
Abstract

Significance Statement
Chorda tympani schwannomas (CTSs) are rare tumors that typically present with hearing loss. This report highlights an even rarer presentation: an asymptomatic patient with normal hearing. It emphasizes the crucial role of imaging—particularly contrast-enhanced MRI and diffusion-weighted imaging—in differentiating CTS from congenital cholesteatoma. This distinction allows for a confident presumptive diagnosis and supports a conservative “wait-and-scan” approach, which avoids unnecessary surgical intervention and the risk of iatrogenic taste disturbance in asymptomatic individuals.
Case Presentation
A 42-year-old asymptomatic woman was referred to our department for evaluation of a left retrotympanic mass (Figure 1). Otoscopic examination revealed a whitish mass located primarily behind the posterosuperior quadrant of the tympanic membrane. The mass caused bulging of the overlying tympanic membrane and extended slightly to involve the posterior wall of the external auditory canal without evidence of bony erosion. No middle ear effusion was present. Pure-tone audiometry showed normal hearing bilaterally. Examination of the right ear was unremarkable.

Endoscopic view of the left ear. A whitish, retrotympanic mass (arrow) is visible in the posterosuperior quadrant, causing slight bulging of the intact tympanic membrane.
Temporal bone computed tomography (CT) revealed a 3-mm mass at the tympanic orifice of the posterior canaliculus (Figure 2). The ossicular chain was intact, and there was no evidence of facial canal dilation. On magnetic resonance imaging (MRI), the mass demonstrated low signal intensity on T1-weighted images and showed enhancement following gadolinium administration (Figure 3). The mass showed no restricted diffusion on diffusion-weighted imaging (DWI).
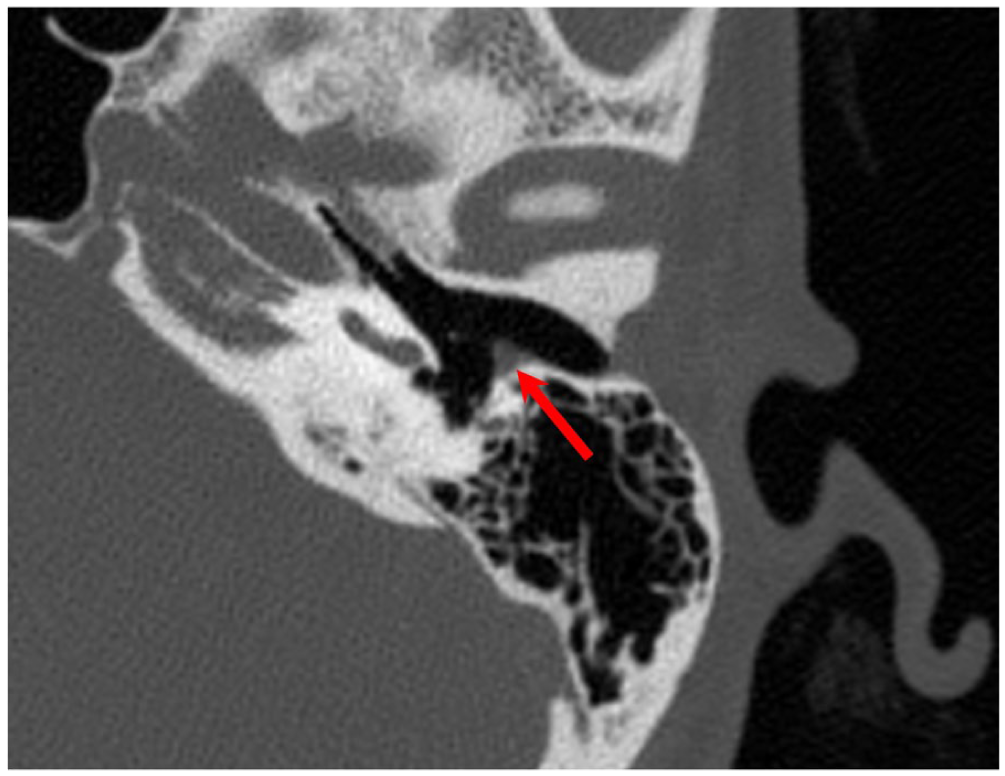
Axial temporal bone computed tomography scan. A small, well-defined soft-tissue mass (arrow) measuring approximately 3 mm is identified at the tympanic orifice of the posterior canaliculus for the chorda tympani nerve.
