
Abstract
Objective:
This study compares complications between drainless parotidectomies versus parotidectomies where drains were inserted post-operatively.
Data Sources:
PubMed, MEDLINE, Embase, Cochrane Database of Systematic Reviews, and Web of Science databases.
Review Methods:
This systematic review and meta-analysis compared outcomes of parotidectomy with and without intraoperative drain insertion. A comprehensive database search was conducted in accordance with PRISMA reporting guidelines, yielding 186 articles, of which 21 met the inclusion criteria. Studies were assessed for risk of bias using the Newcastle–Ottawa Scale for non-randomized studies and the Cochrane Risk of Bias 2.0 tool for randomized controlled trials. Post-operative complication rates – including hematoma, seroma, and sialocele formation – were extracted and analyzed.
Results:
The database search yielded 284 citations, of which 98 citations were omitted due to duplication. Of the remaining 186 citations, 142 were omitted during title/abstract screening, and the remaining 43 underwent full-text screening, of which 22 were excluded, resulting in 21 studies included in the systematic review and 5 being included in quantitative analysis. Across included studies, 3138 individuals underwent parotidectomy (2263 with drains and 875 without). No significant differences were found between drain and drainless groups in hematoma (OR = 0.9, CI: 0.14 to 5.7, P = .91) or sialocele/seroma formation (OR = 0.45, CI: 0.17 to 1.18, P = .10). In single-arm studies, hematoma rates were similar (1.03% with drains vs 0.5% without), while sialocele/seroma rates were higher in drainless cases (11.5% vs 6.4%).
Conclusion:
There was no significant difference in complication rates post-operatively between the drain and no drain groups, with an increased length of hospital stay in the drain group, and a trend toward higher seroma rates in the drainless group. Nevertheless, it is feasible to perform outpatient parotidectomy with drains.
Introduction
The customary post-operative care for patients undergoing parotidectomy involves the utilization of a percutaneous drain, owing to the abundant vascular supply and concern of post-operative complications such as the formation of hematoma or seroma. In 2023, Liu et al conducted a survey among members of the Canadian Society of Otolaryngology-Head and Neck Surgery to enquire about their preferences regarding routine use of drains in parotidectomy, where 68% of respondents expressed a preference for routine drain insertion. 1
Over the recent years, there has been a practice shift toward performing head and neck surgeries, such as thyroidectomy, on an outpatient basis. The primary motivators for performing outpatient surgery include improving patient care by minimizing hospital stay and to promote faster recovery at home, increasing the efficiency of healthcare personnel and hospital resources, and reducing overall healthcare costs. 2 Historically, parotidectomies have been performed on an inpatient basis mainly to facilitate overnight drainage of the surgical site. 3 Several retrospective studies have demonstrated that there is no statistically significant difference between drain and drainless parotidectomies in terms of the hospital course, complication rates, or overall surgical outcomes. In addition, drains are associated with significant morbidity due to the associated pain and discomfort, and risk of drain site infection. However, these studies have considerable limitations, mainly in terms of sample size and study design.3 -5
The primary objective of this meta-analysis is to compare post-operative hematoma, seroma, and sialocele rates between routine drain versus drainless parotidectomy in order to provide evidence to guide surgical practice in parotidectomy. Length of hospital stay is examined as a secondary outcome.
Methods
Study Protocol
This systematic review and meta-analysis was based on a pre-specified protocol. The Cochrane Handbook for Systematic Reviews of Interventions was used to design and prepare the current study. The Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement was used as a reporting tool. A librarian from Unity Health Toronto was consulted for guidance in developing the manuscript’s systematic search strategy.
Eligibility Criteria and Study Selection
Studies were eligible for inclusion if they met the following criteria:
(i) Study design: Randomized controlled trials (RCTs), prospective cohort studies, or retrospective cohort studies.
(ii) Population: Adult individuals undergoing parotidectomy for any indication, with documentation of the type of parotidectomy performed, its indication, and any concurrent surgical interventions provided within the manuscript.
(iii) Intervention: Use of intraoperative surgical drains.
(iv) Comparator: Omission of drain placement (drainless parotidectomy).
(v) Outcomes: Reporting of post-operative complications (including hematoma, seroma, or sialocele formation) and/or hospital length of stay.
Studies were excluded if they met any of the following criteria:
(i) Focused on unrelated diagnoses or procedures not involving parotidectomy.
(ii) Involved in vitro or non-clinical analyses.
(iii) Were not primary clinical studies, including case reports, case series, cross-sectional studies, review articles, editorials, or letters.
(iv) Were published in languages other than English, due to feasibility and resource limitations.
Information Sources, Search Strategy, and Study Selection
PubMed, MEDLINE, Embase, Cochrane Database of Systematic Reviews, and Web of Science databases were systematically screened from inception until November 2023. The following subject headings: (“parotidectomy” OR “parotid”) AND (“drainage” OR “drains” OR “suction drain”). To broaden the literature search, we scanned the reference lists of eligible studies and contemporary reviews for potentially missed relevant studies. The study selection process comprised omitting duplicate citations, followed by screening of titles and abstracts for possible inclusion by 2 reviewers independently to identify articles for full-text review. Articles were only included if both reviewers independently determined that all inclusion criteria were met. If consensus was not reached, a third author was consulted.
