
Abstract

Significance Statement
Granulomatosis with polyangiitis (GPA) can present various otolaryngologic (ENT) manifestations, such as sinusitis and otitis media, and may be complicated or uncomplicated. 1 Recognition of disease pattern is critical as mortality approaches 80% in untreated patients. 2 This report describes a challenging presentation of the condition with simultaneous, progressive bilateral parotitis, acute sinusitis, and complicated otitis externa/media ultimately leading to facial paresis.
Manuscript
A 38 year-old South Asian male was referred to the ENT clinic for persistent otalgia and otorrhea despite oral ciprofloxacin treatment for otitis externa. Medical history was significant for a positive QuantiFERON test earlier in the month with recent history of international travel. On initial evaluation, he was treated with oral amoxicillin-clavulanate for concern of left parotitis, fluconazole for concern of left fungal otitis externa, and methylprednisolone. Additional work-up included a negative culture of the left external auditory canal (EAC) and neck ultrasound showing signs of bilateral parotitis (obtained 6 days after the clinic visit). He returned to clinic 12 days later with persistent symptoms and was sent to the emergency department. Computed tomography neck revealed bilateral parotitis with a 2.2 cm right parotid abscess, left middle ear opacification, and left maxillary sinus opacification (Figure 1). He was admitted and underwent needle aspiration of the parotid abscess. Intravenous antibiotics were empirically started. Cultures of the left EAC and right parotid abscess aspirate detected no typical or acid-fast microorganisms. PCR for Methicillin-resistant Staph aureus (MRSA) and HIV serology were negative, and chest radiograph revealed no pulmonary processes. Labs demonstrated leukocytosis, anemia, and elevated C-reactive protein (CRP). Antinuclear antibody, anti-Ro, and anti-La were negative; however, c-ANCA titers were weakly positive (1:40). After 2 days, he was switched to piperacillin-tazobactam and vancomycin with clinical improvement. Leukocytosis normalized and he was transitioned to oral antibiotics for discharge.

Coronal cut of CT neck upon initial presentation to the emergency department, showing bilateral parotitis with 2.2 cm right parotid abscess. CT, computed tomography.
Three days later, he returned with left facial weakness (House-Brackman grade IV) and spontaneous purulent drainage at the left pre-tragal region. At this time, extrapulmonary tuberculosis or GPA was suspected. He underwent left myringotomy with tube placement, left maxillary antrostomy, and incisional biopsy of left parotid gland to obtain additional tissue. Pathology results of the maxillary sinus revealed dense acute and chronic inflammation throughout the specimen with some normal glands as well as focal necrosis (Figure 2). Superficial parotid gland biopsy showed extensive, dense, acute, and chronic inflammation completely obscuring the normal architecture of the gland, as well as focal necrosis (Figure 3). Further antibody testing revealed significantly elevated PR3-ANCA levels, leading to a diagnosis of GPA in the setting of latent tuberculosis infection. GPA treatment was initiated with prednisone and methotrexate while the infectious disease team continued to follow-up for tuberculosis management. At 4 months following diagnosis, facial weakness has only partial recovered.
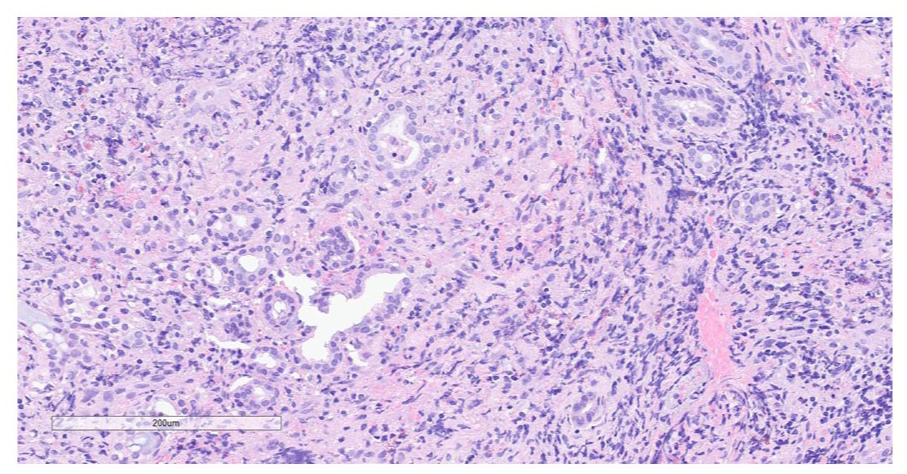
Pathology results of the maxillary sinus revealing dense acute and chronic inflammation throughout the specimen with some normal glands as well as focal necrosis.
