
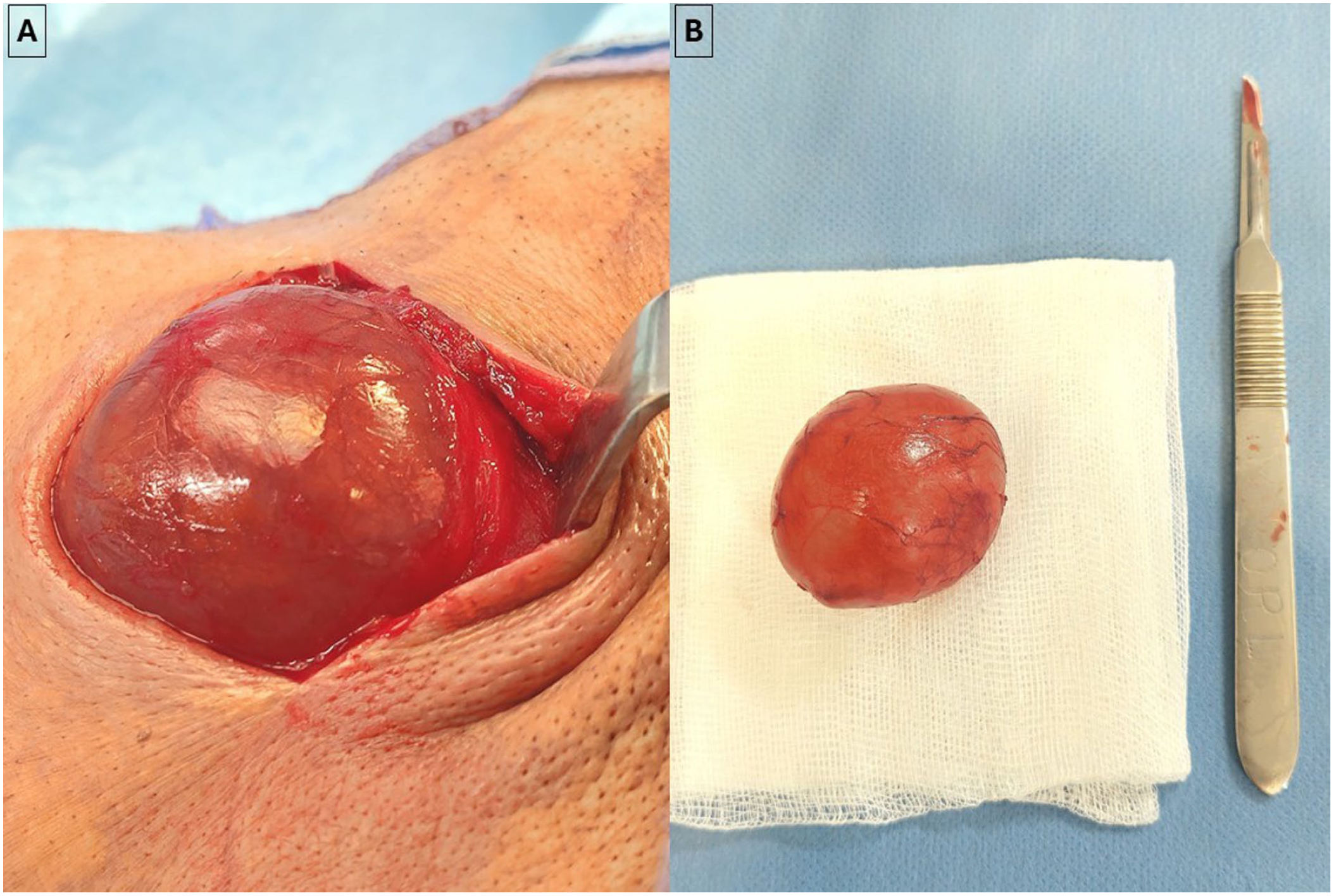
(A) Intraoperative view of the cystic lesion which was extraglandular. (B) Macroscopic image of the cyst after complete resection.
Histopathological examination confirmed the diagnosis of a benign lymphoepithelial cyst (LEC; Figure 3). No recurrence or malignant transformation has been noted after 10 months of follow-up.
