
Abstract
Objectives:
Foreign body (FB) ingestion is a common problem in pediatric populations. The aim of this study was to investigate the epidemiological, clinical features, and outcomes of pediatric esophageal foreign bodies ingestion with particular focus on complicated cases.
Methods:
We retrospectively reviewed all pediatric cases diagnosed with esophageal foreign body (EFB) from January 2014 to December 2022. We analyzed patient characteristics, foreign body types, sites and duration of impaction, clinical manifestations, treatment outcomes, and complications.
Results:
Among the 95 cases, 56 were boys and 39 were girls, with a median age of 4 years (3-7 years). The average consultation delay was 6 hours. The most common symptom was dysphagia (30.5%). All patients had neck and chest X-rays. The upper esophagus was the most common site of impaction (62.1%). EFB included coins and blunt objects (87.4%), bones and sharp items (9.5%), and button batteries (2.1%). Ninety-four patients underwent rigid esophagoscopy, and foreign bodies were successfully removed in 75 cases. Complications occurred in 6.3% of cases, including minor mucosal lesions of the esophagus, bronchospasm, esophageal stenosis, and esophageal perforation. Main predictors of complications were sharp FB and button batteries.
Conclusion:
Rigid esophagoscopy remains an effective approach for foreign body removal in children. Clinicians should be mindful of these complications mainly in cases of sharp FB and button batteries. To prevent dangerous complications, it is essential to emphasize parental education and prompt and accurate diagnosis to opt for the suitable endoscopic approach.
Introduction
Foreign body (FB) ingestion is a frequent pediatric emergency. According to the American Association of Poison Control Centers’ National Poison Data System 2018, there were 66 519 foreign body ingestions in children under 5 years of age. 1 Although, most ingested FBs pass spontaneously through the gastrointestinal tract, 10% to 20% remain lodged in the esophagus and require endoscopic removal. 2 Coins are the most frequently ingested items in children.1,3 Typically, their removal does not lead to serious complications. However, many other ingested foreign bodies are particularly harmful and can be life-threatening, including button batteries, magnets, and sharp items. 4 In addition, clinical symptoms are not specific, especially in very young children, and many cases are asymptomatic, which can lead to delayed diagnosis and management. Such delays increase the rate of complications and raise the overall costs for pediatric esophagoscopy. 5 Hence, early diagnosis and removal of esophageal FB is crucial for a better outcome. Indications, timing of endoscopic removal and retrieval tools used were clearly described.6,7 Both rigid esophagoscopy (RE) and flexible one (FE) have comparable efficacy and safety, and the postoperative course is usually uneventful. 8 Rarely, complications may occur and be fatal such as esophageal mucosal laceration, perforation, or tracheoesophageal fistula.
These complications are usually related to the FB characteristics, the management delay, the operator experience, and the removal approach adopted.
In this study, our aim was to describe both epidemiological and clinical features in addition to the outcome of pediatric esophageal foreign bodies ingestion with particular focus on complicated cases.
Through this study, we tried to highlight diagnostic keys, therapeutic challenges and to contribute to clinical approach improvement of this common pediatric emergency.
Patients and Methods
Setting and Design
A retrospective chart review was performed in the Oto-Rhino-Laryngology Department of the Rabta Hospital in Tunis. We included all patients under 15 years of age and managed for esophageal FB (EFB) during a period of 9 years, from January 2014 to December 2022. Cases were identified by reviewing consultation records, clinical symptoms, X-ray or cervicothoracic (CT) scan and endoscopy reports, and follow-up records. We excluded cases whose imaging or endoscopy showed no evidence of FB in the esophagus, and those with incomplete records. In all cases, a RE was performed under general anesthesia after at least 6 hours nil per os. A rigid esophagoscope with an appropriate diameter was inserted to explore the oral cavity and the esophageal tract. Foreign bodies were removed using appropriate grasping forceps. A postendoscopic clinical and radiographic evaluation was performed for all cases. Oral intake was then permitted 6 hours after RE with normal evaluation. If oral intake was tolerated and went smoothly, patient was then discharged. However, in case complications were suspected during endoscopy or at postendoscopic evaluation, a multidisciplinary management including otorhinolaryngologist, pediatric surgeons, and pediatricians was conducted.