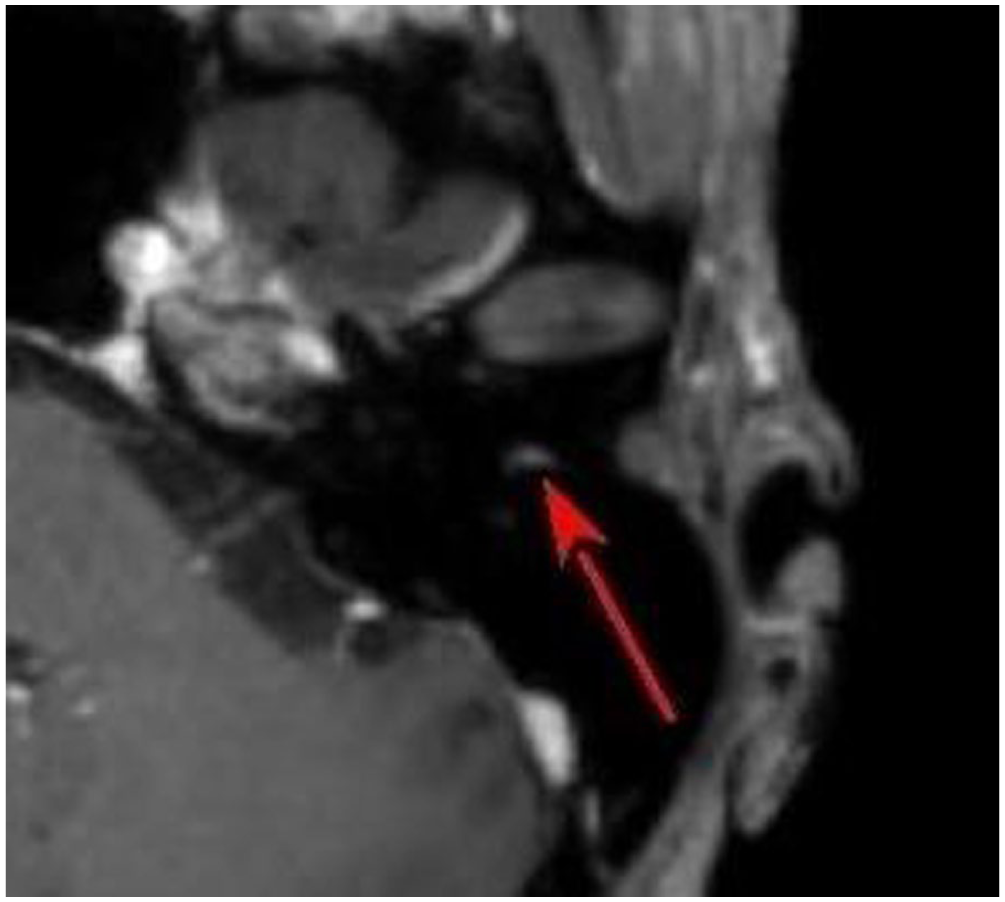
Axial post-contrast T1-weighted magnetic resonance imaging. The lesion (arrow) demonstrates enhancement following gadolinium administration, a characteristic finding for a schwannoma.
Based on these findings, a presumptive diagnosis of a chorda tympani schwannoma (CTS) was made. Congenital cholesteatoma, the primary differential diagnosis, was considered less likely as the lesion demonstrated contrast enhancement and showed no restricted diffusion on DWI. A glomus tympanicum tumor, another differential diagnosis, was also considered unlikely. This was because the mass appeared whitish rather than reddish—a finding characteristic of a highly vascular tumor—and was non-pulsatile.
