
Abstract

Significant Statement
The petrosquamosal sinus is a persistent embryonic emissary vein coursing along the temporal bone tegmen. Though often overlooked, its population prevalence is estimated at 11%, with higher rates in patients with chronic ear disease. Preoperative identification on high-resolution imaging is paramount for surgical planning to prevent inadvertent intraoperative hemorrhage during otologic procedures such as mastoidectomy, thereby enhancing patient safety.
Case Presentation
A 33-year-old man was referred to our department for the evaluation and management of a left-sided attic cholesteatoma. Otoscopic examination revealed a retraction pocket in the pars flaccida of the left tympanic membrane, with associated purulent discharge. Pure tone audiometry confirmed a conductive hearing loss of 30 dB. An initial high-resolution computed tomography (CT) scan of the temporal bones demonstrated a soft tissue density occupying the epitympanum and mastoid cavity. The mastoid was noted to be sclerotic and poorly pneumatized, findings consistent with long-standing chronic ear disease and pars flaccida cholesteatoma. Incidental to these findings, a tortuous bony sulcus was observed traversing the mastoid tegmen, appearing to connect the sigmoid sinus with the region of the glenoid fossa. To definitively characterize a suspected vascular anomaly, a dynamic CT angiography (CTA) of the temporal bone was performed. The CTA clearly depicted a patent petrosquamosal sinus (PSS) originating from the sigmoid sinus, coursing anteriorly within a bony canal, and ultimately draining into the retromandibular vein (Figures 1-3). The patient subsequently underwent a canal wall down mastoidectomy and tympanoplasty. Forewarned by the preoperative imaging, the surgical plan was modified to mitigate the risk of vascular injury. Meticulous care was taken during drilling near the tegmen to avoid exposing the PSS. A portion of the epitympanum, obscured by the bony overhang containing the sinus, was inaccessible to direct microscopic visualization. Therefore, an endoscope was utilized to inspect this hidden area and ensure complete removal of the cholesteatoma. The surgery was completed successfully without any hemorrhagic complications, and the patient’s postoperative course was uneventful.
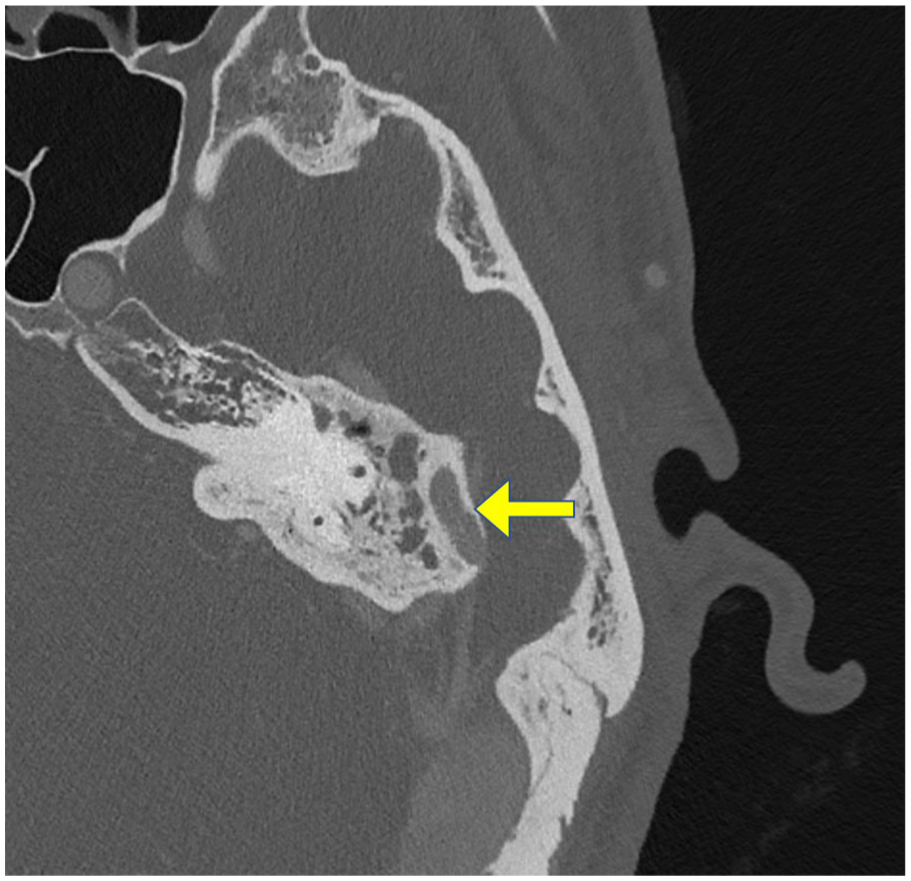
Axial computed tomography of the temporal bone showing a contrast-enhanced tortuous vessel (arrow) traversing the mastoid tegmen, which appears to connect the sigmoid sinus with the region of the glenoid fossa.