Data Collection
The following demographic, clinical, and endoscopic data were collected and analyzed: age, gender, type, number and location of FBs, symptoms after FB ingestion, duration and location of FB impaction, X-ray or CT scan, endoscopy reports, and complications related to the episode. Management and outcomes were recorded retrospectively. For complicated cases, relevant images were included to better contextualize the study findings.
Statistical Analysis
Categorical data were presented as a number and percentage (%). Since age and duration of the FB impaction were not normally distributed, the median and interquartile ranges were used to describe the data. Comparisons of continuous variables were performed using the student’s t-test and Mann–Whitney test. Categorical variables were compared using Pearson’s Chi-square test and Fisher’s exact test. All tests were two-tailed, and a P value <.05 was considered statistically significant. All statistical analyzes were performed using IBM SPSS Statistics for Windows (Version 21.0; IBM Corp., Armonk, N.Y., USA).
Results
This study enrolled 95 cases of EFB. Fifty-six (58.9%) were boys and 39 (41.1%) were girls, with a median age of 4 years ranging from 3 to 7 years.
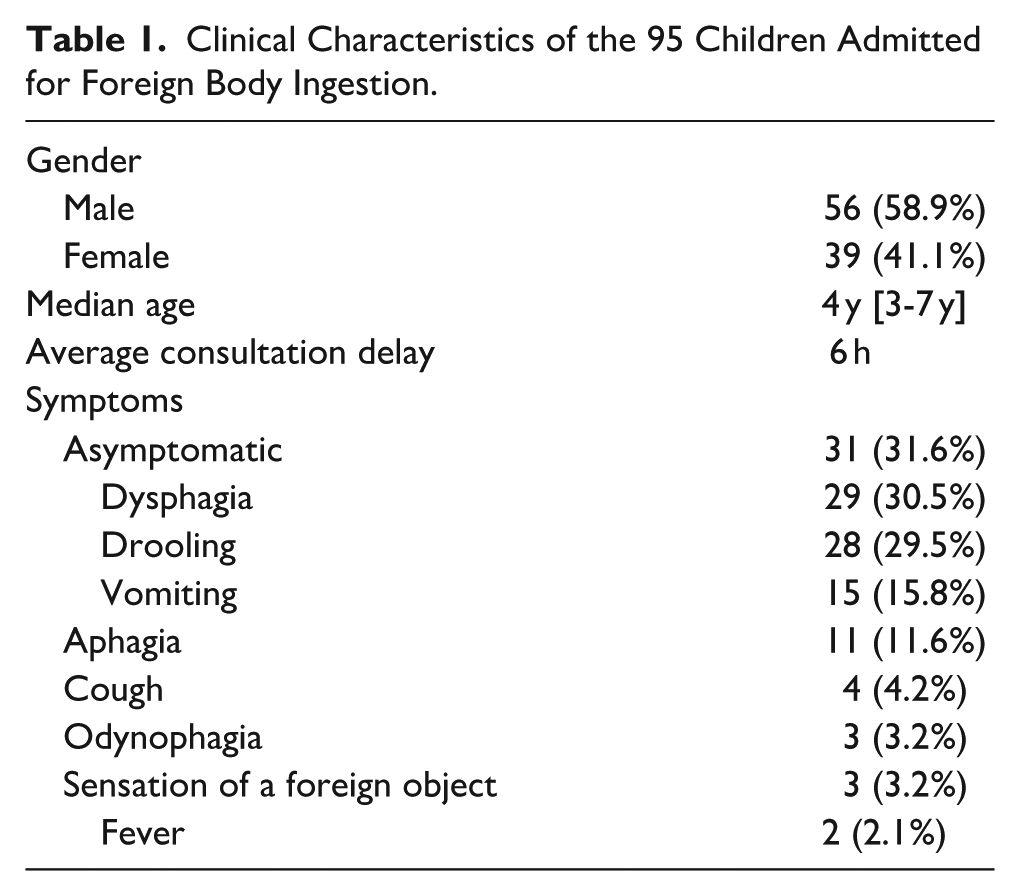
The median consultation delay was 6 hours, ranging from 2 hours to 60 days. Main symptoms were discomfort and dysphagia (30.5%). Thirty-one (31.6%) children were asymptomatic. Two cases had fever without any identifiable etiology. None of them developed complications (Table 1).
