
Abstract

Significance Statement
Transglottic carcinoma, first described by Jean Le Roux-Robert in 1936, is characterized by tumor infiltration and extension within the paraglottic space. Due to its concealed location, early symptoms are often subtle and nonspecific. Laryngoscopic examination may reveal only swelling of the false and true vocal folds, with an intact mucosal surface and no visible tumor. Histopathological diagnosis is often challenging, as superficial biopsies may not reach sufficient depth. Consequently, some patients undergo multiple inconclusive biopsies before a definitive diagnosis is achieved. 1
This study presents 3 recent cases of transglottic laryngeal carcinoma, highlighting sore throat accompanied by vocal fold swelling as a potential early clinical sign of this malignancy. We have obtained written informed consent from the patients.
Case 1: A 72-year-old male was admitted in October 2024 with acute dyspnea. Nasopharyngolaryngoscopy revealed bilateral vocal fold immobility and glottic stenosis (10/2024, Figure 1d). Notably, in 2021, the patient had undergone excision of a left vocal fold lesion previously diagnosed as a benign polyp following symptoms of sore throat and hoarseness (3/2021, Figure1a). Postoperatively, his hoarseness rapidly progressed, swelling of the left false and true vocal folds was observed by laryngoscopic evaluations, and no further evaluation was pursued (5/2021 and 10/2021, Figure 1b and c). He was eventually diagnosed with laryngeal squamous cell carcinoma.
Case 2: A 51-year-old male presented in September 2024 with a 2-month history of intermittent stabbing sore throat, without notable hoarseness. Despite treatment with antibiotics, acid suppressants, and anti-inflammatory agents, his symptoms persisted. Four successive laryngoscopic examinations over 2 months revealed progressive swelling of both the false and true vocal folds (6/2024, 7/2024, and 9/2024, Figure 1e-h). A definitive diagnosis of laryngeal squamous cell carcinoma was eventually established through deep tissue biopsy.
Case 3: A 68-year-old male was admitted in March 2024 with a 1-year history of sore throat and hoarseness. A glottic mass was noted (3/2024, Figure 1k). Over the preceding 8 months, he had undergone 2 biopsies for recurrent vocal fold lesions, both revealing moderate to severe dysplasia of the right vocal fold (6/2023 and 1/2024, Figure 1i and j). Ultimately, he was diagnosed with squamous cell carcinoma involving the left false vocal fold and the right true vocal fold.
While transglottic carcinoma is not currently recognized as a distinct subtype by the Union for International Cancer Control (UICC), 2 its unique clinical characteristics have prompted some researchers to advocate for its separate classification. 3 Originating in the laryngeal ventricle, this tumor typically extends submucosally into both the supraglottic and glottic regions via the paraglottic space. Such infiltration may produce early symptoms such as a sore throat, while laryngoscopy may only show vocal fold swelling without mucosal disruption, making early diagnosis difficult. 4 By the time hoarseness occurs, vocal fold fixation is often already present.