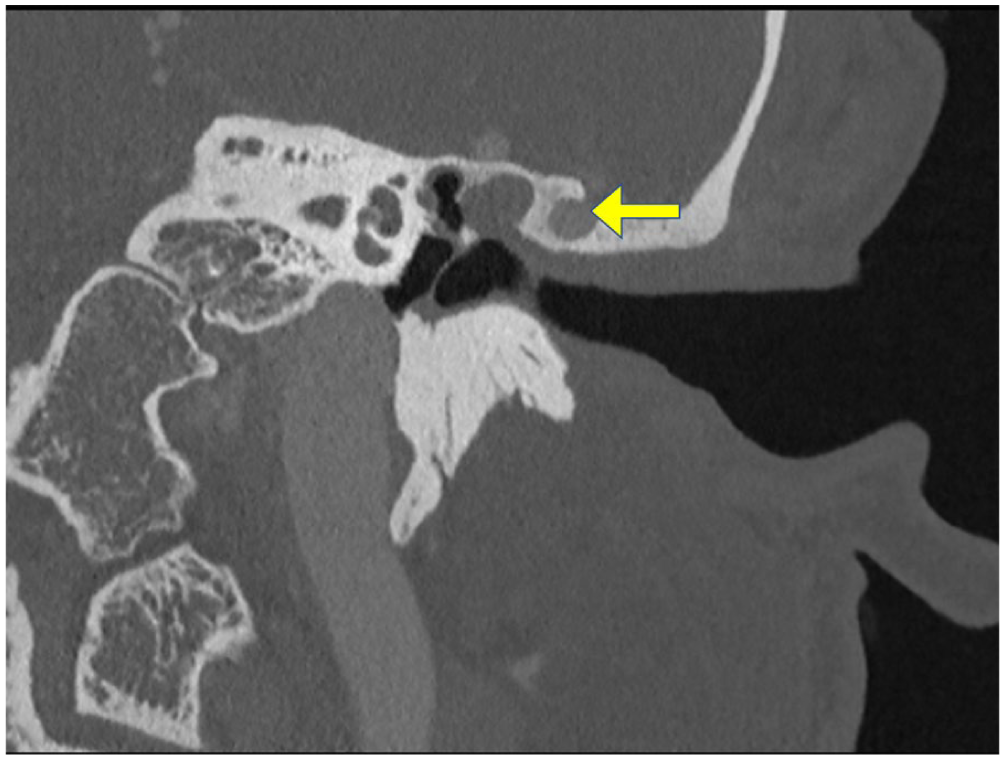
Coronal computed tomography image of the temporal bone showing a contrast-enhanced vessel (arrow) coursing through a bony canal.