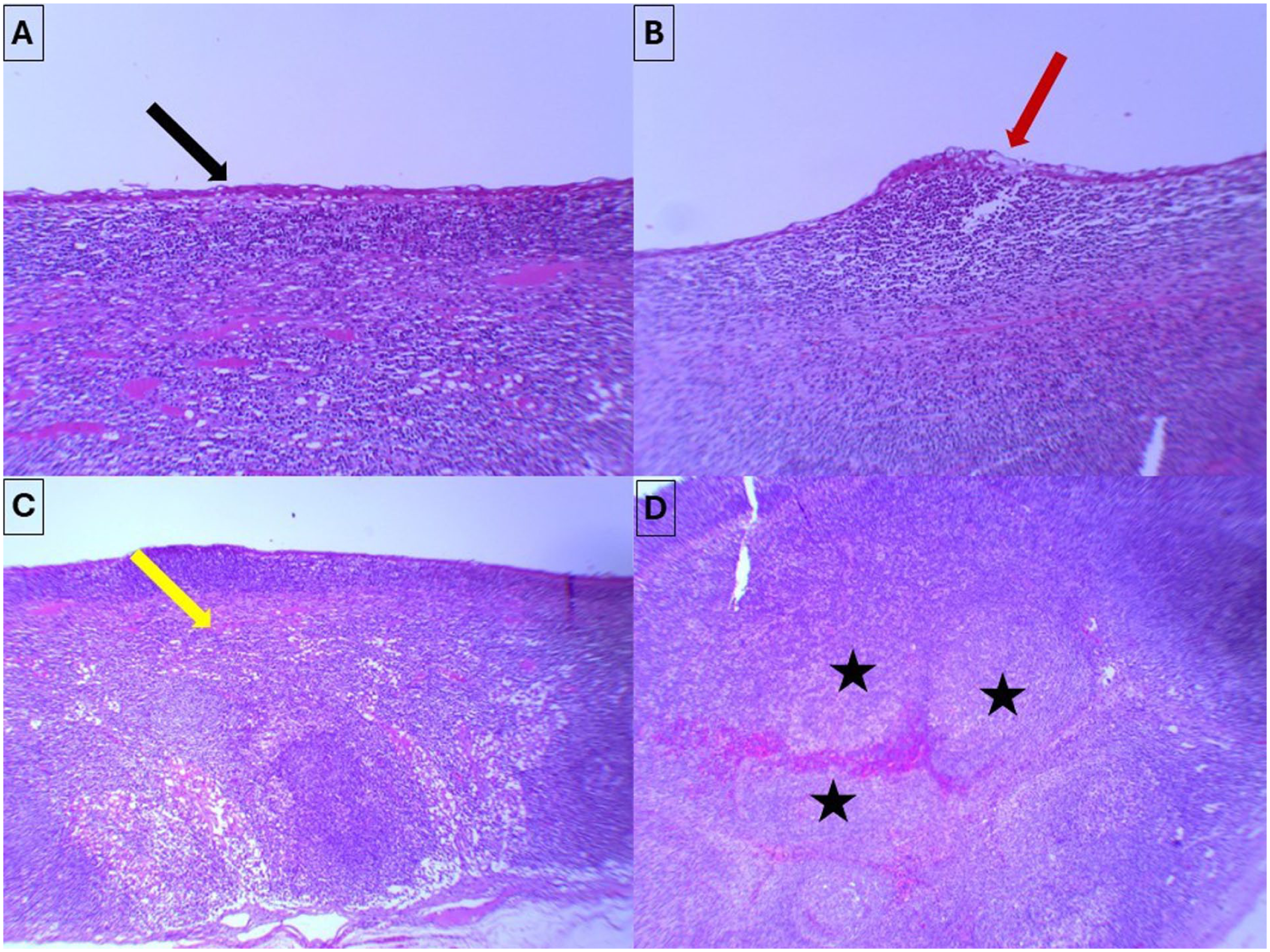
(A and B) The cyst wall is lined by a flattened squamous-type epithelium (black arrow), with focal areas showing respiratory-type epithelium (red arrow) (hematoxylin-eosin × 20). (C) The epithelial lining overlies fibrous connective tissue exhibiting a dense inflammatory infiltrate composed predominantly of lymphocytes (yellow arrow) (hematoxylin-eosin × 4). (D) The lymphocytic infiltrate organizes into lymphoid follicles, with occasional enlarged and pale germinal centers (black stars) (hematoxylin-eosin × 10).
Discussion
LECs are uncommon, slowly growing cystic lesions of the salivary glands.1,2 Although parotid involvement is most common, isolated submandibular cases are exceptional.2,3
The main hypotheses suggested are cystic transformation of salivary gland inclusions entrapped in the lymph node within or around (as in our patient) the gland during embryogenesis, or migration of HIV-infected cells into the salivary gland inducing metaplastic and cystic changes in the salivary ducts.1,4
The LEC can be single or multiple. 4 Histologically, the cysts are observed in a lymph node, adjacent to or embedded in the submandibular gland. 4 The cyst is histologically lined with a stratified squamous epithelium, respiratory epithelium, or both, overlying a lymphoid connective tissue. 3
Cystic lesions of the submandibular region are very uncommon. However, submandibular cystic masses pose a diagnostic challenge, as many different pathologies can manifest with similar cystic features. The potential clinical differential diagnoses are salivary duct retention cyst, cystic metastatic lymph node, branchial cleft cyst, chronic sclerosing sialadenitis, Warthin tumor, mucoepidermoid carcinoma, lymphoma, and lymphangioma.1,3 Patients over 50 years of age should raise consideration for a possible malignant etiology, particularly a cystic metastatic lymph node from a head and neck squamous cell carcinoma, since malignant tumors of the submandibular gland are relatively uncommon. In HIV-positive patients, lymphoma and LEC should be the primary considerations. In HIV-negative patients, clinicians should first consider a salivary duct retention cyst, a cystic metastatic lymph node, and a branchial cleft cyst.
Due to the well-established relationship between LEC and HIV, and the higher frequency of LEC in HIV-positive patients, serologic testing for HIV should be systematically included in the diagnostic workup of any patient presenting with such lesions.3 -5 LECs can be associated with other conditions like Sjogren’s syndrome, Mikulicz’s disease, and myoepithelial sialadenitis. 2 In our patient, the screening for HIV and Sjogren’s syndrome was negative.
Therapeutic options included surgery, fine‑needle aspiration, radiotherapy, sclerotherapy, and conservative therapy with highly active antiretroviral therapy (HAART) medications.2,4 In HIV-positive patients, management may involve observation under HAART or repeated fine-needle aspirations to relieve symptoms. In HIV-negative individuals, surgical excision remains the treatment of choice. 3
Malignant transformation is rare, but exists.3,4 Therefore, a close follow-up is indicated.3,4 Recurrence is rare if complete surgical excision is obtained. 1
Footnotes
Consent for Publication
Written informed consent was obtained from the patient to publish the imaging clinic article.
Author Contributions
Wadii Thabet: Conceptualization & Writing. Marwane Mfathia: Data collection & Writing. All authors reviewed the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this research are included in this published article. Data supporting the findings of this study are available from the corresponding author on reasonable request.