Quality Assessment of the Included Studies
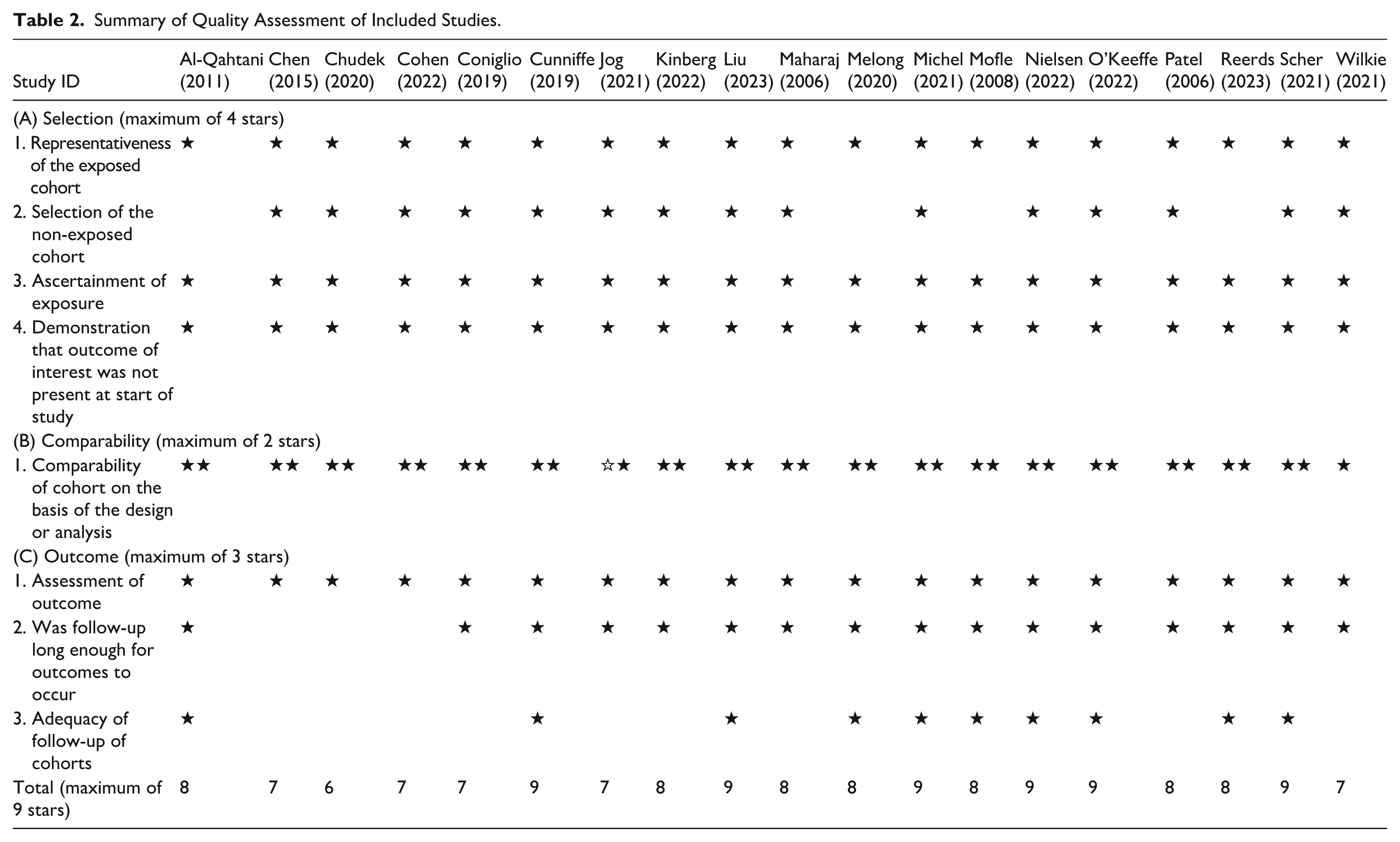
The quality of each study was examined in accordance with the Cochrane risk of bias tool (version 2) for RCTs and Newcastle–Ottawa Scale (NOS) for cohort studies, with each study being assigned a corresponding score across various domains for the overall quality of the study. The NOS score ranges from 0 to 9 stars, with higher scores indicating lower bias. We considered studies with 7 or more stars as good quality, 4 to 6 stars as fair quality, and 3 or less stars as low quality. Two co-authors (S.H. and B.A.) completed the quality assessment, and discrepancies were settled by consultation with the principal investigator.
Data Collection and Study Endpoints
We collected the baseline characteristics of the included studies and participants, such as first author’s name and year of publication (study identifier), study arms, total sample size, age, gender, outpatient versus inpatient, post-operative complications (hematoma, seroma, and sialocele), length of hospital stay, and use of fibrin glue or tissue sealant.
Our endpoints included post-operative complications (hematoma, seroma, and sialocele) and length of hospital stay. Two co-authors (S.H. and B.A.) independently collected data using a predesigned extraction sheet, and discrepancies were settled by consultation with the principal investigator
Statistical Analysis
Data synthesis was conducted using Review Manager 5.4.1 and RStudio Posit PBC (Version 4.2.2) for Microsoft Windows. Two independent authors (S.H. and A.A.) extracted and entered the data into Review Manager. A random-effects model was employed to account for potential heterogeneity, assessed using the I2 statistic. Heterogeneity was considered statistically significant if I2 ≥50% with a P-value <0.1. In cases of significant heterogeneity, a sensitivity analysis was performed to identify potential sources of variability and determine the study contributing to the observed heterogeneity.
For continuous outcomes, the standardized mean difference (SMD) was calculated between the 2 groups. A positive SMD for length of hospital stay would favor the drainless group, a negative SMD would favor the drain group, and a SMD of 0 would favor neither group.
For dichotomous outcomes, the odds ratio (OR) was calculated between the 2 groups. The OR is the odds of an event in the intervention (no drain) group compared with the control (drain) group.
Results
Summary of Literature Search
The database search yielded 284 citations, of which 98 citations were omitted due to duplication. Of the remaining 186 citations, 142 were omitted during title/abstract screening, and the remaining 43 underwent full-text screening, of which 22 were excluded, resulting in 21 studies included in the systematic review. Due to heterogeneity and wide variations in reporting outcomes, only 5 studies were included in the quantitative analysis. Figure 1 summarizes the PRISMA flowchart for literature search and study selection.
