
Abstract
Background:
Mucormycosis is a rare but life-threatening fungal infection. While rhinocerebral forms are well-documented, oral cavity involvement remains underreported and misdiagnosed, despite its potential for rapid progression and serious complications.
Aim:
This systematic review aimed to evaluate and synthesize available evidence on the clinical presentation, anatomical patterns, diagnostic methods, outcomes, and management strategies associated with oral cavity involvement in mucormycosis.
Methodology:
Literature search was conducted across PubMed, Scopus, Embase, Web of Science, and Google Scholar up to 2025. Eligible human studies were included. Data were extracted and narratively synthesized. Quality assessment was conducted using the Newcastle-Ottawa Scale, and risk of bias was evaluated with the ROBINS-I tool with 7 included studies.
Results:
Seven studies comprising 451 cases were analyzed. Most patients were middle-aged males with diabetes and a recent post-COVID-19 status. Common clinical features included palatal ulcers, eschar, tooth mobility, and necrotic lesions. Diagnosis relied on potassium hydroxide mount, histopathology, and imaging. Amphotericin B was the mainstay of antifungal therapy, often combined with surgical debridement or maxillectomy. Mortality varied widely across studies, with better outcomes linked to early diagnosis and combined treatment.
Conclusion:
Oral Mucormycosis is a critical yet often underrecognized condition. Timely identification in high-risk patients is essential to prevent progression.
Introduction
Mucormycosis, a rare yet aggressive fungal infection caused by fungi of the order Mucorales, has emerged as a significant opportunistic infection affecting immunocompromised individuals. The disease is characterized by angioinvasion, leading to tissue necrosis, thrombosis, and subsequent rapid progression if not promptly diagnosed and treated.1,2 Clinicians have documented rhinocerebral mucormycosis most frequently, but involvement of the oral cavity (though less common) is important since it spreads quickly and can cause serious maxillofacial problems.3-5 The pathogenesis of mucormycosis in the oral region typically begins with fungal spore inoculation in susceptible tissue, often following dental procedures (extractions), trauma, or in the presence of underlying conditions such as uncontrolled diabetes mellitus (DM), hematologic malignancies, or immunosuppressive therapy.6-10 The maxilla and palate are commonly affected owing to their rich vascular supply and anatomical continuity with the paranasal sinuses, which facilitates fungal spread. Clinical manifestations in the oral cavity range from palatal eschar, gingival necrosis, exposed bone, tooth mobility, and maxillary or mandibular osteomyelitis.3,5,8,11 In several cases, initial presentation in the oral cavity has preceded or masked deeper rhino-orbital or cerebral involvement.12-14
The involvement of the jaws is highly recognized as a potential nidus for mucormycosis, especially in patients with poorly controlled glycemic status or those undergoing immunosuppressive therapy.8,15,16 Reports suggest that routine dental procedures can trigger fulminant mucormycotic infections, signifying the importance of high clinical recognition in high-risk individuals.17,18 Mandibular involvement, although rare due to its limited vascular supply compared to the maxilla, has been documented in various case reports.3,17,19 Previous studies have emphasized the polymorphic presentation of oral mucormycosis, where early symptoms such as nonhealing ulcers, foul odor, tooth loosening, or unexplained oral pain are often misdiagnosed as common odontogenic infections.14,20,21 These diagnostic delays contribute to disease progression, increased morbidity, and even mortality. Radiological imaging, particularly computed tomography (CT) and MRI, plays a vital role in delineating the extent of bony involvement, but histopathological confirmation remains the gold standard.1,2,22 Several studies and reviews have underscored the clinical complexity and diagnostic challenges associated with oral cavity Mucormycosis.4,5,23,24 While numerous isolated case reports and small series highlight the variability in presentation, treatment, and prognosis, a comprehensive synthesis of oral mucormycosis data specifically targeting its manifestations, management strategies, and outcomes in the oral cavity remains lacking. Moreover, most existing systematic reviews or epidemiological data focus broadly on rhinocerebral forms or COVID-19-associated mucormycosis, with limited emphasis on oral manifestations outside the pandemic context.3-5,23,25,26
Despite numerous individual case reports and small-scale studies, the literature lacks a focused and comprehensive systematic review dedicated to analyzing the oral cavity involvement in mucormycosis across diverse patient populations. The rationale for this systematic review is to bridge this gap by synthesizing existing evidence, identifying clinical patterns, and highlighting diagnostic and therapeutic challenges in oral mucormycosis. The aim of the present systematic review was to critically evaluate and consolidate the literature pertaining specifically to oral cavity involvement in mucormycosis, with emphasis on clinical features, anatomical patterns, diagnostic methods, outcomes, and management strategies.
