
Abstract
We present the case of a 7-week-old female with a segmental, beard-distributed infantile hemangioma, and acute upper airway obstruction. The patient presented with progressive stridor and respiratory distress, prompting urgent evaluation. Bedside flexible laryngoscopy was inconclusive due to patient distress, but operative direct laryngoscopy and bronchoscopy revealed near-circumferential subglottic hemangioma, necessitating endotracheal intubation for airway protection. She was transferred to a tertiary care center for multidisciplinary evaluation and management. Given the distribution of the hemangioma and airway involvement, PHACE syndrome was strongly considered. MRI and MRA of the brain and neck demonstrated no cerebral or large vessel anomalies, though extensive hemangiomatous involvement of the facial and deep neck soft tissues was noted. Echocardiogram and ophthalmologic evaluations were unremarkable. The patient underwent direct laryngoscopy, bronchoscopy, and intralesional Kenalog injection into the supraglottic and subglottic hemangioma. Propranolol was initiated with favorable clinical and radiographic responses. This case emphasizes the importance of early airway evaluation in infants with beard-distributed hemangiomas and highlights the role of comprehensive PHACE syndrome workup. It demonstrates the utility of early propranolol therapy and steroid injection in the management of airway-compromising hemangiomas.
Keywords
Introduction
Infantile hemangiomas (IHs) are the most common benign vascular tumors of infancy, affecting ~4% of infants, with risk factors including prematurity and female sex. 1 IH expression of glucose transporter-1 (GLUT-1) differentiates them from other vascular tumors or vascular malformations. Although not completely understood, 1 hypothesis for IH development is hypoxia-induced vascular proliferation. Hypoxic conditions, such as prematurity, induces neovascularization and angiogenesis through expression of angiogenic factors vascular endothelial growth factor (VEGF) and basic fibroblast growth factor (bFGF). 2 IHs are typically not present at birth but appear within the first few weeks of life. The natural progression of IHs is divided into 3 phases: proliferative (0-1 year), involution (1-5 years), and involuted (5-10 years). The proliferative phase is marked by the fastest growth velocity of the lesion. The involution phase represents the beginning of lesion fading, and the involuted phase reflects near-complete or complete regression. 3
IHs are not only most commonly localized but can also present as segmental, plaque-like lesions that often exceed 5 cm in diameter. When segmental or located in high-risk areas, IHs can lead to life-threatening complications. 2 Segmental hemangiomas in a “beard” distribution involving the chin, lower lip, anterior neck, and preauricular regions are clinically significant, as they have a strong association with airway hemangiomas and may signal the presence of PHACE syndrome. 4 Airway hemangiomas raise concern for significant airway obstruction, especially in the subglottic and glottic regions, and commonly present with stridor, hoarseness, and respiratory distress. 5 Early recognition and intervention are critical to prevent life-threatening airway compromise. Risk of PHACE syndrome, a neurocutaneous disorder characterized by posterior fossa brain malformations, hemangioma, arterial anomalies, cardiac anomalies, and eye abnormalities, is associated with beard-distributed hemangiomas. Up to 31% of infants with large, segmental hemangiomas on the face may meet criteria for PHACE syndrome. 6
We describe a rare case of a full-term, otherwise healthy infant presenting with acute respiratory distress due to suspected circumferential subglottic hemangioma, later managed successfully with airway stabilization, intralesional steroid therapy, and initiation of propranolol. This case underscores early detection and intervention through a multidisciplinary approach for infants with complex vascular anomalies and suspected PHACE syndrome.
Case Presentation
A 7-week-old female, born full-term via cesarean section to a healthy 32year-old mother, presented with sudden onset of stridor and respiratory distress. Her past medical history was unremarkable aside from a progressively enlarging right-sided facial rash noted since birth, consistent with an IH in a beard distribution. On the morning of presentation, the infant developed suprasternal retractions, tracheal tugging, and increased work of breathing.