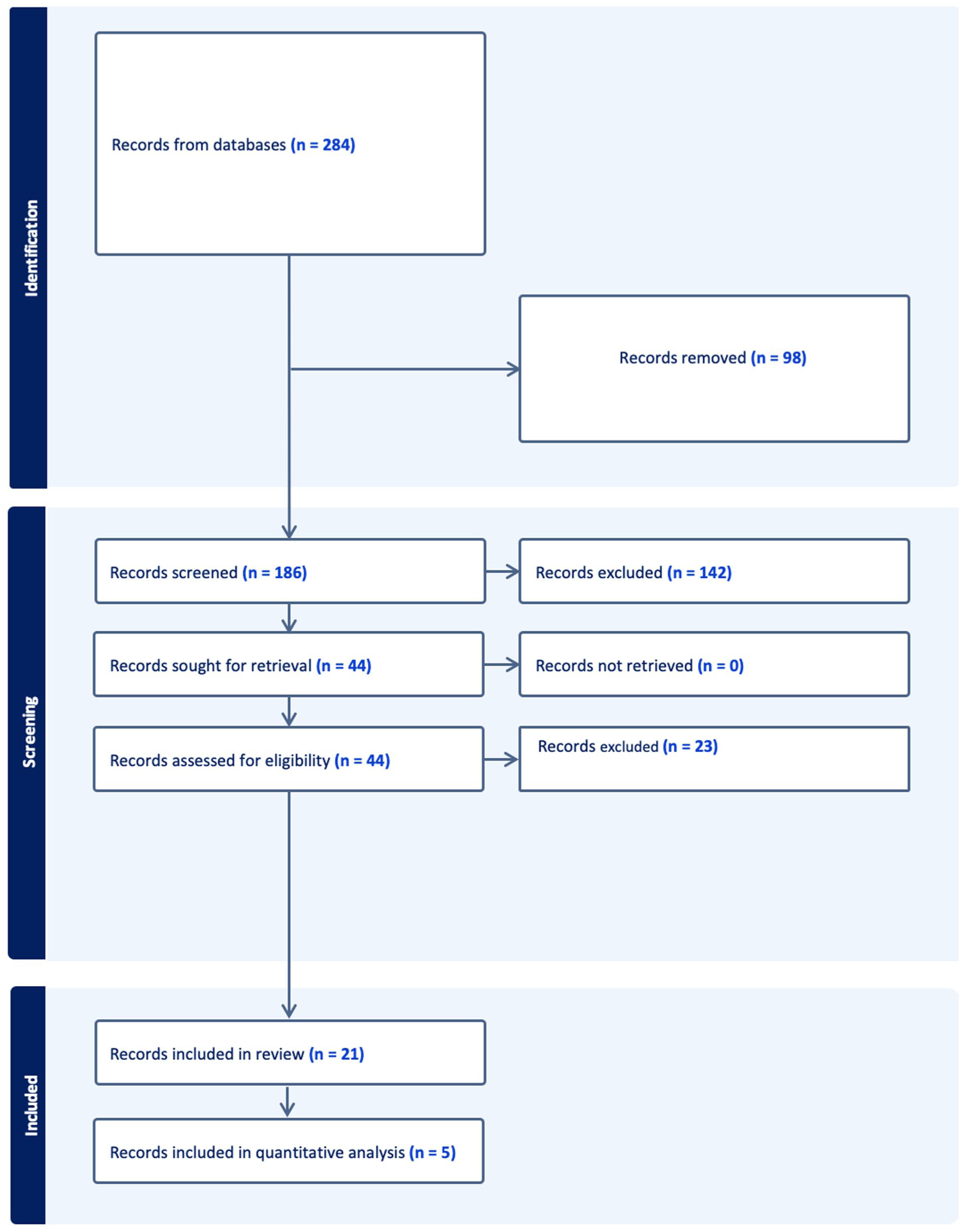
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart for literature search and study selection.
Summary of the Characteristics of the Included Studies and Participants
Overall, 3138 individuals underwent parotidectomy across 21 studies (2263 patients with drain inserted, and 875 with no drain inserted). These studies took place from 2006 to 2023. The research participants were all adult patients. The summary of baseline characteristics of the included studies and participants is depicted in Table 1.
Baseline Characteristics of Included Studies and Participants.
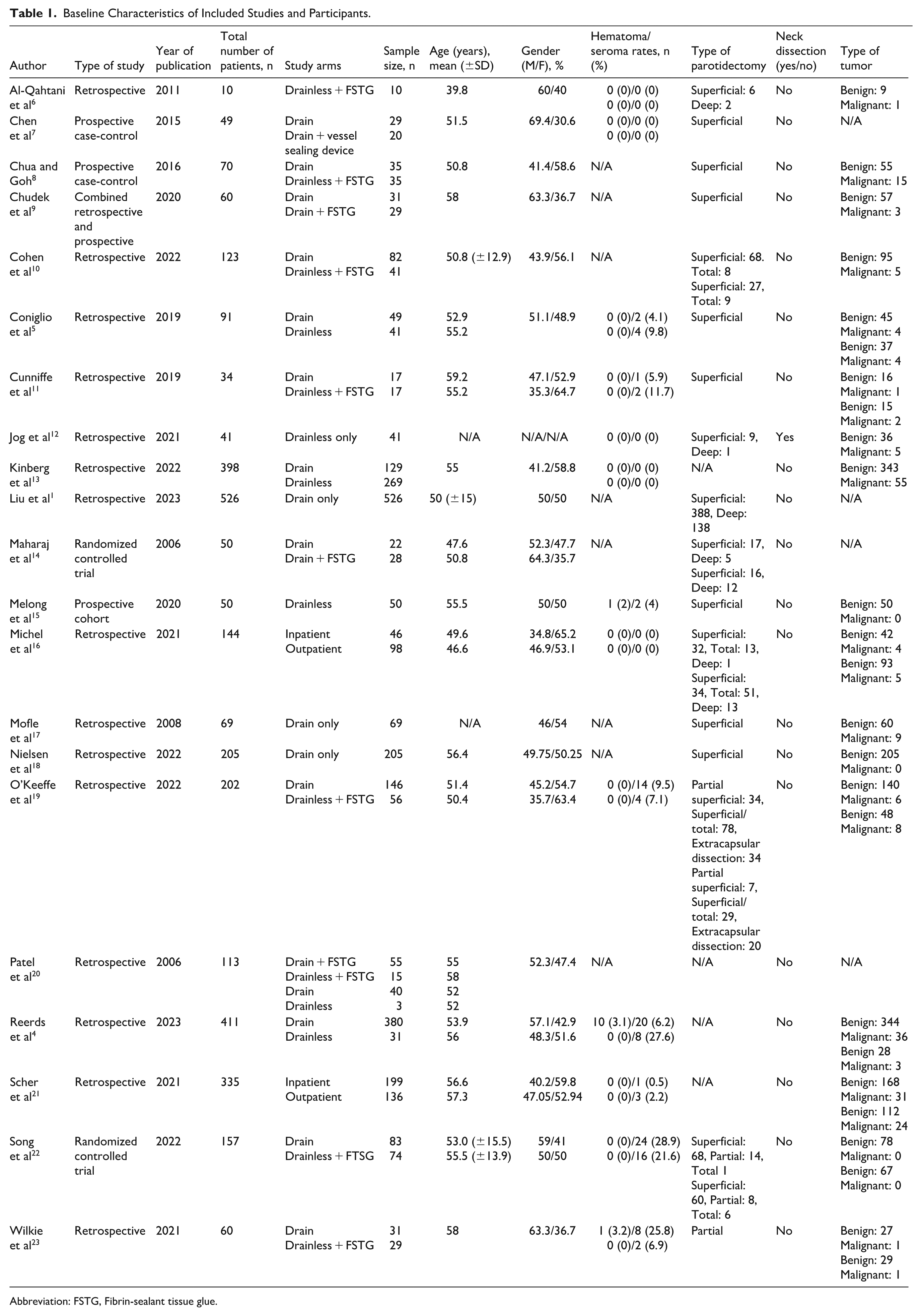
Abbreviation: FSTG, Fibrin-sealant tissue glue.