Clinical Characteristics of the 95 Children Admitted for Foreign Body Ingestion.
All patients had a standard anteroposterior plain X-ray of the neck and chest. FB was detected in 84 (87.4%) cases, mainly in the upper esophagus (62.1%, n = 59) (Figure 1). In 3 (3.1%) cases, the FB was found at the lower third of the esophagus. No radiological signs of complication were identified in all patients.
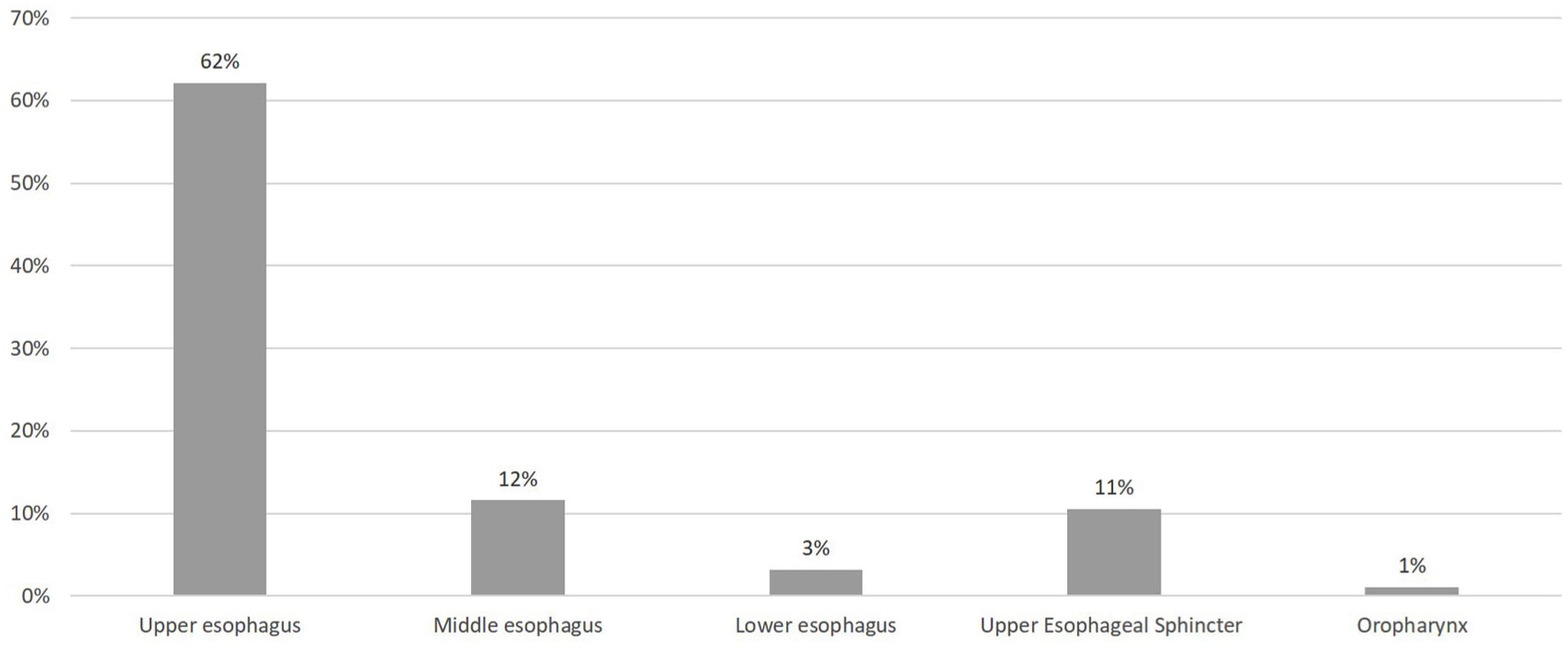
Location of the esophageal foreign body in plain X-rays.
