
Abstract
This case report describes a male patient with chronic invasive fungal sinusitis, mainly characterised by swelling of the eye. After a definitive diagnosis was made based on clinical symptoms and imaging studies, the patient received timely antimicrobial and symptomatic treatment, followed by functional endoscopic sinus surgery and orbital abscess drainage. The foci of infection in the sinuses were completely removed and adequate drainage of the sinuses was achieved, resulting in significant relief of the patient’s symptoms. The follow-up examination 1 month after discharge showed a good recovery.
Admission Details
A 56-year-old male patient was admitted with “swelling of the left upper eyelid for 4 days.” Four days prior to admission, the patient attended a local clinic for nasal congestion, purulent nasal discharge, and mild olfactory disturbance. No treatment was given, and the patient was admitted to the Ear, Nose, and Throat Department with a diagnosis of “chronic sinusitis.” On the day of admission, the left upper eyelid was markedly swollen (Figure 1). The patient was awake, the left eye had limited upward vision, the conjunctiva was congested and oedematous, and only the lower part of the cornea was visible due to the eyelid swelling, the anterior segment was clear, and the rest could not be examined. The right eye had normal vision. The patient reported childhood ocular trauma but did not seek medical attention. There was no history of chemical or radiation exposure, smoking or alcohol consumption, and no family history of similar diseases.
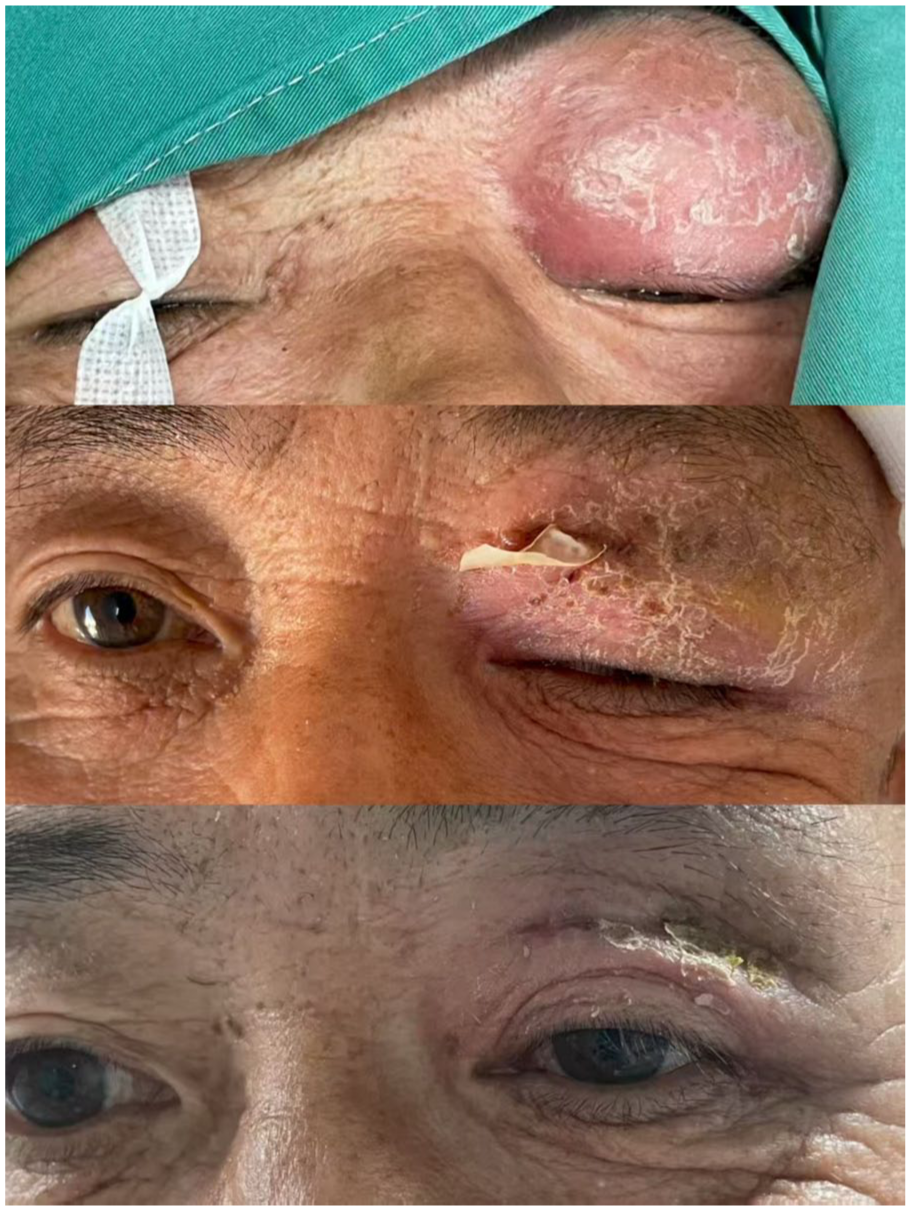
Changes in the patient’s eyes during treatment and follow-up.