Methodology
Research Question and PICOS Framework
This systematic review was conducted to investigate the clinical features, anatomical sites, diagnostic approaches, management strategies, and outcomes associated with oral cavity involvement in mucormycosis. It was registered with the International Prospective Register of Systematic Reviews (PROSPERO) with PROSPERO ID 1035958. The review was done according to the PRISMA guidelines. The PICOS (Population, Intervention, Comparison, Outcome, Study design) framework guided the formulation of the research question. The population (P) included patients of all age groups diagnosed with mucormycosis affecting the oral cavity. The intervention (I) considered various diagnostic modalities and treatment strategies, including surgical, pharmacological, or combined approaches. The comparison (C) was not directly applicable, although indirect comparisons between treatment approaches were considered where available. The outcomes (O) of interest encompassed clinical features, anatomical involvement, diagnostic methods, treatment outcomes, morbidity, and mortality. The study design (S) included retrospective and cross-sectional studies.
Search Strategy
A comprehensive literature search was performed across multiple electronic databases, including PubMed/MEDLINE, Scopus, Embase, Web of Science, and Google Scholar. In addition, manual searching of reference lists from relevant articles and gray literature sources was carried out to ensure inclusion of all pertinent studies. The search strategy involved the use of both controlled vocabulary (MeSH terms) and free-text keywords, systematically combined using Boolean operators. The keywords used included: “mucormycosis” OR “zygomycosis”; “oral cavity” OR “mouth” OR “palate” OR “gingiva” OR “maxilla” OR “mandible” OR “jaw”; and specific terms such as “oral mucormycosis,” “palatal mucormycosis,” and “gingival necrosis.” These terms were combined using Boolean operators such as AND, OR, and NOT to refine and expand the search as necessary. Although no language restrictions were applied during the initial search, only articles published in English were considered during the final screening phase. The search was limited to studies published up to 2025.
Eligibility and Selection Criteria
Studies were included if they reported clinical involvement of the oral cavity in confirmed cases of mucormycosis, involved human subjects, and were designed as case reports, case series, observational studies, or original research articles. Out of a total of 624 articles, only 7 were included in the present review after thorough screening according to the PRISMA flowchart (Figure 1). Eligible studies had to provide specific details regarding anatomical location, diagnostic methods, management, or outcomes. Exclusion criteria comprised reviews, editorials, letters, conference abstracts without patient data, experimental animal or in vitro studies, and studies addressing only rhinocerebral mucormycosis without clear mention of oral involvement. Two independent reviewers screened titles and abstracts for relevance, followed by full-text evaluation. Disagreements were resolved through consensus or consultation with a third reviewer.

PRISMA flowchart for the review.
Data Extraction, Synthesis, and Quality/Risk of Bias Assessment
Data extraction was performed using a standardized data extraction form. Narrative synthesis was adopted due to heterogeneity in study design and outcome reporting. Study quality was assessed using the Newcastle-Ottawa Scale (NOS) for cross-sectional studies. 27 Risk of bias was evaluated using the ROBINS-I tool. 28
Results
Table 1 summarizes 7 studies (n = 451 cases) examining oral cavity involvement in mucormycosis, predominantly from India, with additional data from Mexico, Nepal, and Egypt. The average patient age ranged from 38 to 59.7 years, with a male predominance (71%-80%). DM (up to 100%) and post-COVID-19 status were common predisposing factors, along with corticosteroid and oxygen therapy use.22,23,25,26,29 The palate was the most frequently affected site (seen in up to 100%). 30 This is followed by the alveolus, gingiva, tongue, and buccal mucosa. Clinical presentations included palatal ulcers, eschar, tooth mobility (up to 49%), pain, fistula, and necrotic lesions. 26 Radiographic signs and palatal perforation were also notable. 22 The findings highlight the need for early oral screening in at-risk patients.
Summary of Included Studies on Oral Cavity Involvement in Mucormycosis.

