
Abstract
Background:
Rhinoplasty is a widely performed cosmetic and functional procedure. Despite its popularity, postoperative dissatisfaction remains a common concern. This study aims to assess patient satisfaction and quality of life using the rhinoplasty outcome evaluation (ROE) survey, to help improve preoperative planning and postoperative care.
Patients and Methods:
A systematic literature review was conducted in PubMed, Cochrane, Google Scholar, EBSCO, and Web of Science using the terms “Rhinoplasty OR Septorhinoplasty,” “Satisfaction OR Prognosis OR Outcome,” “Quality of Life OR QoL,” and “ROE OR Rhinoplasty Outcome Evaluation.” All studies published between 2018 and 2024 were selected, and nonrelevant studies were excluded after full text review.
Results:
Twenty-four studies were included in a meta-analysis comparing ROE scores pre- and postoperative. The results demonstrated a significant improvement in satisfaction and quality of life postoperatively. The subgroup analysis revealed a notable variation in the outcome according to the country of origin. Although the study heterogeneity was high (I2 = 99.8%), a random-effects model was used for the analysis.
Conclusions:
Gender was not a major determinant of satisfaction. However, the country of origin significantly influenced ROE scores. These findings emphasize the need for culturally sensitive counseling, individualized surgical planning, and management of patient expectations to enhance satisfaction.
Introduction
Rhinoplasty is a commonly performed surgical procedure in the field of otorhinolaryngology and plastic surgery, 1 it aims to improve both functional and aesthetic aspects of the nose. As an essential facial structure, the nose plays a critical role in facial symmetry, identity, and aesthetic conformity. 2 Beyond physical modifications, rhinoplasty significantly affects psychological well-being. The dual goals of achieving nasal functionality and patient satisfaction make this procedure particularly challenging. 3
The results of rhinoplasty have a profound impact on patients, encompassing improvements in self-esteem, social interactions, and overall quality of life. However, the evaluation of the success of the procedure goes beyond objective measures such as surgical precision and anatomical changes. Subjective patient-reported outcomes, including satisfaction and perceived quality of life, have gained prominence in recent years as critical indicators of success. These subjective results are influenced by multiple factors, including preoperative expectations, surgeon expertise, and individual variables such as age, gender, and psychosocial expectations.4 -6 Studies have highlighted those individuals who have realistic expectations and comprehensive preoperative counseling tend to report higher levels of postoperative satisfaction. 7 Some of the key challenges in assessing rhinoplasty outcomes include the variability of patient perceptions and the lack of universal measurement tools. To address this, various standardized questionnaires have been developed to evaluate changes in quality of life after the procedure such as the rhinoplasty outcome evaluation (ROE), sino-nasal outcome test, nasal obstruction and septoplasty effectiveness scale, and the Standardized Cosmesis and Health Nasal Outcome Survey (SCHNOS).8,9
The ROE is a reliable and widely used tool designed to measure both functional and aesthetic outcomes by evaluating psychological, emotional, and social dimensions. Its simplicity and ability to capture nuanced patient experiences make it a valuable resource for both clinical practice and research. 5