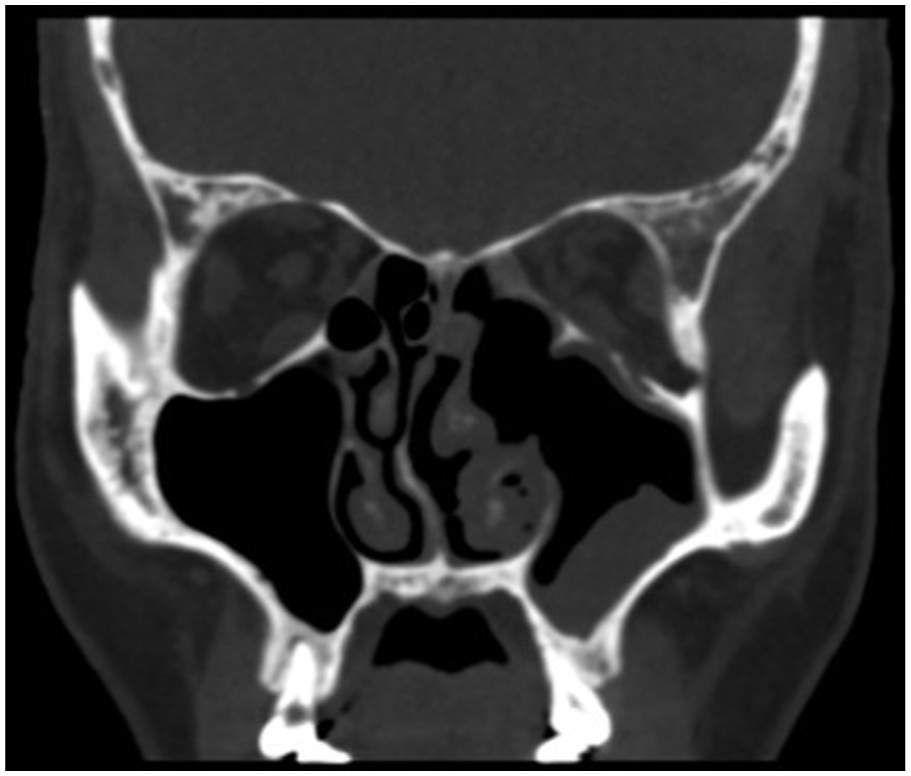
Blood Test: White blood cell count: 14.02 × 109/L, neutrophil percentage: 79.6%, lymphocyte percentage: 8.7%, monocyte percentage: 10.1%, absolute neutrophil count: 11.16 × 109/L, absolute monocyte count: 1.42 × 109/L. Prior to admission, an emergency computed tomography (CT) scan of the paranasal sinuses showed increased soft tissue shadows in the left paranasal sinuses and nasal cavity; irregularities in the left nasal bone and left middle and inferior turbinates, with possible bone resorption; protrusion of the left eye, intraocular gas accumulation, and increased soft tissue shadows with gas accumulation in the left eyelid and orbital region (Figure 2).