Abbreviations: CKD, chronic kidney disease; CLD, chronic liver disease; DM, diabetes mellitus; HbA1c, glycated hemoglobin; HIV/AIDS, human immunodeficiency virus/acquired immunodeficiency syndrome; IHD, ischemic heart disease; IV, intravenous; ROCM, rhino-orbito-cerebral mucormycosis; SD, standard deviation; TMJ, temporomandibular joint.
Table 2 compiles diagnostic approaches, treatments, and outcomes of 451 oral mucormycosis cases across 7 studies. Diagnosis was commonly established through KOH (potassium hydroxide) mount, fungal culture, histopathology, and imaging (CT/MRI).25,26,29,22 Time to diagnosis ranged from 8 to 45 days post-COVID-19, averaging 10.5 days in one study. 24 Amphotericin B (liposomal/conventional) was the primary antifungal used, sometimes with Posaconazole.24,29 Surgical management ranged from conservative debridement to total maxillectomy.23,30 Outcomes varied: mortality was highest in Bonifaz et al (74.6%), 37 while Ghalwash et al reported a 49% mortality. 30 Recurrence was linked to incomplete debridement or endoscopic-only procedures. 23 Complications included cerebral extension, mucocutaneous involvement, and cavernous sinus invasion.22,29,30 Early diagnosis and combined surgical-medical therapy were critical to improving prognosis.
Diagnostic Methods, Management, and Outcomes of Oral Mucormycosis Cases.

Abbreviations: CECT, contrast-enhanced computed tomography; CNS, central nervous system; CT, computed tomography; FESS, functional endoscopic sinus surgery; ICA, internal carotid artery; ICMR, Indian Council of Medical Research; ITS-PCR, internal transcribed spacer-polymerase chain reaction; KOH, potassium hydroxide; MRI, magnetic resonance imaging; PNS, paranasal sinuses; STIR, short tau inversion recovery.
Figure 2 illustrates the distribution of mucormycosis involvement across various oral sites. The palate is the most affected site, accounting for 58% of cases, followed by the alveolus (20%). Other less frequent sites include the gingiva (5%), tongue (3%), and buccal mucosa (2%). Twelve percentage of cases presented with involvement of combined oral sites. These findings signify the palate as the primary site of infection, mostly due to its proximity to the maxillary sinus and vascular network. Early recognition of palatal lesions is crucial for timely diagnosis and intervention in oral mucormycosis.

Pie chart representing the site of mucormycosis.
Figure 3 illustrates the number of mucormycosis cases that resulted in recovery or death across 5 studies. The highest recovery rate was reported by Bhavana et al 23 with 47 patients recovering and only 6 deaths, suggesting effective management or early diagnosis. Sachan et al 29 also showed a favorable outcome with 42 recoveries and 10 deaths. In contrast, Bonifaz et al 24 reported a significantly higher number of deaths (41) compared to recoveries (14), indicating potentially advanced disease stages or delayed intervention. Paudel et al 22 demonstrated the best survival profile with 20 recoveries and only 1 death. Ghalwash et al reported nearly equal outcomes, 26 recoveries and 25 deaths, indicating a more variable prognosis. 30 These variations highlight the importance of early diagnosis and intervention in mucormycosis outcomes.