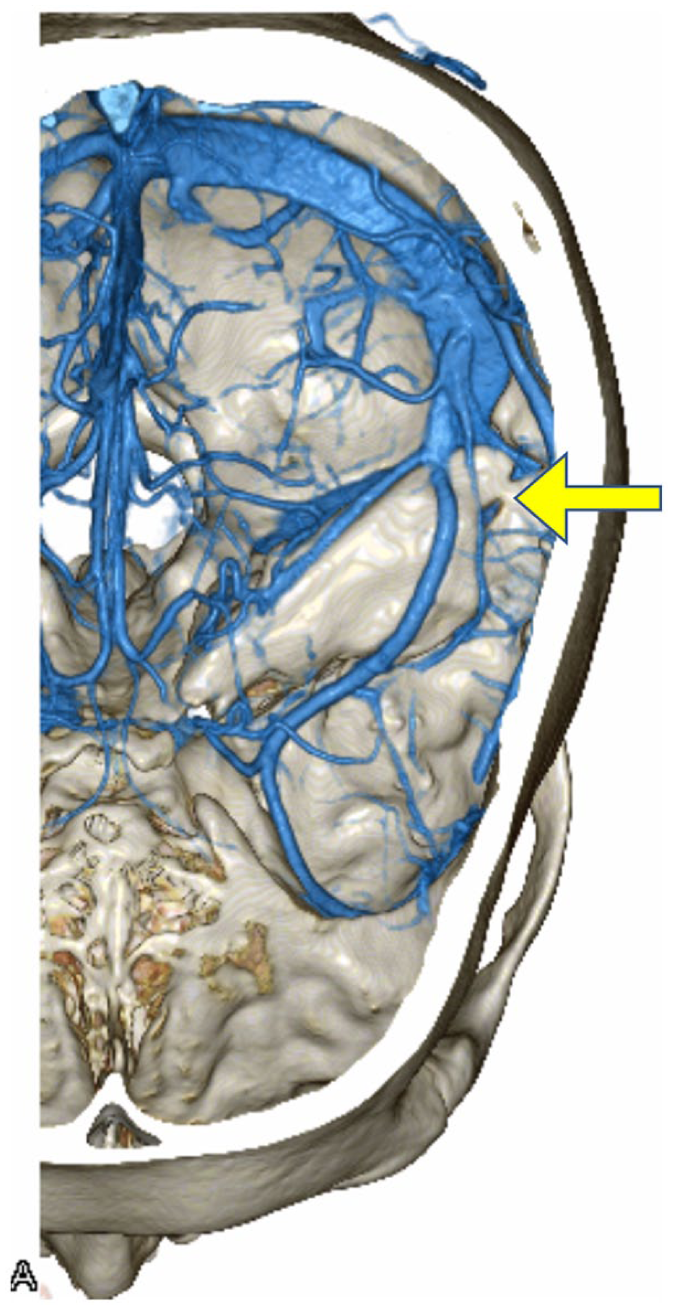
Three-dimensional computed tomography angiography reconstruction demonstrating a patent petrosquamosal sinus (arrow) originating from the sigmoid sinus, coursing anteriorly within a bony canal, and draining into the retromandibular vein.
Discussion
The PSS is an embryonic emissary vein that provides a communication between the intracranial dural sinuses and the extracranial venous system. 1 It originates from the transverse-sigmoid sinus junction and drains into the retromandibular vein or pterygoid venous plexus. In most humans, this channel regresses during late fetal development as the internal jugular vein becomes the dominant cerebral venous outflow pathway. Its persistence into adulthood is an anatomical variant of significant clinical importance for the otologic surgeon.
Although historically considered rare, the true prevalence of the PSS has been debated. A recent meta-analysis estimated the overall population prevalence at 11.1%, 1 indicating that PSS is not an uncommon finding. Moreover, its prevalence is significantly elevated in temporal bones exhibiting radiological signs of chronic otitis media and poor pneumatization, with rates reported as high as 45.7%. 2 The sclerotic mastoid observed in our patient is consistent with this high-risk anatomical phenotype, highlighting the importance of careful radiological review in these cases.
The primary clinical significance of an unrecognized PSS is the risk of life-threatening hemorrhage during mastoid surgery. Inadvertent injury to this vessel can lead to profuse venous bleeding that obscures the surgical field and is difficult to control. Further complications include air embolism and iatrogenic thrombosis of the dural sinuses resulting from attempts at hemostasis, particularly with the migration of bone wax. 3 In rare instances where the PSS serves as a dominant or sole venous outflow pathway due to contralateral sinus hypoplasia or aplasia, its ligation could have catastrophic consequences, including venous infarction and death.
This case exemplifies the indispensable role of modern, high-resolution imaging in contemporary otologic surgery. High-resolution CT is the primary modality for identifying the bony canal or groove housing the PSS. When such a channel is suspected, its vascular nature should be confirmed with CTA 4 or magnetic resonance venography. 5 As demonstrated here, this diagnostic diligence allows for precise preoperative planning and intraoperative modification of surgical technique—such as the adjunctive use of an endoscope—to navigate these challenging anatomical variants safely. Careful preoperative radiological assessment is therefore essential to anticipate the presence of a PSS and prevent serious surgical complications.
Footnotes
Ethical Considerations
Ethical approval to report this case was obtained from the Clinical Research Ethics Review Committee of Mie University Hospital (H2021-114).
Consent for Publication
Written informed consent was obtained from the patient for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, H.S., upon reasonable request.