Summary of the Quality Assessment
The overall quality assessment was good quality in 18 studies, fair quality in 1 study as per the NOS as demonstrated in Table 2, and low risk of bias was identified in 1 RCT and some concern of bias in 1 RCT due to lack of information regarding allocation concealment and some concern of bias in selection of the reported result per the Cochrane risk of bias assessment tool version 2 as demonstrated in Figure 2.
Summary of Quality Assessment of Included Studies.
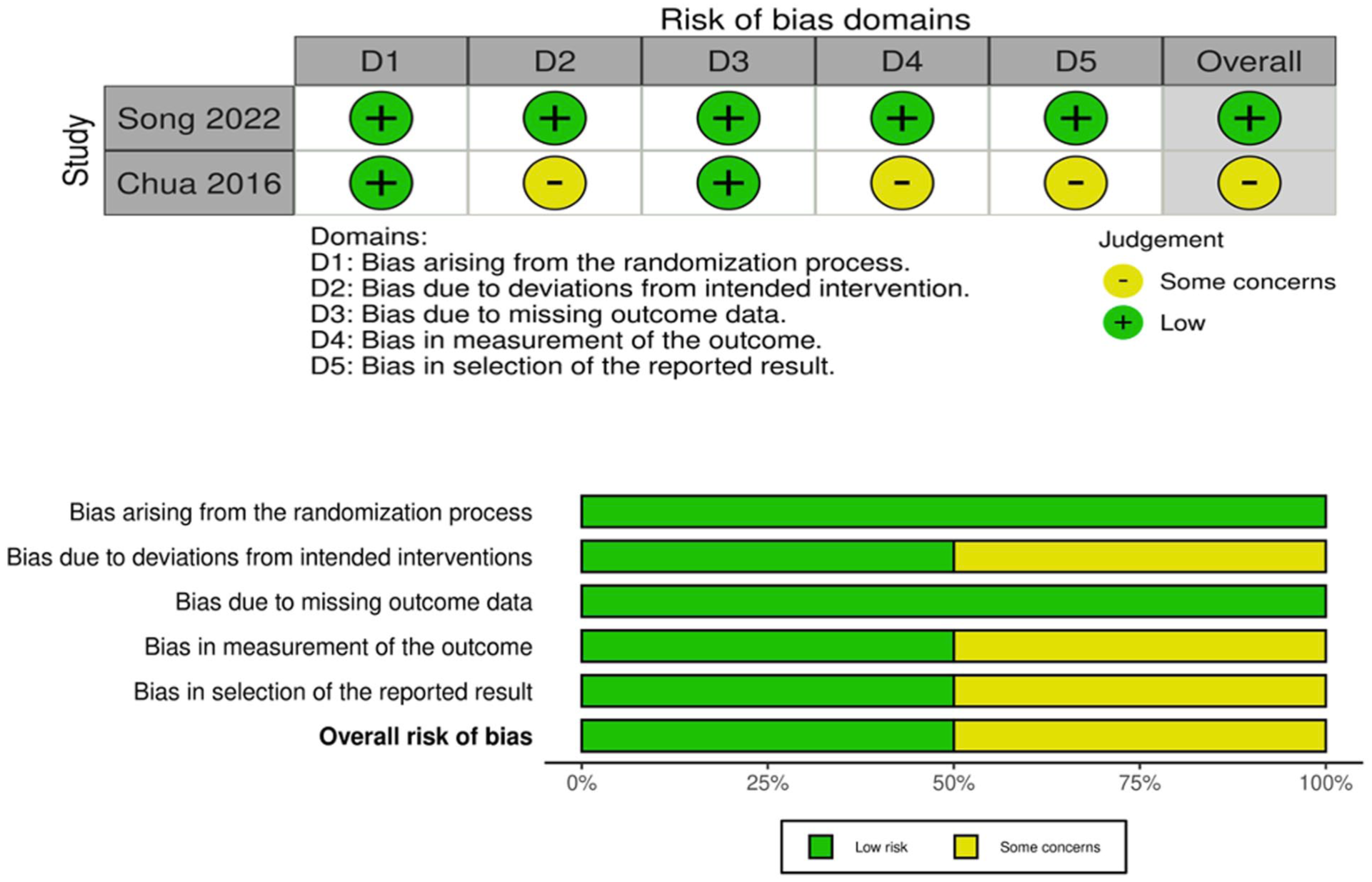
Summary of the quality assessment of the included randomized controlled trials.
Meta-Analysis of Endpoints
Primary Outcomes
Hematoma – Drain Versus No Drain
Rates of hematoma formation comparing patients with and without drains were analyzed based on data from 3 studies involving 555 (drain) and 118 (no drain) patients. The odds ratio analysis for hematoma formation in patients undergoing parotidectomy reveals no statistically significant difference between the 2 groups (OR = 0.9, CI = 0.14 to 5.7, P = .91). The studies showed a low degree of heterogeneity (I2 = 0%, P = 0.46). The meta-analysis findings are summarized and depicted in Figure 3.