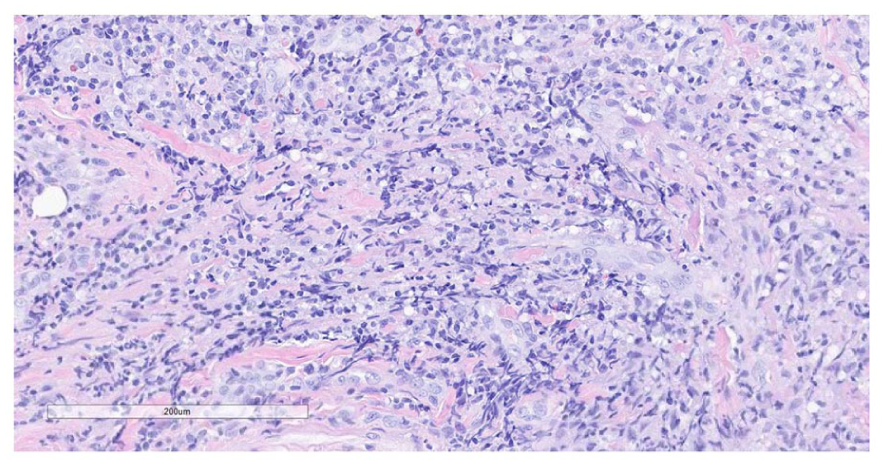
Superficial parotid gland biopsy showing extensive, dense, acute, and chronic inflammation completely obscuring the normal architecture of the gland, as well as focal necrosis.
ENT involvement is observed in 71.9% (64/89) of GPA cases. Sinonasal and otologic manifestations are the most common symptoms, seen in 58.4% and 34.8% of all cases, respectively. Patients experiencing head and neck symptoms present younger with less likelihood of renal involvement, however with better outcomes. 3 A study of chronic GPA patients with predominantly ENT manifestations found that only 14% (3/22) were symptomatic with otitis externa. 4 While external ear involvement has been described, it is exceedingly rare as an initial presentation of GPA. Similarly, salivary gland involvement has been reported in ANCA-associated vasculitis. 5 The parotid gland is the most commonly affected, but there are few published reports of parotitis as a presenting feature of GPA.6,7 To our knowledge, unilateral otitis externa and parotitis has been reported once previously as the initial manifestation of GPA. 8 Our patient appears to be the first presenting with bilateral parotitis and otitis externa.
Interestingly, clinical features of ANCA-associated vasculitis vary depending on geographical region, with hypotheses that HLA genes contribute to prognosis. 9 Epidemiological studies have demonstrated that incidence of GPA is decreased in south Asian populations, and renal symptoms are less likely. 10
This case was further complicated as extrapulmonary tuberculosis has been described with sinusitis, otitis, parotitis, and facial palsy.11,12 Tuberculosis can also induce production of ANCAs. 13 Due to these factors, limited GPA is a challenging diagnosis, that is, most commonly mistaken for tuberculosis. Confusion is more likely in the setting of latent tuberculosis infection. 14
The pathogenesis of GPA and factors contributing to a subacute disease process remain to be fully understood. Multisystem presentations involving the upper respiratory tract, lungs, and kidneys should classically raise suspicion for the pathology. ENT providers should recall that a limited disease course with exclusively ENT involvement has been described, as well. GPA is an important diagnostic consideration in patients with head and neck inflammation refractory to conventional treatments.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Written informed consent to present and publish this case report was obtained from the patient.
Author Contributions
M.M. conducted literature review and drafted/critically revised the manuscript. T.P. drafted and critically revised the manuscript. M.S. provided pathological assessment and assisted in drafting the manuscript. K.P. and H.N. critically revised the manuscript and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data pertaining to this report are available upon request, so long as it is within HIPAA guidelines.