This systematic review and meta-analysis aim to evaluate patient satisfaction and quality of life after rhinoplasty, with a specific focus on the ROE questionnaire as a standardized measurement tool. The study seeks to identify factors that may influence these results. By synthesizing evidence from different studies, this research will provide a comprehensive understanding of the determinants of patient satisfaction and quality of life after rhinoplasty. Ultimately, the findings aim to guide surgeons in optimizing preoperative planning and postoperative care to achieve better patient-centered outcomes.
Materials and Methods
Literature and Strategy
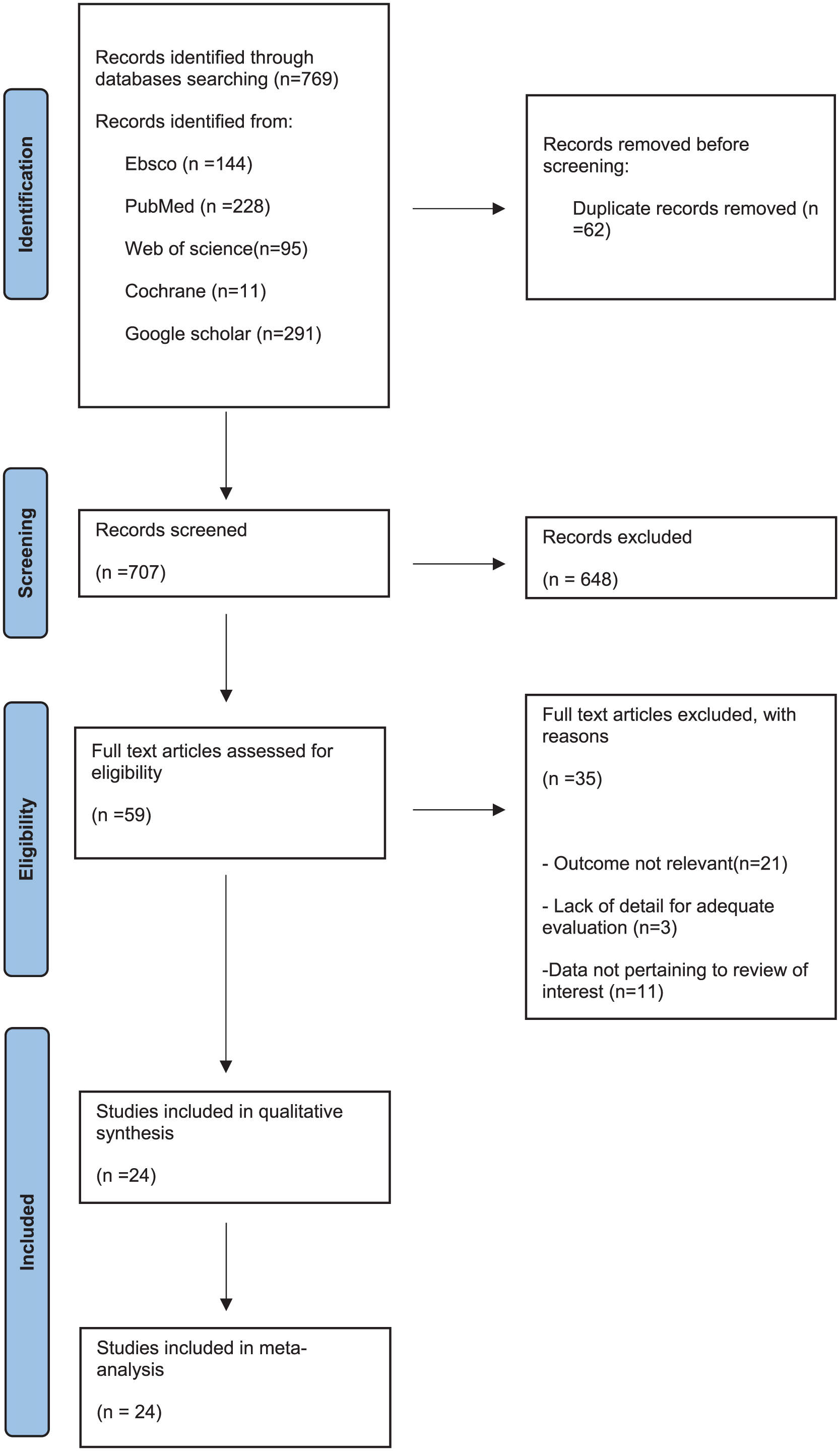
This systematic review and meta-analysis were registered in the International Prospective Register of Systematic Reviews (PROSPERO) with the registration number CRD42024572432. A thorough and detailed electronic search was conducted through the 5 main databases with a total of 769 studies, PubMed 228 studies, Cochrane Library 11 studies, Google Scholar 291 studies, EBSCO 144 studies, and Web of Sciences 95 studies for articles published from 2018 to 2024 in the English language.
The general search terms agreed on were converted into MESH terms with the use of PubMed: (Rhinoplasty OR Septorhinoplasty) AND (satisfaction OR prognosis OR outcome) AND (quality of life OR QoL) AND (ROE OR rhinoplasty outcome evaluation). Keywords were identified in the title, abstract, or heading of the topic.
Inclusion and Exclusion Criteria
This research included all studies published between 2018 and 2024 in English language, the studies reported the number of patients who underwent rhinoplasty surgery and evaluate quality of life or patient satisfaction after rhinoplasty. Studies that presented patient-related variables, use the ROE questionnaire, and present the overall ROE score or scores for individual questions. Additionally, the studies had to report results relevant to the clinical questions.
Exclusion criteria were studies not available in full text, studies that did not report ROE scores pre- and postoperatively, studies were not original articles (e.g., editorials, letters, commentaries), and duplicate studies, which were a total of 62.
Article Selection and Data Extraction
Two independent authors (A.A., R.S.) screened the included articles according to title and abstract through Rayyan followed by a full-text screening of eligible studies; duplicates were eliminated. Outstanding disagreements were resolved by 2 independent authors (S.A. and E.A.). Three independent authors manually extracted data (G.O., R.A., and L.A.), which included study information (author, year of publication, name of journal, country, study design and sample size), demographic data (gender and comorbidities), and results (total ROE score ± SD/median [range] pre- and postoperatively based on gender).
Assessment of Quality
To assess the risk of bias (ROB) and confounding for the primary studies, the Newcastle-Ottawa Scale (NOS) was used as a defined criteria to achieve a high-quality standard for transparent analysis of the publications. Studies assessed with a score of ≥5 were at low ROB.
Analysis of Data
The meta-analysis was conducted using R with the inverse variance method, using the restricted maximum likelihood estimator for τ2 and the Q profile method for the confidence interval of τ2 and τ. I2 was calculated based on the Q statistic. Additionally, the Hartung–Knapp adjustment was applied for the random effects model, and Hedges’ g was used as the bias-corrected measure of the mean difference (MD).