She was evaluated at a local community emergency department where bedside flexible laryngoscopy was attempted but was limited due to infant distress. Given concern for airway involvement, she was taken to the operating room for a definitive airway with simultaneous operative laryngoscopy and bronchoscopy. Findings included hemangiomatous involvement of the supraglottic larynx, right arytenoid, epiglottis, and near-circumferential subglottic narrowing (Figure 1). The patient was intubated intraoperatively and transferred to a tertiary pediatric hospital for further evaluation.
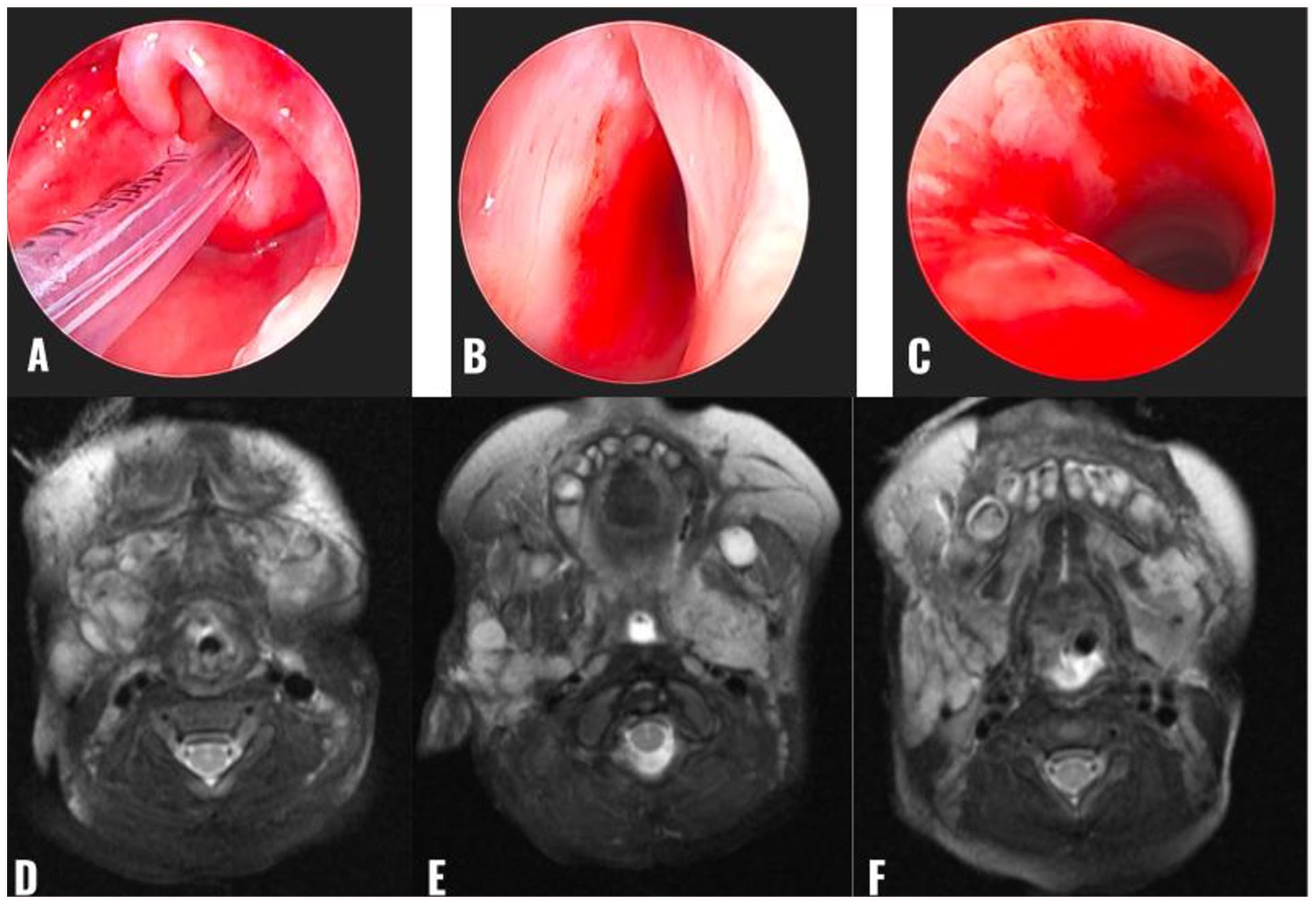
Comparing direct laryngoscopic visualization with MRI findings in the setting of multiple vascular malformations. (A) Supraglottic view showing vascular lesions to the supraglottic larynx, right arytenoid, and epiglottis. Also seen is a tight right AE fold, further complicating this pediatric airway. (B) Glottic view visualizing vascular lesion just inferior to the left vocal cord. (C) Subglottic view showing circumferential vascular lesion. (D–F) Representative axial, T2-weighted MRI with hyperintense, septated, lobulated hypervascular lesions bilateral. AE, aryepiglottic.