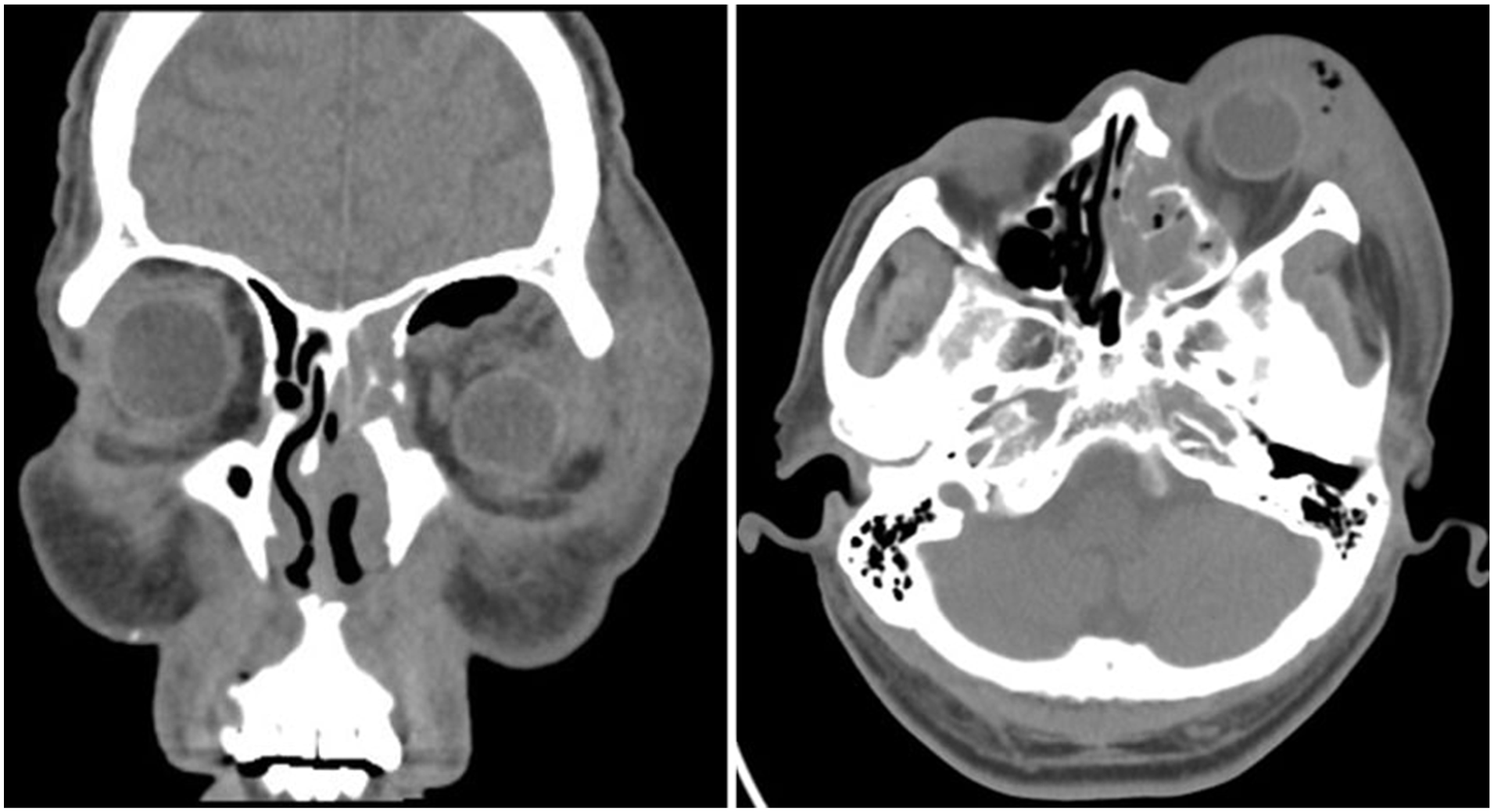
Sinus CT scan upon admission.