Results
ROB Assessment
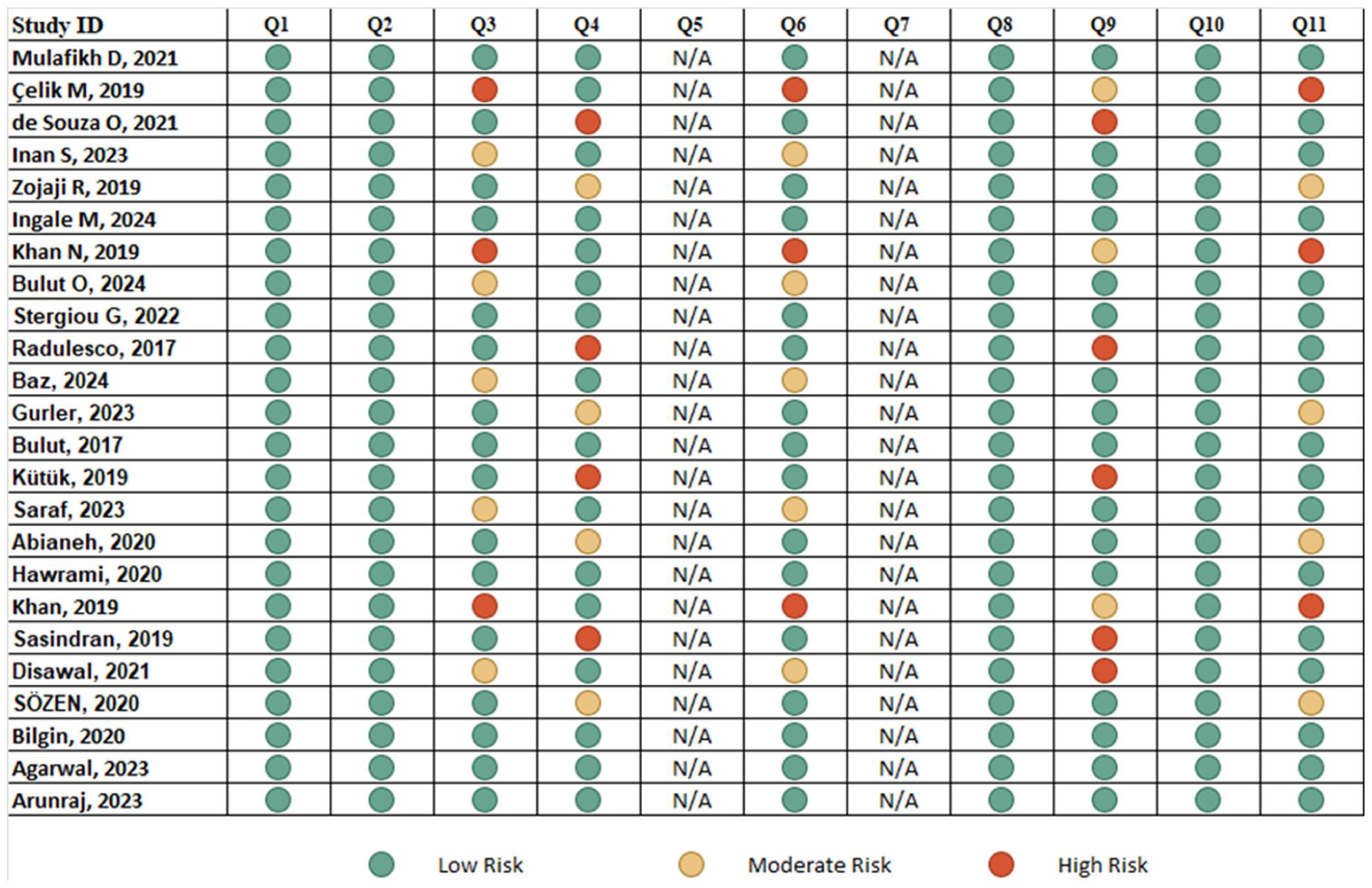
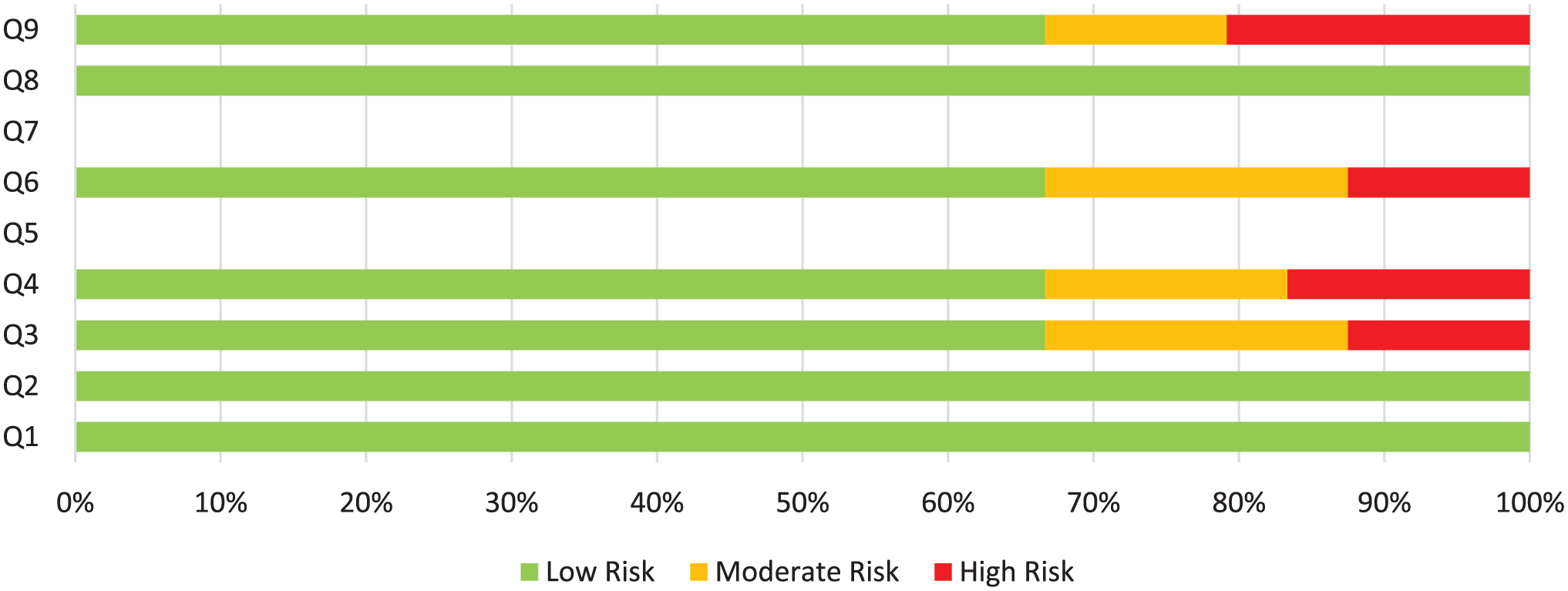
The ROB assessment for the primary studies was conducted using the NOS. Overall, most of the studies demonstrated a low ROB in key domains, including source of information (Q1), inclusion/exclusion criteria (Q2), and representativeness (Q3). However, there were areas of concern in some specific domains. Evaluator masking (Q5) was marked as “N/A” across all studies, it was either not applicable or not addressed. Confounding control (Q10) presented moderate-to-high risks in “Khan N 2019” and “Gurler 2023,” where confounding factors were not adequately controlled. Similarly, exclusions (Q9) were a concern in “Radulesco 2017” and “Disawal 2021,” where exclusions were either unclear or unjustified. Time period (Q4) raised moderate concerns in “Khaliq A 2020” and “Hawrami 2020,” due to lack of clarity or undefined time periods. Additionally, quality assurance (Q7) was consistently marked as “N/A” across all studies as it was not explicitly evaluated in the methodologies. However, “Baz 2024” and “Stergiou G 2022” had low risk across all domains due to robust methodologies.