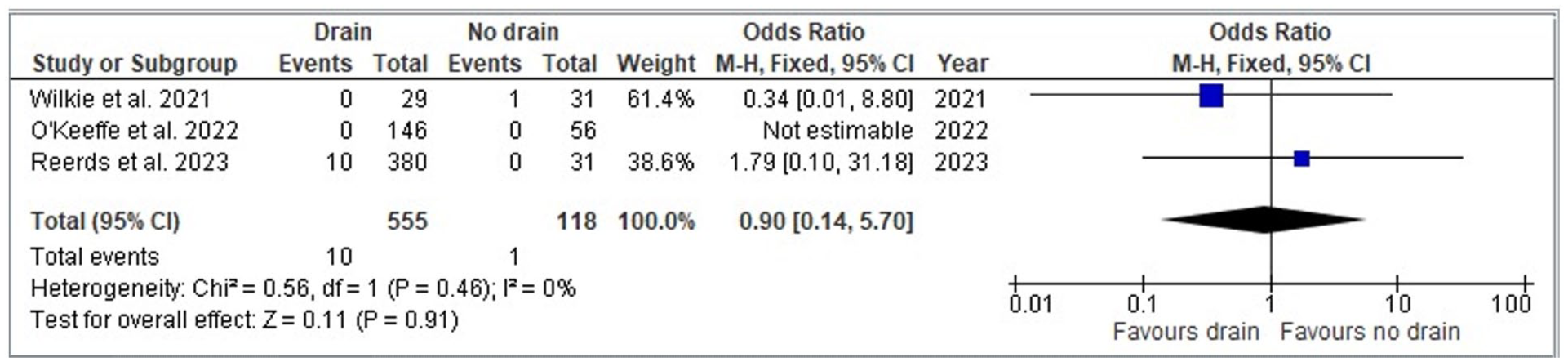
Forest plot for odds ratio analysis between drain versus no drain in parotidectomy patients – hematoma.
Seroma/Sialocele – Drain Versus No Drain
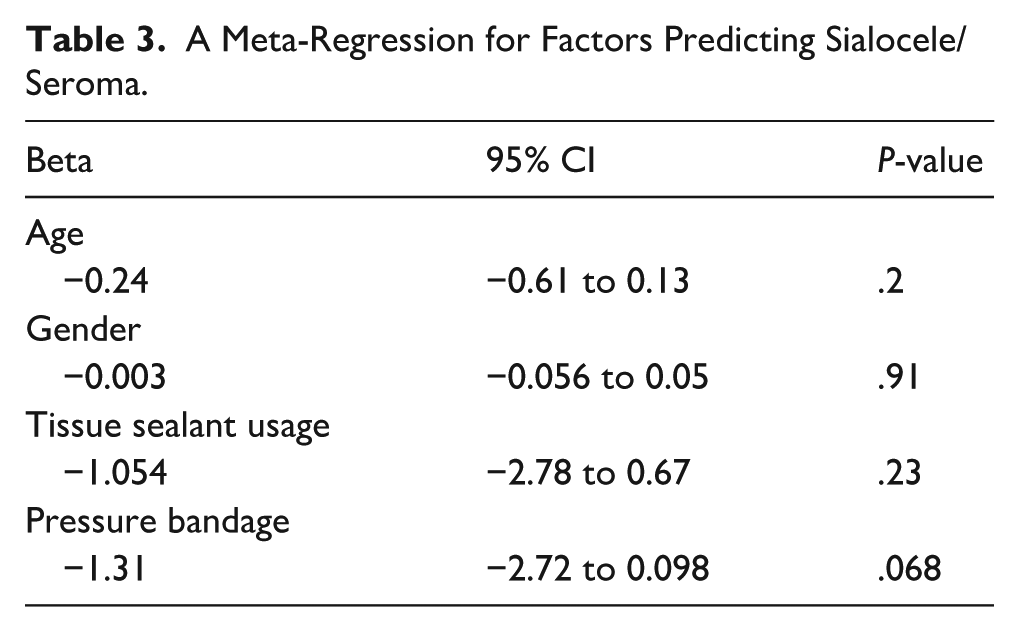
The meta-analysis findings for sialocele/seroma formation comparing patients with and without drains were based on data from 5 studies involving 621 (drain) and 176 (no drain) patients. The odds ratio analysis for sialocele/seroma formation in patients undergoing parotidectomy reveals no statistically significant difference between the 2 groups (OR = 0.45, CI = 0.17 to 1.18, P = .10). The studies showed a moderate degree of heterogeneity (I2 = 61%, P = .03). A meta-regression was also performed for confounding variables influencing the occurrence rates of sialoceles/seromas. We found that none of the covariates once removed yielded statistically significant results, with the confounding variables removed being age (Beta: −0.24, 95% CI: −0.61 to 0.13), gender (Beta: −0.056, 95% CI: −0.056 to 0.05), tissue sealant use (Beta: −1.054, 95% CI: −2.78 to 0.67), and pressure bandage use (Beta: −1.31, 95% CI: −2.72 to 0.098). This can be seen in Table 3. A sensitivity analysis using the I2 statistic was conducted for Figure 4 using a leave-one-out technique. Removing the study by Reerds et al 4 resulted in the greatest reduction in heterogeneity (I2 = 24%), and the results remained non-significant (OR: 0.24, 95% CI: 0.29 to 1.59). This can be seen in Figure 5. Odds ratios related to studies have also been done for Figure 4 for relevant covariates, as demonstrated in Figure 6.
A Meta-Regression for Factors Predicting Sialocele/Seroma.
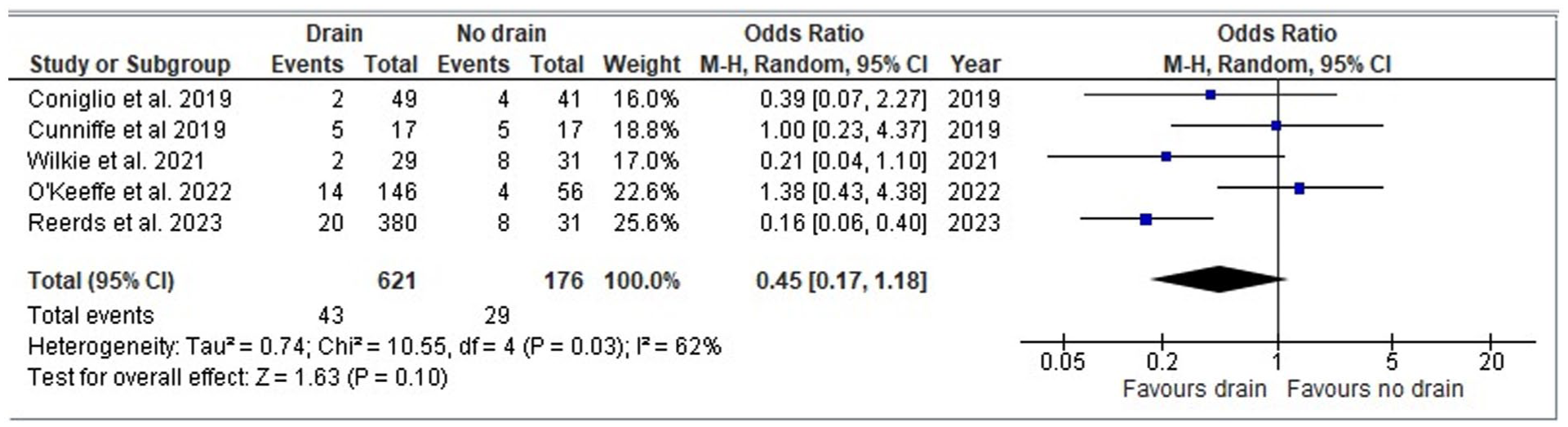
Forest plot for odds ratio analysis between drain versus no drain in parotidectomy patients – sialocele/seroma.