Treatment Procedure and Details
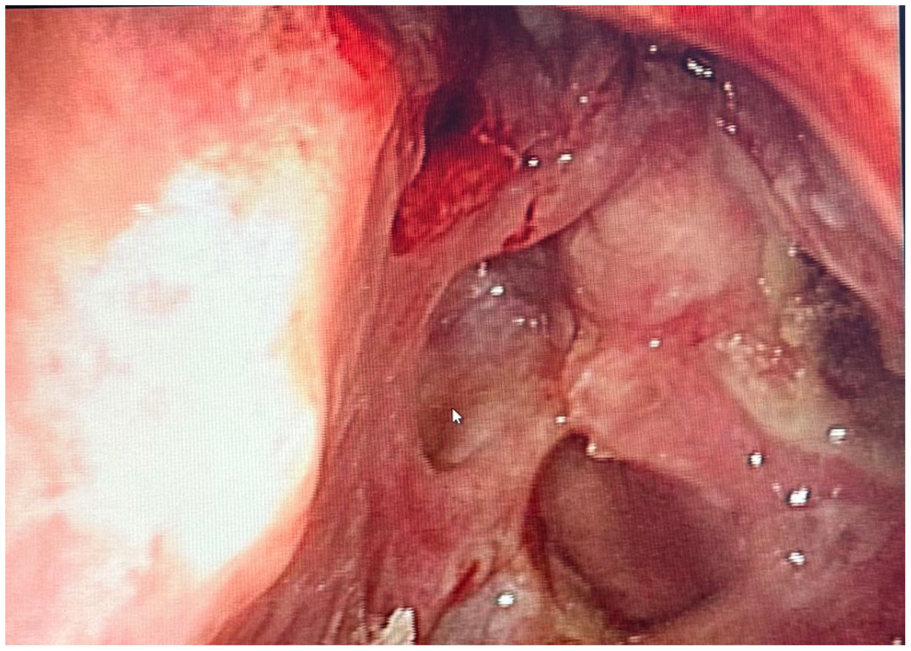
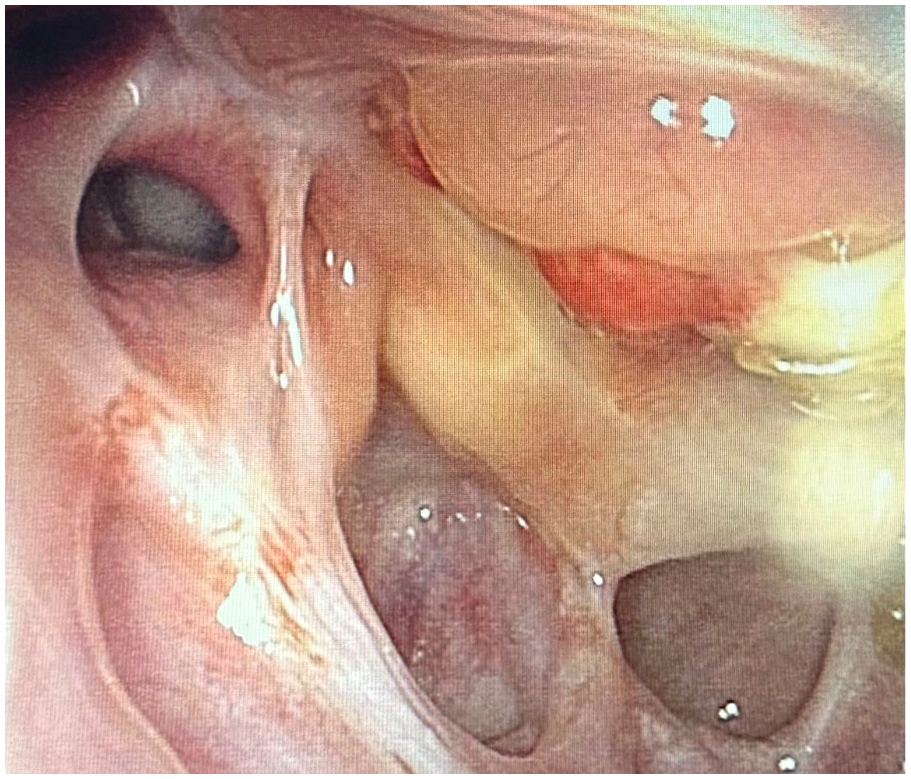
On admission, the patient received antimicrobial therapy: cefoperazone sodium 1.5 g, intravenous infusion, every 12 hours; dexamethasone 10 mg, once daily (QD); ornidazole 0.5 g, QD; fluconazole sodium chloride injection 0.2 g, topical application, QD; After an emergency CT scan, of the paranasal sinuses, surgery was performed on the second day of hospitalisation with multiple sinuses under nasal endoscopy. Part of the deposits were removed for pathological examination. The remaining sinuses on the left side were opened, and purulent secretions were removed from the sinuses. It was found that the upper half of the paper plate was damaged, and the orbital contents protruded into the nasal cavity. The opening of the frontal sinus was partially narrowed due to compression by the orbital contents. A large amount of secretion was removed with an aspirator (Figure 3). After the secretion had been removed, the abscess on the left upper eyelid had reduced significantly.