*Q1, Source of info; Q2, Inclusion/exclusion; Q3, Representativeness; Q4, Time period; Q5, Evaluator masking; Q6, Standard methods; Q7, Quality assurance; Q8, Classification standards; Q9, Exclusions; Q10, Confounding control; Q11: Data completeness.
*Q1, Source of info; Q2, Inclusion/exclusion; Q3, Representativeness; Q4, Time period, Q5, Evaluator masking; Q6, Standard methods; Q7, Quality assurance; Q8, Classification standards; Q9, Exclusions; Q10, Confounding control; Q11, Data completeness.
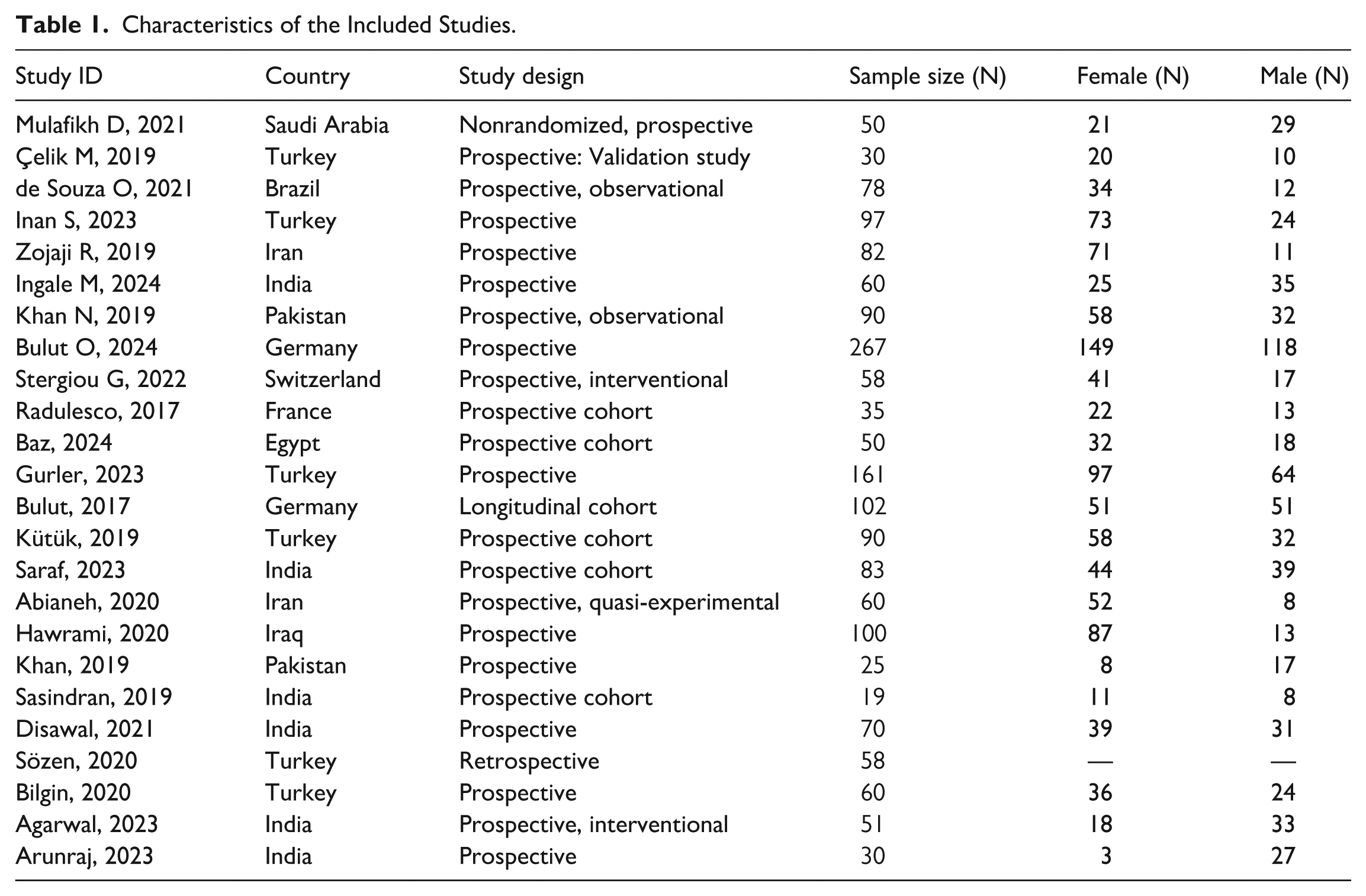
In this meta-analysis, we included 24 studies on rhinoplasty. The studies were from various countries including Saudi Arabia, Turkey, Brazil, and India. The total sample was 1806 patients. Gender distribution shows variability, with several studies having a higher number of female participants, such as Inan (2023) with 73 females and 24 males, and others showing a more balanced distribution, such as Gonçalves (2022) with 48 females and 44 males (Table 1).
Characteristics of the Included Studies.