Histopathological confirmation was considered but deferred, given that the patient was asymptomatic and the potential risk of iatrogenic taste dysfunction from an invasive biopsy. Therefore, conservative management with regular imaging follow-up was recommended.
Discussion
CTS is an exceedingly rare benign tumor, and its clinical presentation can vary, making preoperative diagnosis challenging. 1 Otoscopically, CTS typically appears as a pale, whitish, or pinkish mass behind an intact tympanic membrane, often in the posterosuperior quadrant.2,3 This appearance can mimic that of a congenital cholesteatoma, a more common middle ear mass. While the most frequently reported symptoms of CTS are conductive hearing loss and tinnitus,1,4,5 our patient was asymptomatic, which represents a rare clinical presentation. 6 Preoperative taste disturbance is notably absent in nearly all reported cases. It is speculated that the tumor’s slow growth allows for neural compensation. 7 However, a limitation of this report is the absence of objective gustatory function tests, such as electrogustometry. As the patient reported no subjective taste disturbance, more detailed testing was not performed in the initial assessment. It is therefore possible that the tumor’s slow compression caused a gradual, compensated decline in taste function that went unnoticed by the patient. In this context, the term “asymptomatic” refers to the patient’s subjective perception and does not exclude the possibility of pre-existing functional decline on the affected side.
Radiological assessment is paramount for differentiating CTS from other middle ear lesions. A high-resolution CT scan typically reveals a well-defined soft-tissue mass, which may or may not be associated with bony erosion.4,8 One subtle but potentially useful sign is the enlargement of the petrotympanic fissure on sagittal CT views. 1 However, MRI is the most valuable imaging modality for diagnosis. CTS characteristically demonstrates avid enhancement with gadolinium, a key feature that distinguishes it from a non-enhancing congenital cholesteatoma. 1 Furthermore, the absence of restricted diffusion on DWI, as seen in our patient, strongly argues against a diagnosis of cholesteatoma. 1
The management of CTS depends on the patient’s symptoms, hearing status, and tumor size. While surgical resection is the definitive treatment for symptomatic or growing lesions,4,9 a conservative “wait-and-scan” approach may be a valid option for small, asymptomatic tumors such as the one in our patient. This strategy avoids the primary morbidity of surgery: iatrogenic taste disturbance resulting from the sacrifice of the chorda tympani nerve.
Taste disturbance after middle ear surgery is not a rare complication, reported in 42.7% of patients at 10 days postoperatively. 10 The risk becomes more significant when a “healthy” chorda tympani nerve (CTN), not involved in inflammation as in our case, is subjected to surgery. According to a prospective cohort study by Lafargue et al, when a healthy CTN was transected, taste disorders occurred at a high frequency of 73.3% at 10 days postoperatively, and this incidence remained significantly higher compared to other types of nerve injury (stretching or preservation) for up to 1 year. 10 As a schwannoma originates from the nerve sheath itself, preserving the nerve during complete tumor excision is exceptionally difficult Furthermore, persistent taste disorders have been shown to impact a patient’s quality of life. 11 Thus, the substantial risk of iatrogenically inducing a permanent and high-impact taste disturbance in a subjectively asymptomatic patient provided a rationale for our conservative “wait-and-scan” approach. It is recommended that all patients be counseled preoperatively about the potential for postoperative dysgeusia. 9 Given that our patient was asymptomatic, observation with serial imaging allows for monitoring of tumor growth while preserving gustatory function.
Footnotes
Ethical Considerations
Ethical approval to report this case was obtained from the Clinical Research Ethics Review Committee of Mie University Hospital (H2021-114).
Consent for Publication
Written informed consent was obtained from the patient for publication.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, HS, upon reasonable request.