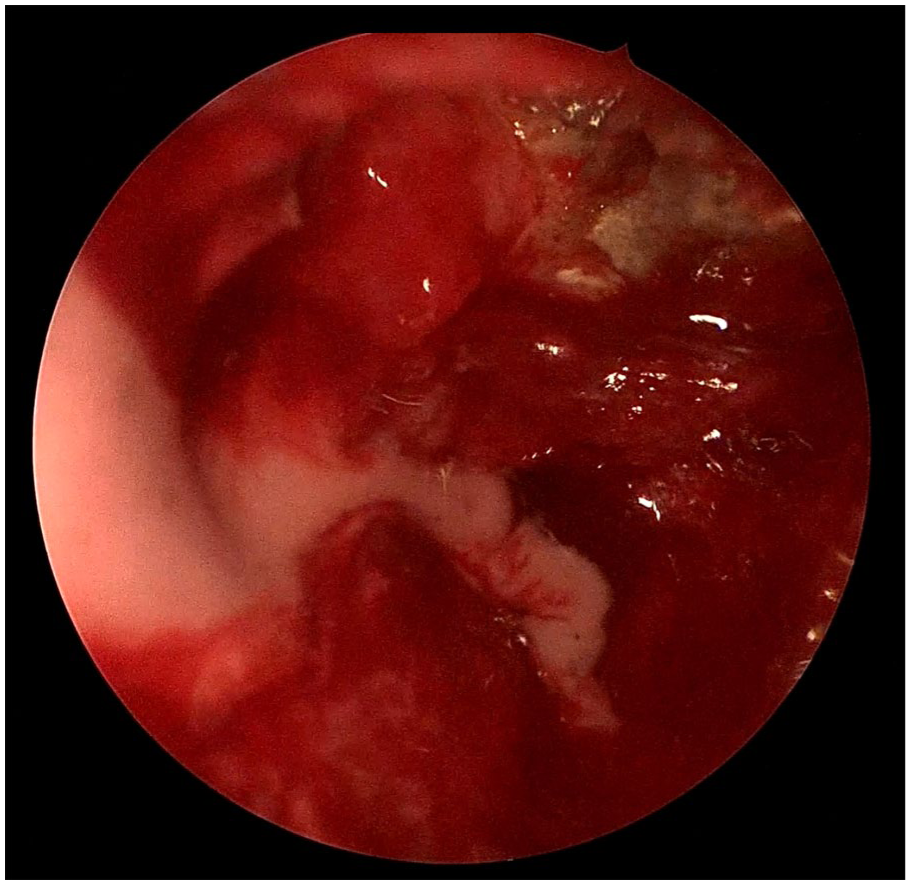
Intranasal endoscopic images of the sinuses during surgery.
Postoperative Pathological Macroscopic Findings
Several colourless hyphae and a small number of spores are observed. The hyphae are relatively uniform in thickness and appear elongated with acute-angled branching. A small number of lymphocytes and plasma cells infiltrate the margins (Figure 4). Postoperative treatment was continued with the original antimicrobial regimen. On the second postoperative day, the left upper eyelid continued to be swollen, similar to before admission. A sinus CT and cranial CT were immediately performed to rule out surgical complications, and an ophthalmological consultation was requested to assess the risk of further eye surgery. After the consultation, it was agreed to perform local anaesthesia for debridement and drainage of the left orbital abscess. During the operation, the most prominent part of the abscess was incised, and the pus was squeezed out thoroughly, sparing the eyeball. Hydrogen peroxide and saline were used during the operation for thorough disinfection, and a rubber gauze was placed for drainage postoperatively.