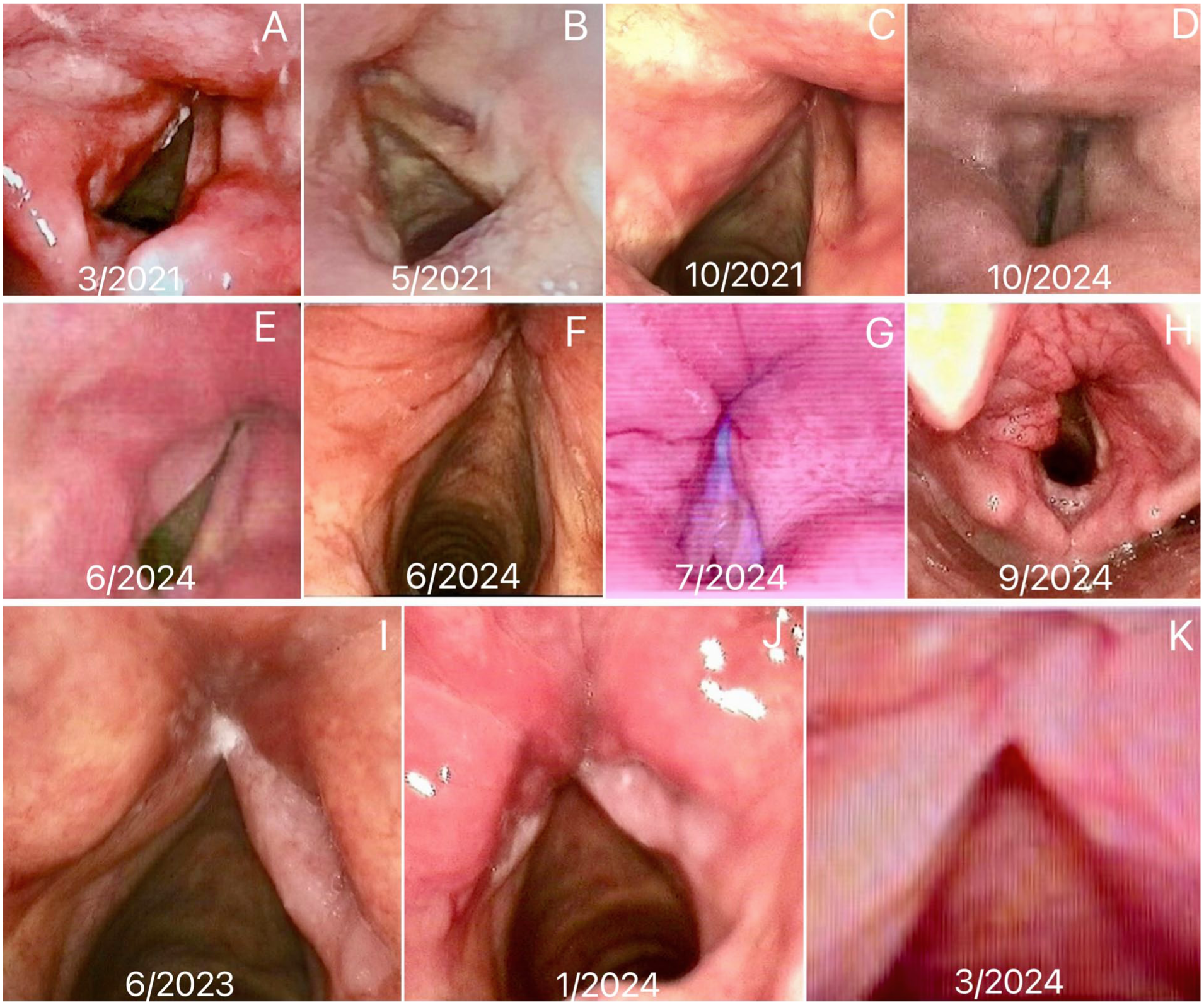
Case 1: (a) Preoperative laryngoscopy result. (b and c) Postoperative laryngoscopy results, he did not receive further diagnosis and treatment. (d) The laryngoscope result indicates bilateral vocal fold immobility.
Clinicians should consider transglottic carcinoma in the differential diagnosis of patients presenting with persistent sore throat and unexplained vocal fold swelling. To minimize the risk of misdiagnosis, biopsies should target submucosal tissues rather than superficial layers, thereby improving diagnostic accuracy.
Footnotes
Acknowledgements
The authors thank Mr. Yuzhang Zhou for his editing of the manuscript.
Ethical Considerations
This study was approved by the Ethics Committee of the Clinical Medical College of Xiangyang No.1 People's Hospital and conducted in accordance with the Helsinki Declaration.
Authors Contributions
Yali Liu and Fen Chen drafted the manuscript. Yuanyuan Wu analyzed the data. Guowei Ma approved the final version of the manuscript. All authors read and approved the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.