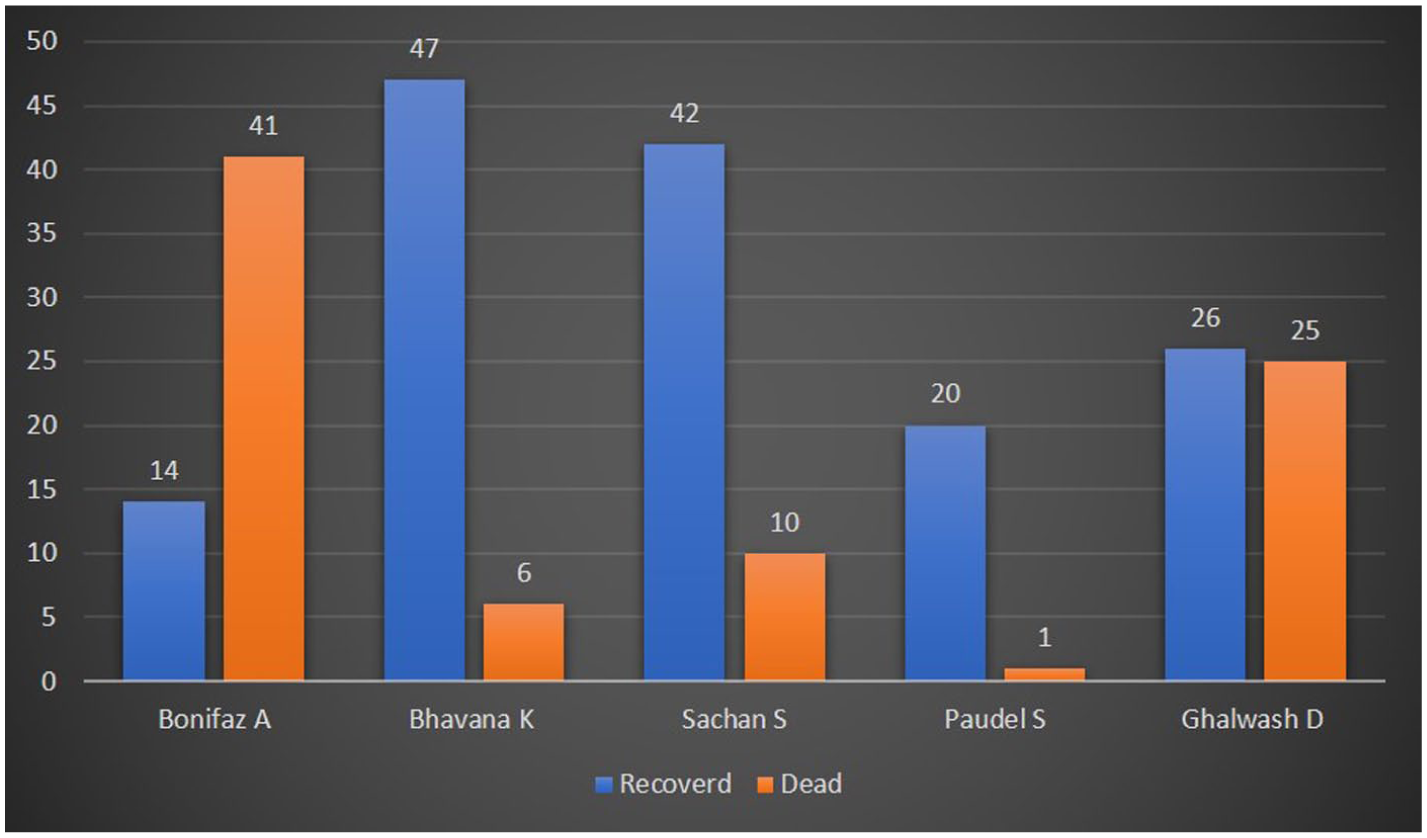
Graph representing the number of cases recovered and dead due to mucormycosis.
Table 3 presents the quality assessment of included cross-sectional studies using the NOS, scored out of 10 based on Selection (5★), Comparability (2★), and Outcome/Exposure (3★). Three studies like Bhavana et al, 23 Sachan et al, 29 and Ghalwash et al, 30 achieved high-quality ratings with total scores of 9/10, 9/10, and 10/10, respectively, reflecting strong methodology, good sample selection, and robust outcome reporting. The remaining 4 studies, including Bonifaz et al, 24 Chandwani et al, 25 Somkuwar et al, 26 and Paudel et al, 22 scored 7/10, categorized as moderate quality. Overall, the assessment indicates that most studies had appropriate comparability (★2) and outcome reporting, though selection criteria varied slightly across studies.
Quality Assessment for Cross-Sectional Studies (Newcastle-Ottawa Scale).

Figure 4a illustrates the risk of bias assessment for included studies using the ROBINS-I tool across 7 domains. Most studies demonstrated a low risk of bias in most domains (green), indicating sound methodological quality. Bhavana et al, 23 Somkuwar et al, 26 and Sachan et al 29 had predominantly low-risk scores across domains, affirming strong study validity. Bonifaz et al 24 and Ghalwash et al 30 showed moderate bias in confounding and classification of interventions (yellow), with Bonifaz et al 24 also lacking information (blue) on participant selection and missing data. Paudel et al 22 had moderate bias in multiple domains but maintained an overall low-risk judgment. Overall, all studies were acceptable, with minimal serious risk observed.

(a) Individual studies’ risk of bias assessment using the ROBINS-I tool. (b) Overall risk of bias assessment using the ROBINS-I tool.