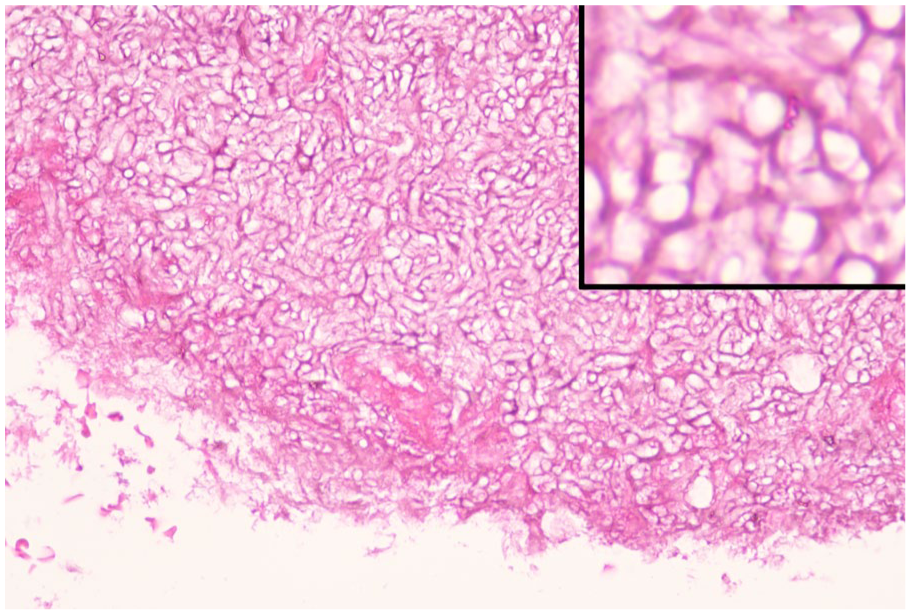
Light microscope pathology images.
On the second day after the eye operation, the swelling of the left upper eyelid had improved significantly. On postoperative day 5 after incision and drainage of the orbital abscess, a follow-up orbital CT scan showed irregularities in the medial wall of the left orbital sinus, maxillary sinus, and medial wall, swelling and gas accumulation around the left eye, and slightly increased density shadows in the left paranasal sinuses and nasal cavity, which primarily indicated inflammation (Figure 5). One week postoperatively, the patient was in a good general condition, and the abscess on the upper left eyelid had clearly receded. After thorough cleaning of the paranasal sinuses, the patient was discharged (Figure 6). Antibiotic therapy was continued for 1 week after discharge. One month after discharge, the follow-up examination revealed good recovery of all sinuses, no orbital abscess, and no other significant complaints (Figure 7).
CT scan of the eye socket after the second surgery.
Electronic nasopharyngoscopy 1 week after FESS surgery. FESS, functional endoscopic sinus surgery.
Electronic nasopharyngoscopy 1 month after FESS surgery. FESS, functional endoscopic sinus surgery.
Discussion
Invasive fungal disease is an infectious disease caused by fungi that invade the human body, grow and multiply in tissues, organs, or blood, leading to inflammatory reactions and tissue damage. The prevalence of invasive fungal infection (IFI) in Asian countries is generally 3 to 15 times higher than in Western countries. 1 In Europe, haematological malignancies are the most common underlying disease associated with IFI, 2 while in lower-income Middle Eastern and North African countries, diabetes is the most common. IFI can affect multiple systems throughout the body, but involvement of the nasal cavity and paranasal sinus mucosa is relatively rare in clinical practise. There is currently little epidemiological data on IFI. Invasive fungal rhinosinusitis (IFRS) is an infectious disease characterised by the invasion of fungal hyphae into the nasal cavity and paranasal sinus mucosa and bone walls, leading to inflammatory reactions and tissue damage in adjacent structures such as the orbital cavity, the anterior cranial fossa, or the pterygopalatine fossa. 3 The most common pathogens are Mucor and Aspergillus.