A meta-analysis of 24 studies involving 1806 patients assessed the difference in ROE scores pre- and postoperatively. Using a random-effects model, the analysis revealed a significant overall improvement in ROE scores postoperatively, with a MD of 33.64 (95% CI [25.41, 41.87]), t = 8.50, P < .0001. Substantial heterogeneity was observed, with an I2 value of 99.8%, and the Q statistic for heterogeneity was 13814.71 (df = 21), P < .0001, and the between-study variance (τ²) was 13.0, indicating high variability in effect sizes.
These findings suggest that while ROE scores significantly improve postoperatively, the degree of improvement varies considerably between studies. This variation may be influenced by factors such as country, or patient population (Figure 1).
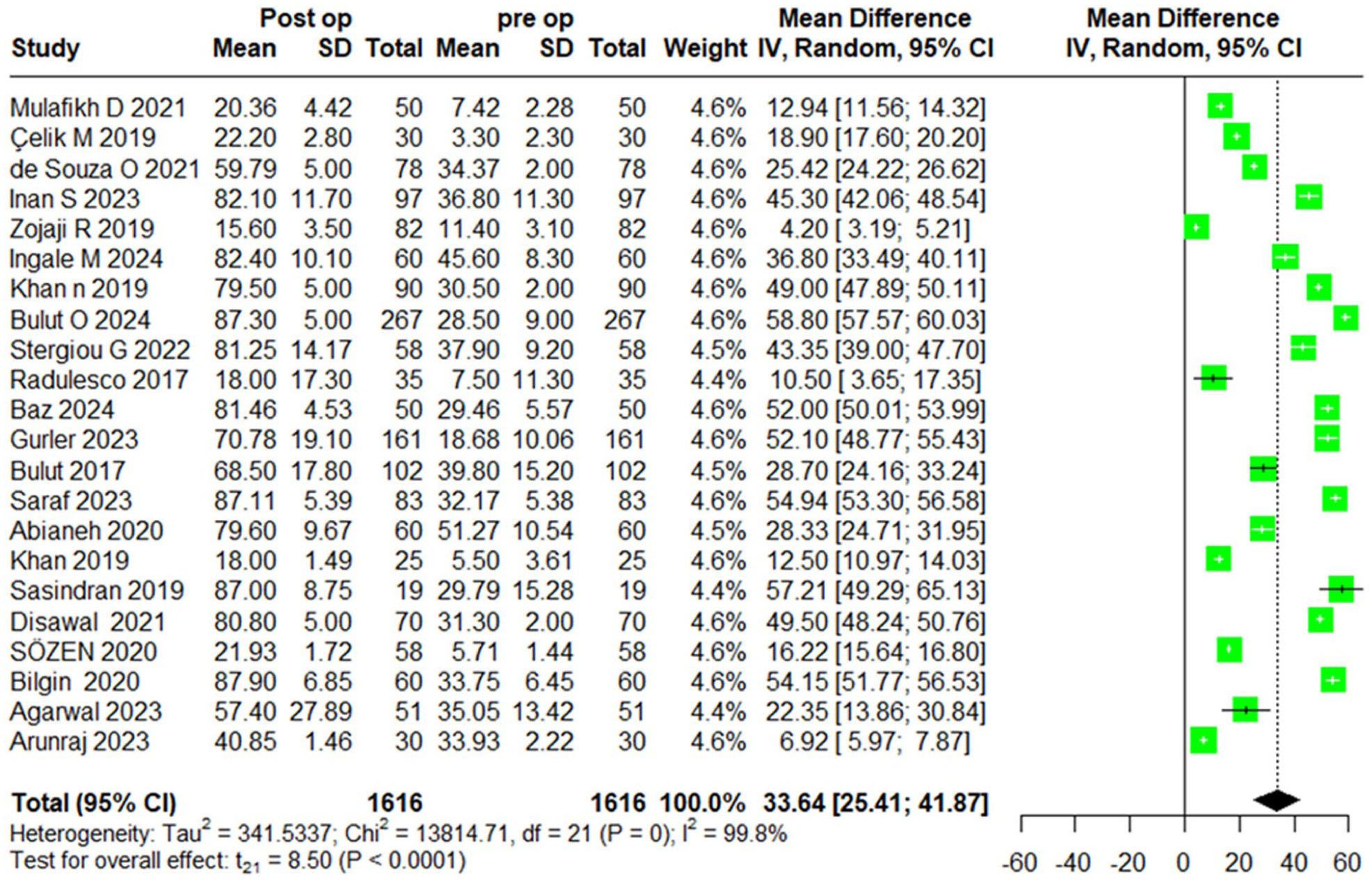
Pre- versus postoperative ROE score mean difference.
We also evaluated the preoperative differences in ROE scores between males and females. The random-effects model revealed a negligible difference between genders, with a MD of 0.44 (95% CI [−2.37, 3.26]), t = 0.37, P = .7207, indicating no significant gender-based differences in preoperative ROE scores. However, moderate heterogeneity was observed across the studies, with an I2 value of 78.4%, and the Q statistic for heterogeneity was 32.34 (df = 7), P > .0001, suggesting considerable variation in effect sizes. The τ2 was 7.9169 (Figure 2).