Foreign bodies were mainly foams (83, 87.4%) followed by sharp objects (9, 9.5%). Button batteries were identified in 2 (2.1%) cases (Table 2). In 1 case, the type of esophageal FB was not specified.
Types of Foreign Bodies Extracted by Rigid Esophagoscopy.
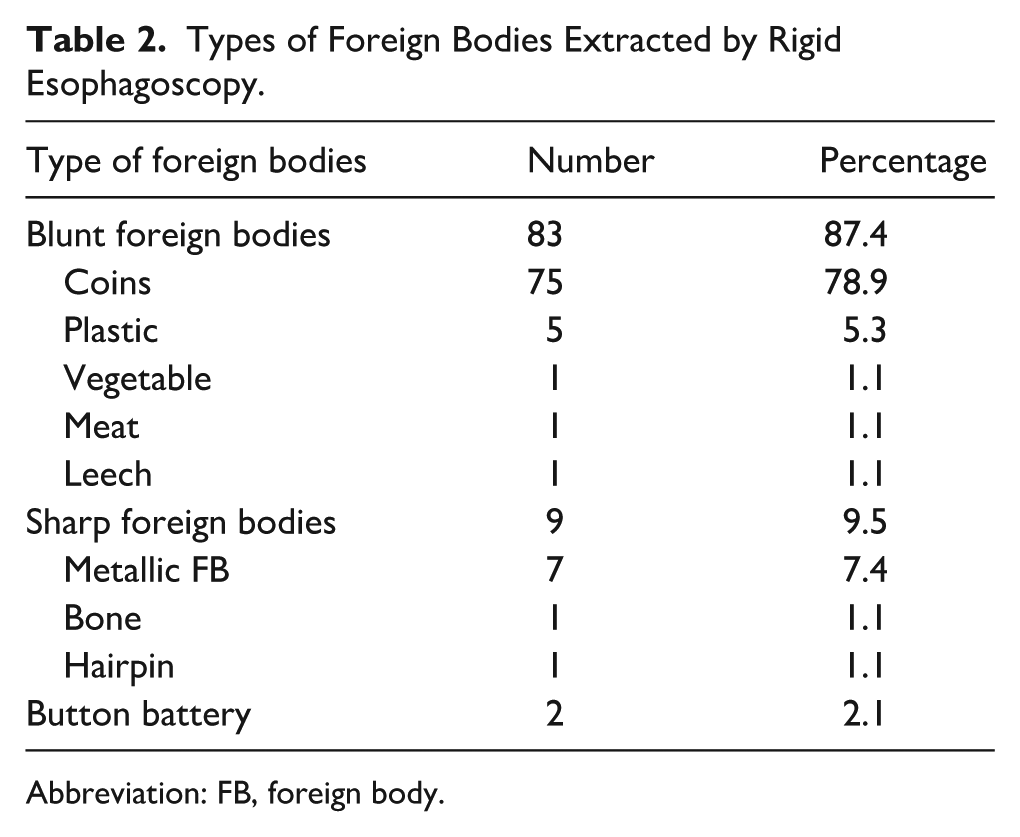
Abbreviation: FB, foreign body.
In all cases, a rigid esophagoscopy under general anesthesia was performed except for 1 patient who underwent a laryngoscopy to remove a FB in the oropharynx. FBs were successfully removed in 75 cases (78.9%). No FB was found in 14 cases during oesophagoscopy, instead 8 coins and 6 blunt-radiolucent objects were detected on the postoperative abdominal X-rays.
Complications occurred in 6 cases (6.3%) (Table 3). They included bronchospasm (1 case), minimal esophageal mucosal laceration (1 case), and esophageal perforation (2 cases). The latter complication led to hydropneumothorax with mediastinal emphysema in 1 case and pneumothorax for the other. Esophageal stenosis was identified in 2 cases of button battery ingestion (Figure 2). They were managed successfully by balloon dilatation without complications.
Clinical Characteristics of the 6 Patients With Complications.