Aspergillus fungi are opportunistic pathogens with a strong ability to multiply, which thrive optimally at temperatures between 25 °C and 30 °C. They form filamentous colonies. They form filamentous colonies, with over 95% of human cases of aspergillosis being caused by Aspergillus fumigatus. 4 Infection occurs through inhalation of airborne Aspergillus spores, with the lungs being the most common site of infection, but the sinuses are also an important target for infection. 5 Aspergillus hyphae have a uniform thickness, branch at their tips at an angle of 45°, and have a diameter of 2 to 4 μm. A special colouration shows septa. 6 Confirmation requires tissue biopsy, microscopic examination, and/or direct observation of the septate, branching hyphae during recovery of the organism. Identification of colony morphology and sporulation further refines the diagnosis. 7 In contrast to mucormycosis, which often affects patients with systemic diseases and weakened health, sinus-orbital aspergillosis can also occur in immunocompetent individuals. 8 Immunocompetent patients mainly come from tropical countries where a humid climate favours fungal growth and leads to a high concentration of spores in the environment. 9 Studies suggest that impaired drainage of the paranasal sinuses leads to local hypoxia. 10
Aspergillus fumigatus binds to laminin and fibrinogen, which may play a key role in tissue invasion. 11 Aspergillus fumigatus has a significantly weaker invasive capacity than Mucor species. 12 Histologically, extensive mucosal necrosis, vasculitis, and thrombosis are relatively rare, whereas epithelioid cell granulomatous reactions are frequently observed. Although clinically characterised by a chronic course, the disease can nevertheless invade blood vessels, the walls of the paranasal sinuses, and the ethmoid plate and penetrate the orbit, where it may spread intracranially and be fatal. 13 Early treatment is recommended for patients who are clinically diagnosed with an IFI. From the combination of clinical symptoms, imaging findings, intraoperative observation of grey-green, cheesy fungal material, and smears of secretions, systemic antifungal combination therapy should be initiated immediately. 14 Three main classes of antifungal agents are used clinically: polyene antifungals (amphotericin B), azole antifungals (itraconazole and voriconazole), and new formulations (eg, nystatin liposomes and echinocandin). 15 Studies suggest that in immunocompetent patients, local surgical debridement in combination with antifungal therapy leads to favourable outcomes.15,16
Based on the clinical course of the disease, fungal sinusitis is divided into IFRS and non-IFRS, depending on whether it is invasive. Among these, IFRS is further subdivided into acute IFRS (AIFRS), chronic IFRS (CIFRS), and granulomatous IFRS. 17 This case belongs to CIFRS. CIFRS begins insidiously, progresses slowly, and usually lasts longer than 12 weeks. It mainly affects the ethmoid and sphenoid sinuses, with Aspergillus being the most common pathogen. The main symptoms include nasal and facial pain, epistaxis, swelling and numbness of the face, proptosis, blurred vision, diplopia, and impaired eye movements. 18 A study involving 1370 patients indicates the following: diabetes, age, hypertension, white blood cell count, percentage of lymphocytes, percentage of neutrophils, C-reactive protein, blood glucose level, and glycated serum albumin are risk factors for IFRS. Diabetes and white blood cell count are independent risk factors for IFRS. 19
CIFRS is pathologically very similar to AIFRS. However, it occurs more frequently in individuals with normal immune function, and its course is slower (from months to years), with more subtle symptoms. 20 The clinical manifestations in the early stages of this disease are non-specific and similar to those of chronic rhinitis and sinusitis. In the middle and late stages, the clinical manifestations closely resemble those of malignant sinus tumours, leading to a high incidence of misdiagnosis. 21 Therefore, the selection of diagnostic methods with high accuracy and clinical value to support the clinical diagnosis and the clear identification of the disease type at an early stage are key to improving the prognosis. The combination of CT and MRI can provide reliable evidence for the clinical diagnosis of CIFRS. 22 In addition, histopathological confirmation of fungal cell invasion into the tissue is the gold standard for the diagnosis of IFRS. The presence of fungal hyphae and/or spores in subcutaneous tissue in a biopsy sample can confirm the diagnosis. Positive results from microbiological fungal testing of clinical samples can further aid in confirmation. Currently, the most informative and diagnostically valuable approach is the combined use of several microbiological methods, including the G-test, the G-test in combination with polymerase chain reaction, fungal culture, and fungal smear microscopy. 23