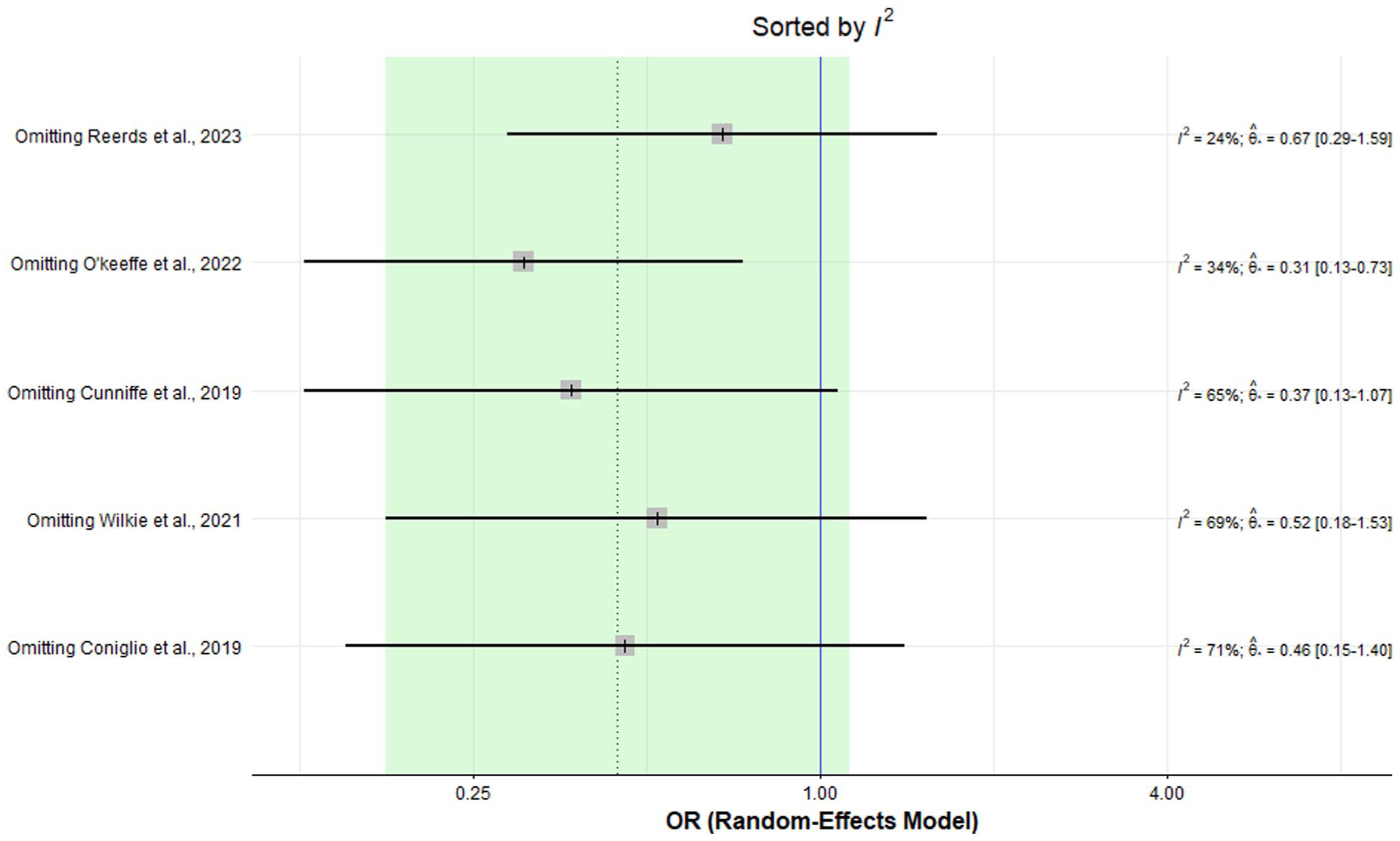
Meta-analysis using a random-effects model for sialocele/seroma.