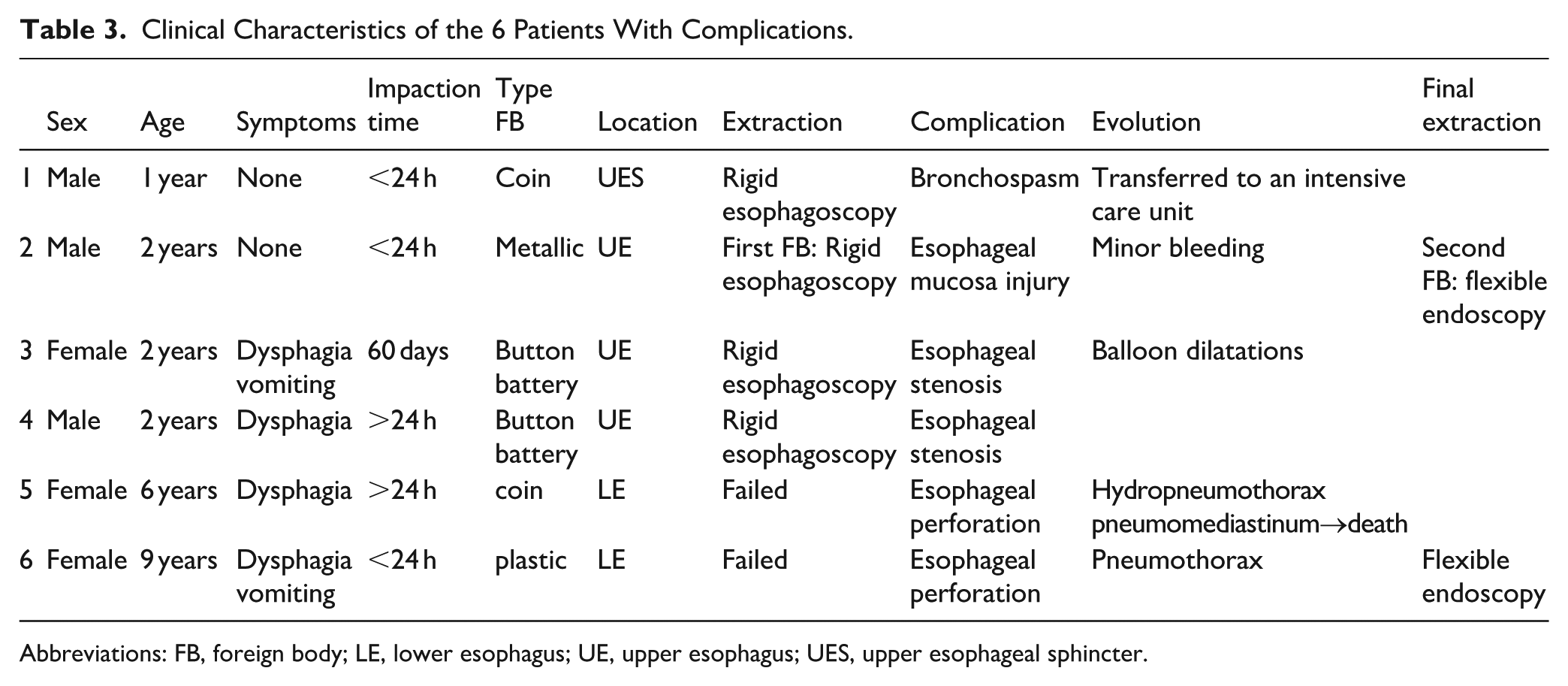
Abbreviations: FB, foreign body; LE, lower esophagus; UE, upper esophagus; UES, upper esophageal sphincter.
Esophageal stenosis confirmed by Barium swallow images.