Upon arrival, the patient remained intubated and sedated. MRI with and without contrast of the brain and neck revealed extensive hemangiomatous enhancement throughout the bilateral facial and deep neck spaces, with no definite subglottic lesion visualized radiographically (Figure 1). MRA of the head and neck was unremarkable. Echocardiography and ophthalmologic evaluations were within normal limits. No additional features of PHACE syndrome were identified, though close follow-up was arranged.
On hospital day 2, the patient underwent suspension laryngoscopy with intralesional Kenalog (triamcinolone) injection into the subglottic and supraglottic hemangioma. Propranolol was initiated at 1 mg/kg/day and titrated to 2 mg/kg/day. The patient tolerated treatment well, with noted improvement in cutaneous hemangioma and decreased stridor (Figure 2). She was successfully extubated on hospital day 5 to high-flow nasal cannula and transitioned to room air by day 6. Repeat swallow evaluation revealed safe oral intake, and the patient resumed bottle feeding.
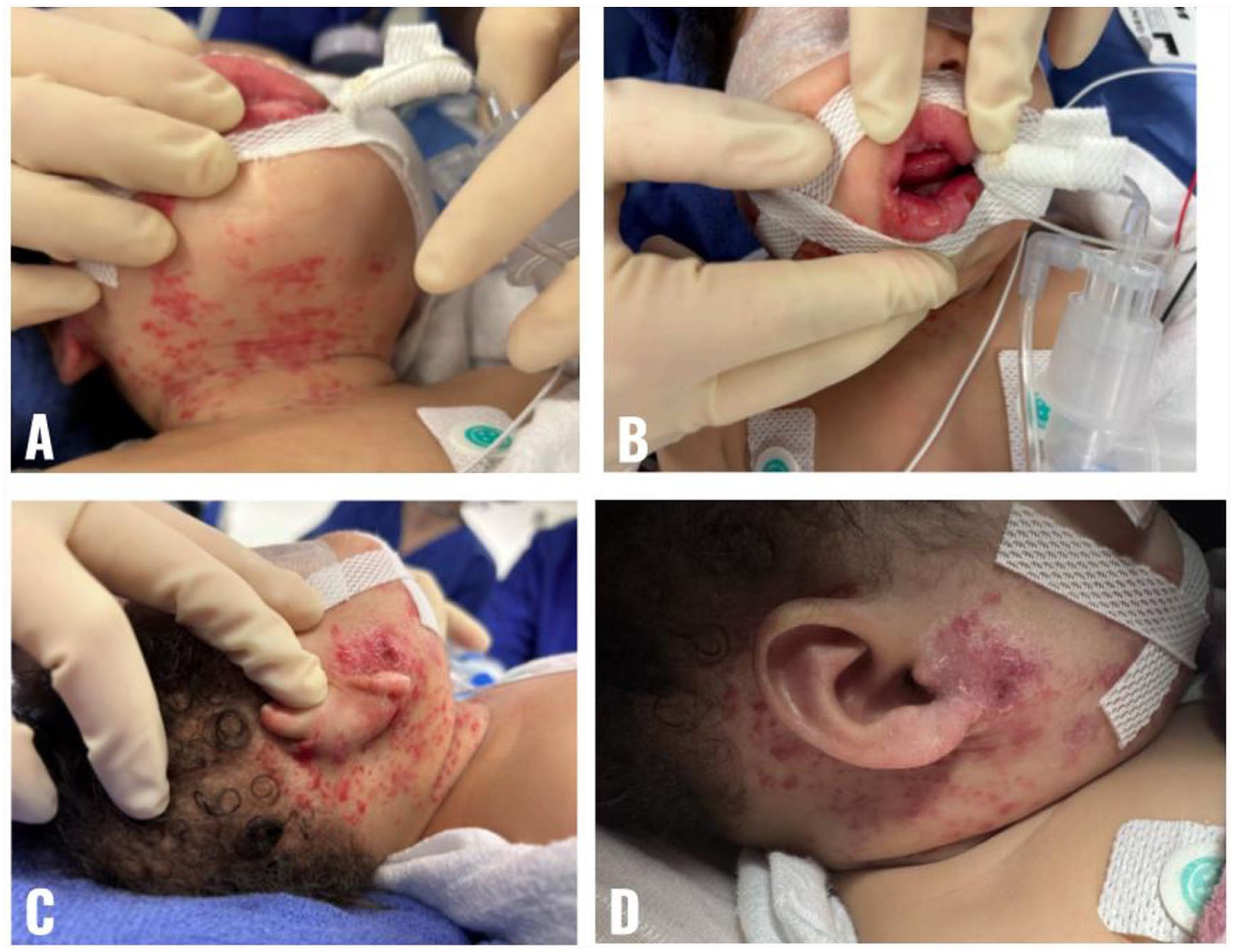
Segmental infantile hemangioma in a “beard” distribution treated with propranolol. (A–C) Pretreatment of vascular lesions involving the anterior neck, lower lip, and right peri-auricular area. (D) Interval improvement of right peri-auricular hemangioma after initiating oral propranolol.
Discussion
Segmental hemangiomas in a beard distribution warrant high clinical suspicion for concurrent airway involvement and associated anomalies, such as PHACE syndrome. 7 In this case, the infant’s sudden decompensation underscores the importance of early ear, nose, and throat (ENT) involvement and airway assessment. Operative endoscopy remains the gold standard for diagnosis and delineation of airway hemangiomas. 8