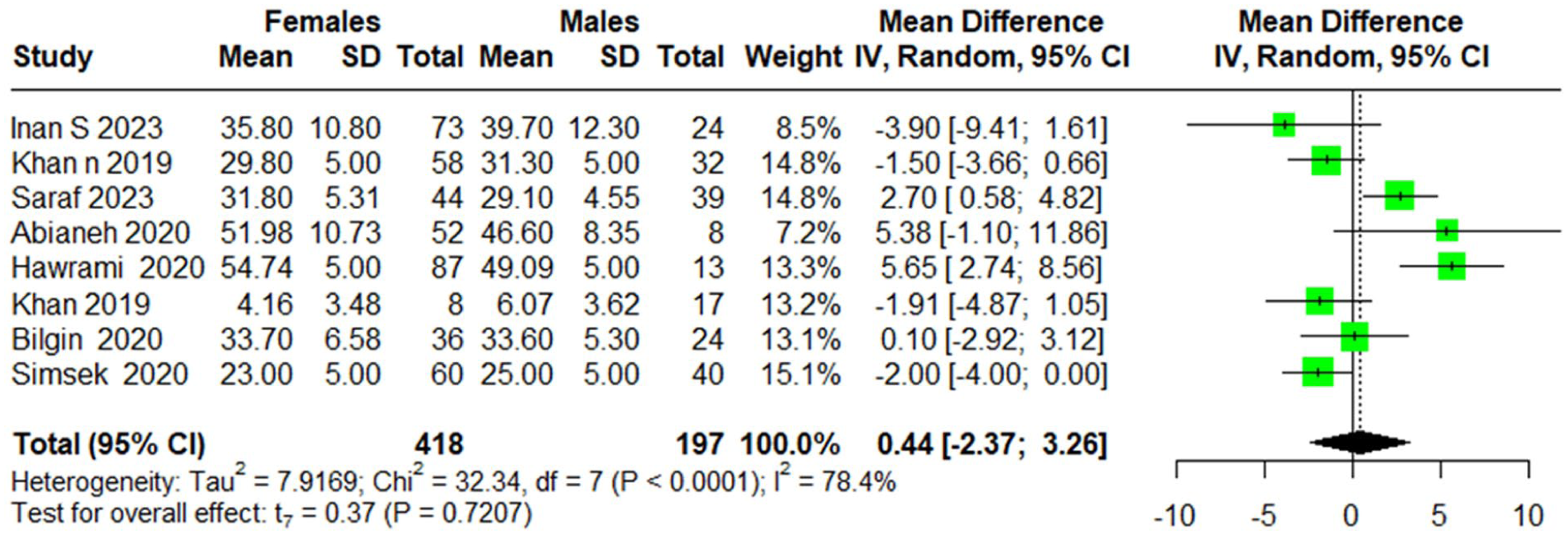
Preoperative difference in ROE between males and females.
Regarding postoperative differences in ROE scores between males and females, the random-effects model revealed a very small, nonsignificant difference between genders, with a MD of −0.7 (95% CI [−5.12, 3.71]), P = .7233, suggesting no significant gender-based differences in postoperative ROE scores. High heterogeneity was observed across the studies, with an I2 value of 94.6%, and the Q statistic for heterogeneity was 147.23 (df = 8), P < .0001. The τ2 was 30.1870 (95% CI [0.34, 3.23]; Figure 3).
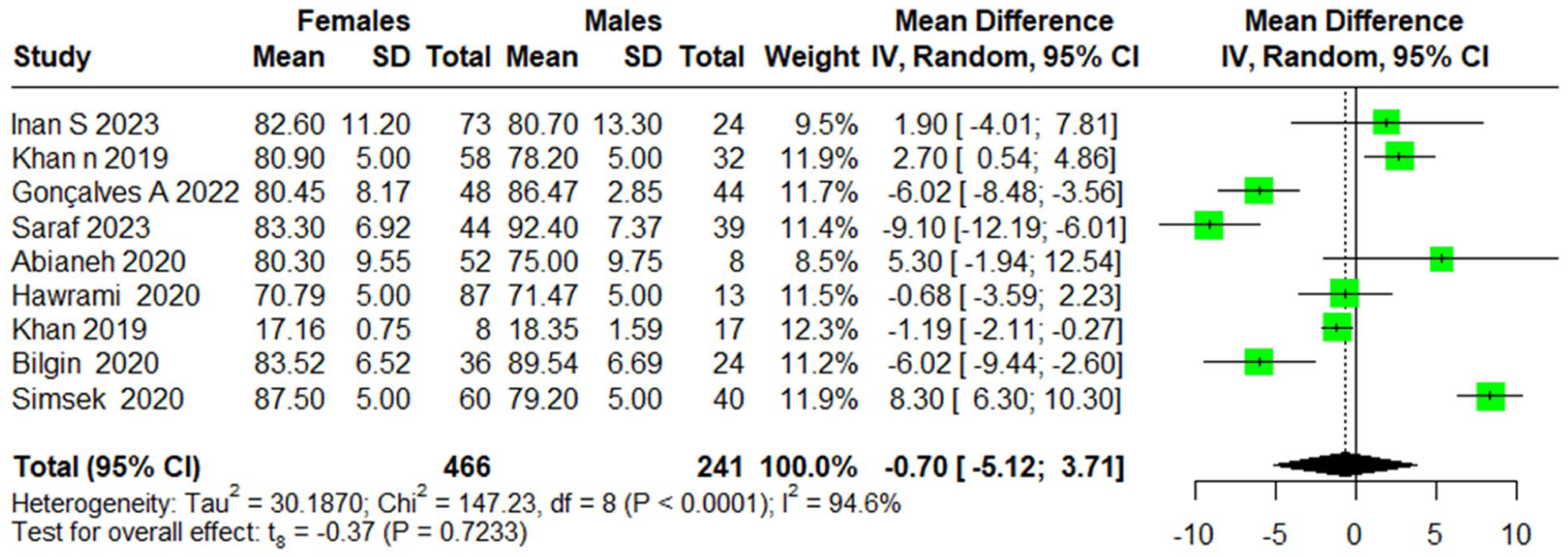
Postoperative difference in ROE between males and females.