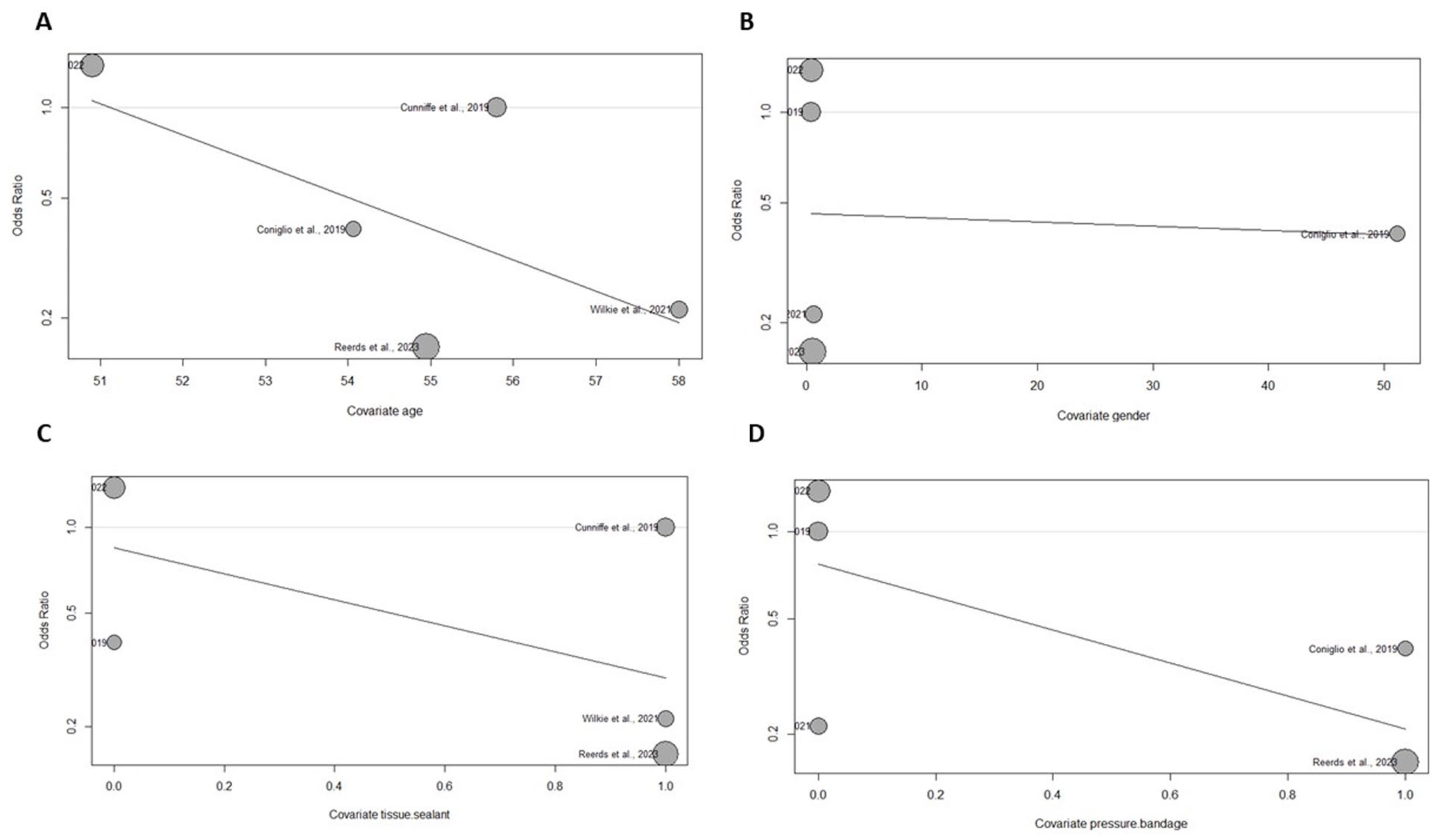
Odds ratios related to covariates relative to sialocele/seroma rates.
Although numerous additional studies reported length of stay (LOS), quantitative analysis was not feasible due to large discrepancies in reporting the observations and in outcome measures and treatment arms, resulting in insufficient data to do suitable statistical analyses. Five studies, including Chua and Goh, 8 Chudek et al, 9 Cunniffe et al, 11 O’Keeffe et al, 19 and Wilkie et al, 23 all reported LOS, with mean values indicating shorter hospital stays for patients without drains. Similarly, Reerds et al 4 reported prolonged hospitalization in 58 of 380 patients (15%) with drains versus 2 of 31 patients (6.5%) without drains. However, most prolonged stays were attributed to factors unrelated to drain placement (eg, drowsiness, nausea, urinary retention, hypertension). Only 1.3% of patients in the drain group experienced post-operative hemorrhage compared to 0% in the drainless group, a difference too small to allow meaningful conclusions.
Discussion
Summary of Main Findings
The current meta-analysis evaluated the post-operative complications (rates of hematoma, seroma, and sialocele) and length of hospital stay between drainless parotidectomies versus parotidectomies with drain insertion. Twenty-one studies were included, encompassing a sum of 3138 individuals who underwent parotidectomy (2263 patients with drain inserted, and 875 with no drain inserted). Only 5 studies were included in the quantitative analysis due to wide variations in reporting outcomes. The overall quality assessment demonstrated good quality in 18 studies, fair quality in 1 study, and low risk of bias was identified in 1 RCT, and some concerns of bias in 1 RCT (due to lack of information regarding allocation concealment and some concern of bias in selection of the reported result). Pooled results demonstrated that drainless parotidectomy has comparable outcomes to parotidectomies performed with routine drain insertion, with no statistically significant difference in the post-operative hematoma, seroma, and sialocele formation. In addition, there was a statistically significant shorter hospital stay for the cohort of patients without drains. When comparing single-arm trials of drain versus drainless parotidectomy, hematoma rates were found to be comparable (1.03% vs 0.5%, respectively), whereas sialocele and seroma rates were observed to be slightly greater in drainless parotidectomies in comparison to parotidectomies where drains were inserted post-operatively (11.5% vs 6.4%, respectively).
Interpretation of Findings and Clinical Implications
The use of drains routinely in parotidectomy remains an area of controversy among head and neck surgeons. 1 Therefore, there has been a growing body of research directed toward studying the use of routine drain insertion in various head and neck procedures. The use of drains is associated with significant morbidity in terms of increased pain and discomfort, increased risk of drain site infections, and prolonged hospital stays leading to increased healthcare costs.24,25 In the early 1990s after the emergence of the practice of outpatient thyroidectomy, Steckler was one of the first to transfer this practice to parotidectomy and report success with outpatient parotidectomy in 1991. 3 While the main idea of drainless parotidectomy is to facilitate outpatient surgery, there have been numerous studies reporting discharging patients with a drain in-situ and subsequently removing them in an outpatient setting. 4 The transition of routine neck drain insertion to drainless parotidectomy was described by Coniglio et al 5 in 2019 in their practice after demonstrating comparable outcomes. 5 Nevertheless, it is vital to note that the majority of included studies used hemostatic agents or fibrin tissue sealants intra-operatively or applied pressure bandages post-operatively when performing drainless parotidectomy. The use of such agents is associated with increased healthcare costs, and therefore, the argument toward performing a drainless parotidectomy with the addition of fibrin sealants with the effort and intention to reduce healthcare costs might be counterintuitive. In addition, due to wide variations in reporting baseline characteristics of type of parotidectomy (total vs superficial parotidectomy), whether concurrent neck dissection was involved and type of pathology of the parotid mass, it is difficult to draw meaningful conclusions regarding post-operative complication rates between drain and drainless parotidectomy for these subsets of patients. However, with the increasing body of evidence that demonstrates both the safety and feasibility of a drainless approach, as well as the evidence provided by the current meta-analysis, performing drainless parotidectomy offers a safe and non-inferior alternative to drain placement, with evidence suggesting comparable complication rates and shorter hospitalization. Importantly, the insertion of drains and routine admissions may expose patients to unnecessary discomfort, infection risk, and increased healthcare costs without clear benefit. Our findings therefore support the view that, for most appropriately selected patients, drainless parotidectomy should be considered a standard and cost-conscious approach rather than an experimental or provisional technique.26 -30 These include parotidectomy for benign pathologies, and parotidectomy with no concurrent neck dissection.