Figure 4b represents the cumulative risk of bias across studies using the ROBINS-I tool. Most domains exhibited a low risk (green), indicating robust methodology. Bias due to confounding and deviations from intended interventions showed 100% low-risk judgments. However, moderate risk (yellow) was notable in domains like selection of participants, classification of interventions, and reporting bias, each affecting ~25% to 30% of studies. Moreover, lack of information (blue) was a concern in ~30% to 35% of studies for classification and missing data domains. These findings suggest that although overall study quality is acceptable, gaps in reporting and participant selection processes may limit interpretability and generalizability. Cross-verification with individual studies (Figure 3) confirms these patterns, especially for Bonifaz et al 24 and Ghalwash et al. 30
Discussion
This systematic review synthesizes evidence from 7 clinical studies, including 451 patients, to demonstrate the epidemiological, clinical, diagnostic, and therapeutic features of oral mucormycosis. Oral mucormycosis, an aggressive opportunistic infection caused by Mucorales fungi, presents with angioinvasion and necrosis, with oral manifestations increasingly recognized as a significant subset, especially post-COVID-19. The present review revealed that the palate was the most frequently involved anatomical site (~58%), followed by the alveolus (20%), gingiva, tongue, and buccal mucosa.3,8,30 The high susceptibility of the palatal region is attributed to its dense vascular network and anatomical proximity to paranasal sinuses, thus leading to fungal angioinvasion and necrosis.5,8 Similar cases were observed in various geographic cohorts from different countries like India, Egypt, Nepal, and Mexico.22,26,30 Palatal involvement as an early sign has also been shown in previous cases, with some presenting as indurated ulcers, leading to delayed diagnosis.31-33 Clinical presentations ranged from palatal ulcers, eschar formation, and tooth mobility (up to 49% in some cohorts), to full-thickness necrosis, oroantral fistulae, and facial pain.5,12,20,21 The polymorphic appearance of oral mucormycosis often mimicking chronic osteomyelitis, periodontal disease, or odontogenic abscesses leads to frequent misdiagnosis or delayed recognition.14,20,21 It has been noted that mucormycosis is most common in the maxilla, although mandibular involvement has also been documented, particularly after dental extractions or trauma, despite its relatively poorer vascular supply.3,17,19 Previous cases have shown primary gingival involvement or orbital extension secondary to periodontal foci, thus depicting a broader clinical spectrum.34-36 DM is considered the chief comorbidity in most of the included studies, primarily among Indian cohorts.23,25,26 This can be explained based on the disease mechanisms whereby hyperglycemia, ketoacidosis, and iron overload impair the neutrophil function, thus facilitating fungal growth.6,7,9
According to Mora-Martínez et al, 37 oral mucormycosis commonly presented with palatal necrosis and tooth mobility and was often misdiagnosed as a dental infection. The authors reiterated that early recognition and combined surgical-antifungal therapy were critical to reduce high mortality in this aggressive, angioinvasive fungal disease. The present review highlights emerging antifungal strategies targeting biofilms, including the use of novel agents and combination therapies, which hold promise in overcoming current therapeutic limitations in oral mucormycosis management.
The present review findings corroborate previous evidence, which explains how poorly controlled diabetes, along with COVID-19 and corticosteroid therapy, significantly increases the risk for Mucormycosis.25,26,29,30 The present review also highlights the post-COVID-19 state as a potent predisposing factor, largely due to immune dysregulation, steroid use, and prolonged oxygen therapy.24,35,30 Certain co-infections like actinomycosis and oral candidiasis have also been noted in post-COVID conditions that complicate the clinical presentations.38,39 In some cases, oral cavity involvement was the only presentation, thus signifying the necessity for immediate intervention as a primary clinical entity rather than only a rhinocerebral extension.12,21 Even immunocompetent individuals developed mucormycosis following dental trauma or extractions, indicating that local breaches in mucosal or bony barriers can initiate infection. There have been reports of recurrences after primary surgical clearance, indicating the need for extended follow-up and antifungal therapy.8,16,40,41 Oral mucormycosis presents with diverse, often certain undiagnosed clinical features, especially in diabetic or post-COVID-19 patients. 37 Thus, timely identification depends upon the incorporation of histopathology, imaging, and microbiology and multidisciplinary care. The combination of early surgical debridement with systemic antifungals is essential to control the progression and reduce the mortality rate. Similar findings have been obtained in the present review, which demonstrates that integrating microbiological, histopathological, and radiological diagnostics facilitates timely and accurate identification of the infection. Thus, these studies have enhanced our understanding of mucormycosis pathogenesis and strengthened the significance of adopting multidisciplinary treatment protocols which integrates early surgical intervention with systemic antifungal therapy. Hence, implementing such comprehensive approaches will be crucial in improving patient outcomes and reducing mortality associated with oral mucormycosis.