Subgroup analysis based on country of origin revealed variation in effect sizes across regions. For instance, studies from Turkey (k = 5) showed a more pronounced improvement, with an MD of 37.29 (95% CI [14.46, 60.11]), and Brazil (k = 1) also indicated a significant improvement, with an MD of 25.42 (95% CI [24.22, 26.62]). In contrast, studies from countries such as Iran (k = 2) reported a less consistent effect, with an MD of 16.20 (95% CI [−137.10, 169.50]), and Pakistan (k = 2) showed substantial variability, with an MD of 30.75 (95% CI [−201.13, 262.64]). Notably, countries such as Saudi Arabia, France, and Egypt had fewer studies but showed consistent improvements with MDs of 12.94 (95% CI [11.56, 14.32]), 10.50 (95% CI [3.65, 17.35]), and 52.00 (95% CI [50.01, 53.99]), respectively (Figure 4).
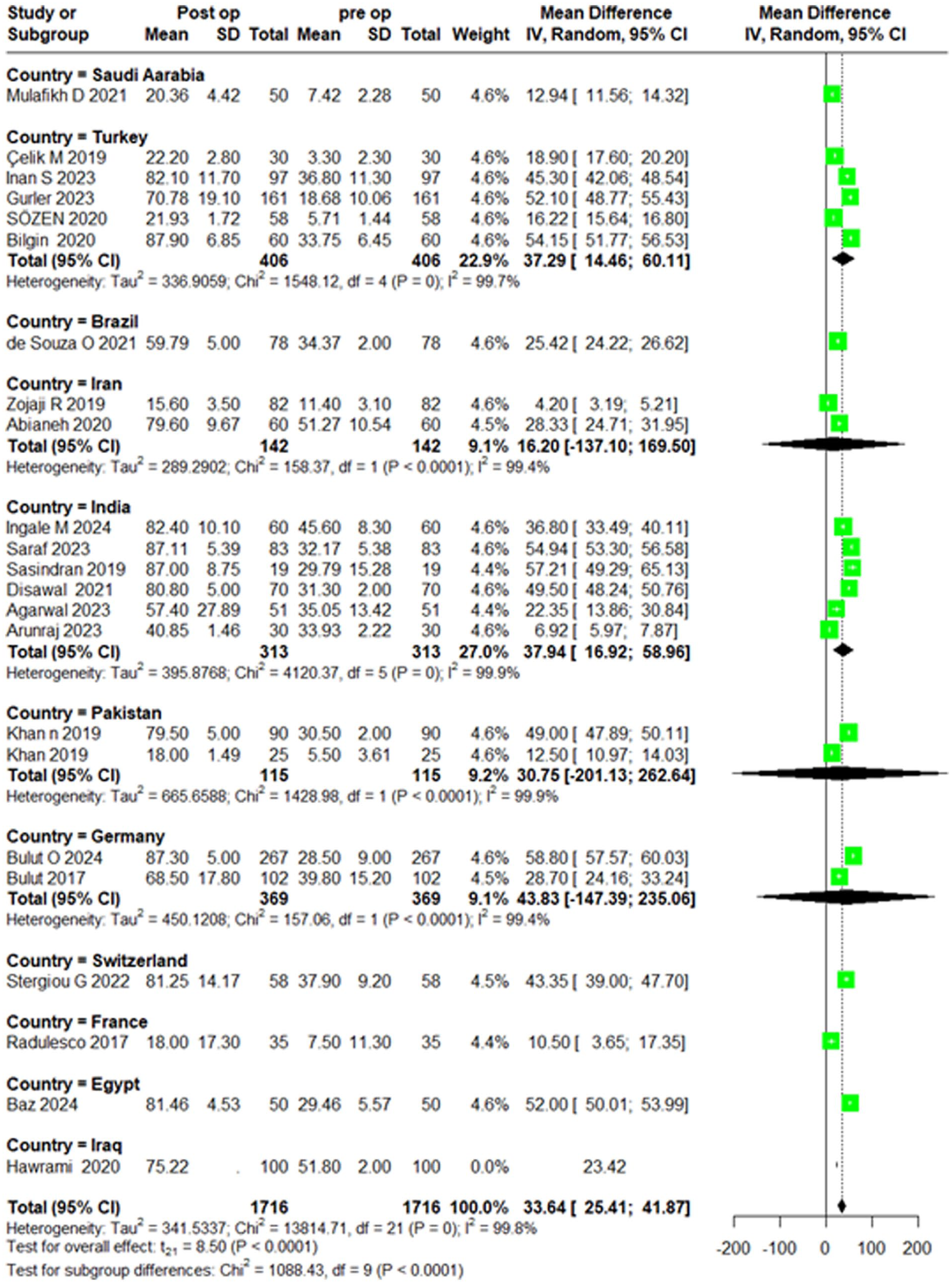
Pre- versus postoperative ROE score mean difference, sub grouped by country.
In ROE scores between preoperative and postoperative leave-one-out analysis shows that omitting any single study does not significantly alter the effect size or heterogeneity. All P-values are <.0001, demonstrating a highly significant improvement in ROE after surgery. In preoperative ROE scores between males and females leave-one-out sensitivity analysis reveals no major change in results by omitting individual studies. For postoperative ROE scores comparing males and females, leave-one-out analyses confirm the robustness of results, with no single study having a substantial impact (Supplemental Figure 5).
Discussion
The findings of this systematic review and meta-analysis underscore the significant impact of rhinoplasty on quality of life, as measured by ROE scores. The overall MD of 33.64 (95% CI [25.41, 41.87]), t = 8.50, P < .0001, indicates a substantial postoperative improvement in patient-reported outcomes. These results align with previous research demonstrating rhinoplasty’s role in enhancing not only facial aesthetics but also psychological well-being and functional respiratory outcomes.10 -13
The high heterogeneity in our meta-analysis (I2 = 99.8%) is likely attributable to several methodological differences across studies. Variations in study design, with retrospective studies being more prone to bias and incomplete data compared to prospective ones, affect the consistency of reported outcomes. Follow-up duration also differed, as early assessments may be influenced by edema and healing, while longer-term evaluations provide more stable reflections of satisfaction. Surgical approaches and indications were not uniform, encompassing both aesthetic rhinoplasty and septorhinoplasty, with differences in techniques such as open versus closed approaches and grafting methods influencing patient-reported outcomes. Population characteristics and sample sizes further contributed to variability, since age, gender, cultural expectations, baseline deformity, and study size (ranging from <20 to >250 patients) can all shape postoperative satisfaction. These factors together explain the substantial heterogeneity and emphasize the need for sensitivity and subgroup analyses, even though the overall evidence consistently supports improved quality of life and satisfaction after surgery.