Similar studies from home and abroad show that the treatment of IFS should follow a 3-pronged approach, which includes surgical debridement of necrotic tissue, administration of systemic antifungal medications, and reversal of immunosuppression. There is limited consensus in the literature regarding the specific management of orbital disease. 24 Orbital exenteration is the most aggressive treatment option for orbital disease, but there is limited data to support its survival benefit. Turner et al found in a meta-analysis of 807 IFS patients that surgical debridement is an effective measure to improve prognosis, but no association was found between orbital exenteration and survival. 25 Similarly, Hargrove et al reviewed 224 published cases of mucormycosis and found that only organ resection in febrile patients improved survival. 26 Literature reports suggest that neutropenia is a major risk factor for mortality in IFS, and that immunomodulatory therapy (such as Granulocyte-macrophage colony stimulating factor [GM-CSF]) may play an adjunctive role, but further research is needed to confirm this. 27 Despite decades of effort, the prognosis for IFRS patients remains unfavourable, particularly for AIFRS. Key factors influencing prognosis include age, underlying conditions, timing of diagnosis and treatment, postoperative antifungal therapy, and regular follow-up. Piromchai and Thanaviratananich 28 found that patients who underwent surgical treatment (endoscopy preferred) within 2 weeks of symptom onset had a higher survival rate than those who were treated after 2 weeks. In addition, the site of fungal invasion has a significant impact on prognosis, with a higher mortality rate for intracranial infestation compared to other sites, and a higher disability rate for orbital infestation compared to other sites. Zygomycetes infections are associated with poorer visual outcomes. Timely functional endoscopic sinus surgery (FESS) debridement is associated with better visual outcomes, more surgical interventions, and a lower mortality rate. 27
Following a definitive diagnosis, the patient in this case underwent antibiotic therapy combined with FESS surgery and local orbital debridement and drainage. The patient in this case had no history of immunodeficiency diseases or diabetes, which improved the postoperative recovery results. As the patient had a fracture of the left orbital wall, the surgery was challenging. Although the frontal sinus, maxillary sinus, ethmoid sinus, and sphenoid sinus were thoroughly opened during surgery, the orbital contents were found to protrude from the opening of the frontal sinus, resulting in inadequate drainage of the frontal sinus. The day after surgery, it was noted that the abscess had not regressed significantly. An ophthalmologist was consulted immediately, and it was agreed to perform orbital abscess debridement and drainage under the premise of protecting the patient’s vision and safety, which led to good results. The literature supports our treatment approach and recommends that treatment should focus on local control as long as there is no evidence of a significant burden of infection in the orbit, preserving viable tissue, with the knowledge that more aggressive options can be rapidly implemented if required. 27 One week and 1 month postoperatively, electronic nasopharyngoscopy showed unobstructed drainage in all sinuses, with no fungal debris or other tissue. The patient’s vital signs were good.
Conclusion
In summary, FESS surgery combined with orbital abscess drainage and targeted antibiotic therapy yields excellent results. During treatment, it is important to closely monitor changes in the patient’s condition. For example, performing a second eye surgery in a timely manner can help control the progression of the disease and improve the patient’s prognosis. In the early stages of the disease, due to the rapid deterioration of the condition, it is essential to make an early and accurate diagnosis and initiate targeted antibiotic therapy, which can lead to a better prognosis. There are also reports in the literature that multiple surgeries can improve patient survival rates.
Footnotes
Acknowledgements
We would like to thank the Otolaryngology Department team at Central Hospital of Dalian University of Technology for their assistance with data collection and paper revision.
Ethical Considerations
This is an observational study. The Research Ethics Committee of Central Hospital of Dalian University of Technology has confirmed that no ethical approval is required.
Consent for Publication
This study has obtained written informed consent from patients, whose anonymous information and clinical data will be published in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analysed in the current study are available upon reasonable request to the corresponding author.