While MRI and MRA are essential for evaluating PHACE features, imaging may underestimate the extent of airway hemangioma, particularly when mucosal and submucosal components are involved. In our case, MRI failed to visualize subglottic disease identified on endoscopy, highlighting the limitations of imaging alone in airway evaluation.
Propranolol has revolutionized the treatment of IHs, with high efficacy in both cutaneous and airway lesions. 9 Intralesional corticosteroid injection can provide additional localized control, particularly in critically narrowed airways. 10
This case reinforces the need for comprehensive, multidisciplinary evaluation including ENT, dermatology, cardiology, ophthalmology, and vascular anomalies specialists. Follow-up is essential, especially given the potential for rebound growth or late-onset complications.
Conclusion
Infants presenting with beard-distributed hemangiomas and respiratory symptoms should be urgently evaluated for airway involvement and PHACE syndrome. Operative airway endoscopy is critical for diagnosis when imaging is inconclusive. Combined intralesional steroid injection and systemic propranolol therapy are effective treatments, and multidisciplinary follow-up ensures optimal long-term outcomes. This case illustrates a rare but high-stakes presentation that emphasizes vigilance and coordination in pediatric airway management.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases.
Consent for Publication
Written informed consent from the patient’s legally authorized representative was obtained for publication of this case.
Author Contributions
Trevor Creamean: writing—review and editing, figure creation, literature review, investigation. Andrew Steehler: conceptualization, supervision, writing—original draft. Kristina Kazimir: writing—review and editing. Kathryn Deeds: investigation, supervision. Allison B.J. Tobey: investigation, supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.