Diagnostic Modalities and Challenges
Diagnosis of mucormycosis is primarily established through KOH mount, histopathological examination, and imaging (CT/MRI).22,25,26,29 Histopathological analysis reveals hallmark features of broad, non-septate hyphae with right-angle branching, confirming Mucorales infection.1,2 Imaging is essential for delineating the extent of sinus or bone involvement, particularly when surgical intervention is considered. 22 However, the average time between COVID-19 recovery and mucormycosis diagnosis is around 8 to 45 days, with a mean of 10.5 days, therefore emphasizing the need for early diagnosis and prompt intervention.20,42 Diagnostic delays are a key determinant of poor prognosis. A study done by Bonifaz et al reported a 74.6% mortality rate, which demonstrated the consequences of late-stage presentation and missed diagnostic opportunities. 24 A recent cross-sectional study by Zakaria et al emphasized the critical diagnostic window of 2 weeks post-COVID for initiating antifungal surveillance in high-risk individuals. 42
The success of the treatment largely depended on how early and aggressively it was started. The main drug used was liposomal amphotericin B, often followed or supported by Posaconazole or Isavuconazole.22,23,24,29 Surgical strategies varied from conservative curettage to total or partial maxillectomy, depending on disease spread.23,30 Evidence supports that aggressive multimodal treatment combining radical surgical debridement with systemic antifungal therapy yields the most favorable outcomes.22,23,30 In contrast, incomplete or minimally invasive approaches, especially endoscopic-only surgeries, were associated with relapse and persistent infection. 30 Ramadorai et al demonstrated improved survival with a staged surgical approach and tailored amphotericin dosing based on radiological staging. 43 Mortality varied widely across studies, ranging from 20% to over 70%, influenced by factors such as diagnostic delays, comorbidities, and adequacy of surgical excision.23,24,26,30 For example, Bhavana et al attributed improved survival rates to early diagnosis and a structured classification-based treatment protocol. 23
Methodological Strengths, Limitations, and Clinical Implications
The included studies demonstrated moderate to high methodological quality, with NOS scores ranging from 7 to 10 out of 10, confirming the reliability of chief clinical and therapeutic findings despite certain drawbacks.23,29,30 Retrospective study designs, variability in treatment protocols, incomplete follow-up data, and a potential publication bias that may have affected the outcomes toward more severe or fatal presentations are some of the limitations identified.24-26 Clinically, the evidence supports routine oral examination, especially of the palate in diabetic, immunocompromised, or post-COVID-19 patients, with prompt initiation of histopathological and radiographic evaluation for any nonhealing oral lesions. It has been noted that early and aggressive surgery, especially open debridement, along with systemic antifungal treatment using Amphotericin B followed by Posaconazole, significantly improves survival. Advances in understanding the disease process, such as its iron uptake, blood vessel invasion, and interaction with the host, have facilitated the treatment approach.31,32 Hence, it is imperative to educate diabetic patients, especially those undergoing dental treatments, to reduce the risk of infection. However, future research should focus on prospective studies that monitor blood glucose level, steroid, or oxygen use, along with recent dental procedures. Comparing open and endoscopic surgeries, reporting outcomes such as 30- and 90-day death rates, recurrence, and recovery, will further help in guiding the treatment protocol. Studies on new antifungal drugs, such as Isavuconazole, are also needed to improve care for this serious and often deadly fungal infection.
Conclusion
Thus, this review affirms oral mucormycosis chiefly as a distinct and severe manifestation of invasive fungal infection primarily affecting the palatal mucosa. The syndemic interaction of COVID-19, diabetes, and dental procedures increases its susceptibility. Early clinical identification, rapid diagnostic confirmation, and a multidisciplinary, aggressive treatment strategy are essential to reduce the mortality rate. Despite current evidence demonstrating considerable progress, standardized multicenter studies are needed to refine diagnosis, optimize interventions, and improve patient outcomes in this life-threatening condition.
Footnotes
ORCID iDs
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.