In addition, the option of discharging patients with a drain left in situ has also been shown to be safe and feasible in contemporary series, including the study by Reerds et al. 4 This approach offers a practical compromise in situations where drainless parotidectomy is not deemed safe, allowing for early discharge while still addressing concerns about post-operative collections. Incorporating this strategy into practice may further expand the opportunities for outpatient management of parotidectomy patients. 4
Comparison With Previous Meta-Analyses
Flach et al 31 conducted a meta-analysis encompassing a total of 3664 patients (1646 in outpatient group and 2018 in inpatient group) to describe the safety and feasibility of outpatient parotidectomy compared to inpatient parotidectomy. Their results demonstrate comparable outcomes of outpatient parotidectomy versus inpatient parotidectomy with no statistically significant differences in development of post-operative complications including hematoma, seroma, sialocele, facial nerve paresis, wound infection, and re-admission rates. Overall, the risk of developing hematoma was lower in the outpatient cohort when compared to the inpatient cohort (pooled OR = 0.45; 95% CI = 0.11 to 1.92; P = .28). In terms of seroma formation, there was no statistically significant difference between the groups (pooled OR = 0.79; 95% CI = 0.21 to 3.03; P = .74). There were variations among the included studies in terms of use of drain, therefore this was not directly assessed. 31
Bajwa and colleagues conducted a meta-analysis of RCTs to evaluate the effectiveness of fibrin sealants in soft tissue surgery of the head and neck, with only one study by Maharaj et al that looks at the use of fibrin sealants in parotidectomy, with supporting evidence that their use is associated with a lower mean total drainage volume and lower hematoma/seroma formation rates in comparison to standard of care parotidectomy with routine drain insertion.14,27 This is supported by findings of Conboy and Brown who reported no wound complications and found a health economic benefit in their study where they performed 21 parotidectomies using fibrin sealants without a drain in a day surgery setting. 28 While there was no direct comparison of drainless versus drain parotidectomy, the use of fibrin sealants appears to be associated with less drain output and might therefore be used in a drainless setting.
Allen et al 32 systematically reviewed the literature to compare surgical outcomes in parotidectomy using hemostatic devices (such as the HARMONIC® Scalpel Ethicon, Johnson & Johnson and LigaSure™ Medtronic) with traditional scalpel and cautery. Three studies included in their analysis showed a statistically significant lower drainage volume with the use of hemostatic devices in comparison to traditional methods. The mean difference estimate was −25.98 ml (95% CI, −26.33 to −25.64), which significantly favored treatment using hemostatic devices (P < .01). However, no direct comparison between drainless parotidectomy and parotidectomy with routine drain insertion was performed. 32
Conclusion and Significance
The current meta-analysis demonstrates comparable post-operative outcomes between drain versus drainless parotidectomy, with shorter hospital stays in the drainless cohort. However, it is also important to note the trend toward increased seroma rates when comparing single-arm trials. This is in keeping with findings from previous systematic reviews and meta-analyses previously published in literature. Thus, based on current findings, supported by findings in literature, it is not entirely clear or justifiable to confidently suggest that drainless parotidectomy can replace the current standard practice of routine drain insertion. Additional RCTs are required to consolidate the quality and power of the presented evidence.
Methodological Considerations and Limitations
To our knowledge, this is the first meta-analysis that thoroughly investigated the post-operative outcomes and length of hospital stay between drain versus drainless parotidectomy. Nevertheless, this study is not without its limitations. The studies included were of different study designs, with only two of them being RCTs, thus demonstrating the need for higher quality research on this topic. The vast majority of included studies were predominantly retrospective cohort studies mainly conducted at single institutions. Therefore, the included studies are subject to potential reporting bias and selection bias. In addition, there were wide variations in reporting complications among included studies leading to significant heterogeneity and limiting the ability to perform a quantitative analysis. Heterogeneity can also be attributed to differences in baseline patient characteristics such as pathology of parotid tumor, sample size, and the variety in the procedures performed. Handling studies with no rare events in certain arms is also a technical limitation to be highlighted; and was approached by implementing a random-effects model to account for interstudy variability. The presence of multiple studies with zero rare events, however, may still impact the precision and interpretation of our results and should be highlighted. Additionally, a sub-analysis comparing outcomes by type of tissue sealant was not feasible, as included studies did not consistently stratify complications according to the specific agent used.
The observed reduction in hospital stay among drainless patients should also be interpreted with caution, as same-day discharge may reflect surgeon preference or institutional protocols rather than the inherent efficacy of the drainless approach. This potential confounding factor limits the ability to draw definitive causal inferences regarding the relationship between drain omission and shorter hospitalization.
Conclusion
Overall, our study showed that drainless parotidectomy has comparable post-operative complication rates and lower hospital stay in comparison to parotidectomy performed with routine drain insertion. The use of fibrin sealants and hemostatic agents also appears to lower drain output and can therefore be employed in a drainless setting. However, these are associated with increased healthcare costs. While limitations remain in the literature, the current body of evidence demonstrates that drainless parotidectomy is not inferior to parotidectomy with drains and is associated with shorter hospital stays and avoidance of drain-related morbidity. Thus, there appears to be no compelling reason to mandate routine drain insertion in modern parotidectomy practice, though further high-quality RCTs would strengthen this conclusion.
Footnotes
Acknowledgements
The authors would like to thank Teruko Kishibe, MLIS (she/her), Information Specialist at Unity Health Toronto, for her invaluable assistance in developing the search strategy and providing guidance on the methodology of the screening process for this systematic review and meta-analysis.
Ethical Considerations
No exemption was required for this paper. This research did not involve direct patient or animal contact, therefore, ethical approval and informed consent are not applicable. This study did not require approval or exemption from the Institutional Review Board as it did not involve any direct patient or animal contact.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.