The improvement in quality of life appears consistent across both genders. Preoperatively, no significant differences were observed between males and females (MD of 0.44, P = .7207), indicating comparable baseline expectations. Similarly, postoperative outcomes revealed no significant gender-based differences (MD of −0.7, P = .7233) These findings suggest that both male and female patients experience similar psychological and aesthetic benefits from rhinoplasty, consistent with earlier studies examining gender-specific satisfaction in facial aesthetic procedures.14 -16
These findings carry important implications for clinical practice. The substantial postoperative improvement in ROE scores reinforces the effectiveness of rhinoplasty in addressing both aesthetic and functional concerns. Considering the absence of significant gender-based differences, a patient-centered approach that prioritizes individual goals and expectations should be emphasized over reliance on generalized gender norms. Furthermore, the observed heterogeneity highlights the importance of thorough preoperative counseling and personalized surgical planning to optimize patient satisfaction and quality of life.17,18
Ethnicity, age, sex, culture, personal preferences, life experiences, and individual perceptions of beauty are key determinants of a person’s aesthetic choices. These factors can significantly influence the outcomes of cosmetic procedures, potentially leading to lower satisfaction levels when they are not adequately considered. To address this, many textbooks and guidelines propose ideal nasal measurements; however, several studies have shown that such standardized metrics may not be suitable for all ethnic groups, as many patients express preferences for nasal characteristics that differ from these norms.19 -22
Our findings demonstrated that ROE scores improved across all countries included in the analysis, though the extent of improvement varied. This is consistent with prior research conducted in diverse cultural contexts, which highlight those perceptions of nasal beauty are strongly influenced by ethnic background and geographic origin. These studies emphasize that applying universal nasal parameters may lead to patient dissatisfaction due to cultural and personal differences.23 -25 The substantial heterogeneity observed across countries in our meta-analysis may reflect contextual differences such as variations in patient demographics, healthcare systems, cultural norms, and ethnic characteristics rather than true differences in surgical effectiveness. These findings underscore the need to account for regional and population specific factors when interpreting pooled data and evaluating external validity in meta-analyses. Notably, there is a lack of research on nasal aesthetic preferences in Middle Eastern populations, highlighting the importance of region-specific studies to better inform surgical planning and improve patient satisfaction.
Despite the strength of the evidence presented, this systematic review and meta-analysis has several limitations. The inclusion of studies with varying methodologies, follow-up durations, and surgical techniques likely contributed to the observed heterogeneity. Nonetheless, this variability enhances the generalizability of our findings. Additionally, the use of self-reported outcome measures, such as the ROE score, introduces potential bias, as patient satisfaction may be influenced by psychological and social factors. However, we addressed this limitation by ensuring that the included data were derived from validated instruments and consistently reported outcomes. Future research should prioritize prospective, longitudinal studies using objective quality of life metrics and standardized surgical assessment tools to further clarify the long-term effects of rhinoplasty on patient well-being.
Conclusion
This meta-analysis confirms that rhinoplasty significantly improves patient satisfaction and quality of life. Both men and women benefit equally, emphasizing that gender is not a major factor in outcomes. Country of origin found to significantly affect ROE scores pre- and postoperatively, suggesting that perceptions of nasal beauty are influenced by ethnic background and country of origin. These findings highlight the importance of personalized counseling and surgical planning. Future research should explore cultural preferences and standardized approaches to enhance outcomes.
Limitations
While this review provides valuable insights, several limitations should be acknowledged. Variability in study designs, surgical techniques, and patient demographics across included studies may have contributed to the observed heterogeneity. The use of self-reported outcome measures, although widely accepted, introduces potential reporting bias. Additionally, the lack of standardized surgical protocols across studies may have limited direct comparability. Some populations were also underrepresented, which may affect the overall generalizability of the findings. Nevertheless, this review offers an important foundation for understanding patient-reported outcomes in rhinoplasty. Future research incorporating long-term follow-up, objective assessment tools, and more diverse population.
Supplemental Material
sj-docx-1-ear-10.1177_01455613251400561 – Supplemental material for Evaluation of Patient Satisfaction and Quality of Life in Patients Undergoing Rhinoplasty Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-ear-10.1177_01455613251400561 for Evaluation of Patient Satisfaction and Quality of Life in Patients Undergoing Rhinoplasty Systematic Review and Meta-Analysis by Enar Alotaibi, Laila Aldokhail, Ghadah Alotaibi, Rand Alshabnan, Aseel Alamoudi, Ghada Alsugair, Reem Alsugair, Mayar Alsaqr, Saleh Alabood and Ibrahim Alawadh in Ear, Nose & Throat Journal
Footnotes
ORCID iDs
Author Contributions
Enar Alotaibi conducted the literature search and creating data extracting sheet and resolved any outstanding disagreements in screening.
Laila Aldokhail exreacted data and writing disscussion and introduction.
Ghadah Alotaibi extracted data and wrote methods.
Rand Alshabnan extracted data and wrote abstract and conclusion.
Aseel Alamoudi and Reem Alsugair both screened literatures.
Ghada Alsugair wrote the results.
Mayar Alsaqr revised analysis, results, discussion, and final manuscript.
Saleh Alabood resolving any outstanding disagreements in screening.
Ibrahim Alawadh supervision and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.