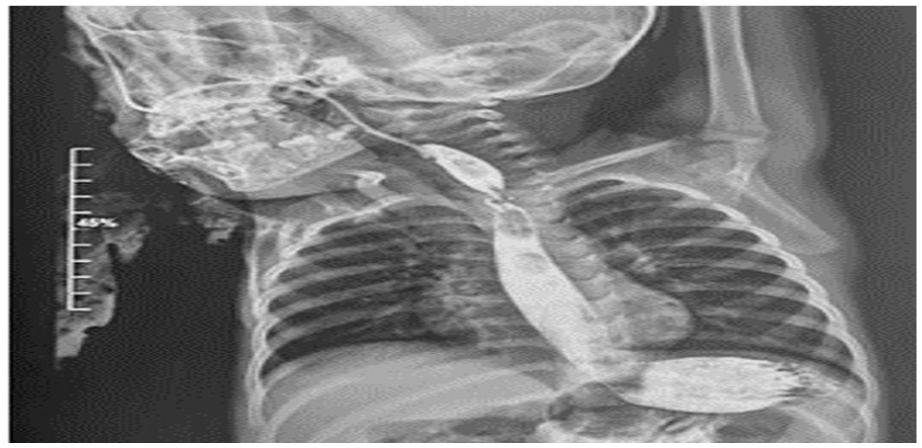
Two cases of esophageal perforation were reported. The first case was a 6-year-old girl who presented to the emergency department, 8 hours after ingesting a coin. The preoperative chest X-ray showed a round FB located in the lower esophagus. No clinical or radiological complications were noted. Rigid esophagoscopy was performed under general anesthesia, but extraction failed. Following the esophagoscopy, the patient developed fever and dyspnea. Chest radiography and cervico-thoracic computed tomography concluded to a hydropneumothorax and a pneumomediastinum (Figure 3). The patient was referred to pediatric intensive care unit (PICU) but her condition deteriorated and she died.
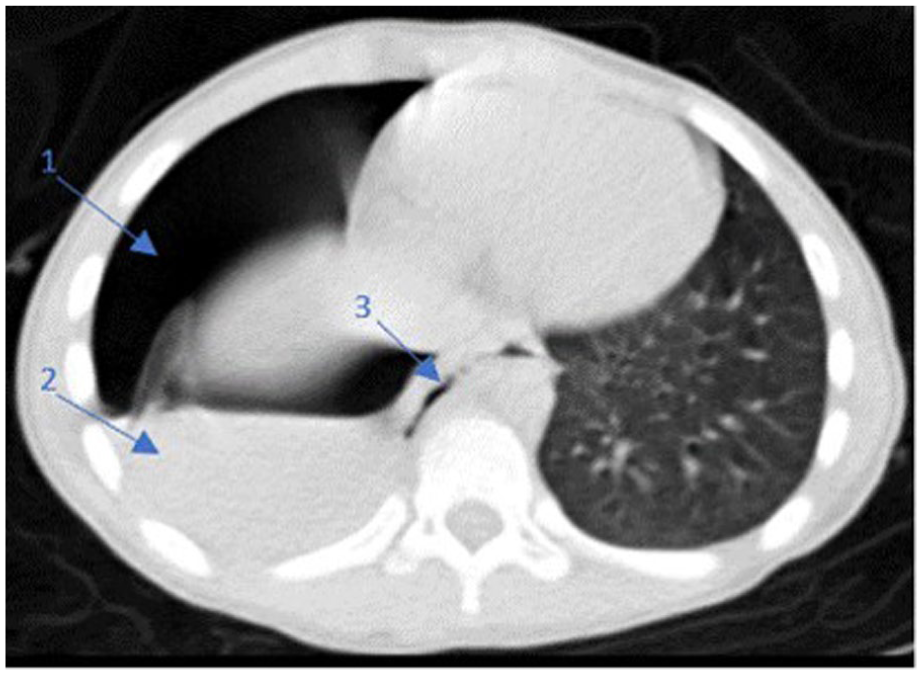
Thoracic CT scan revealing extensive right hydropneumothorax (1, 2) and pneumomediastinum (3).
The second case of esophageal perforation was a 9-year-old girl who presented for dysphagia and vomiting, 4 hours after accidental ingestion of a plastic object. On the chest X-ray, the FB was radiolucent. No clinical or radiological signs of respiratory complications were noted. Rigid esophagoscopy attempt to remove the FB from the lower third of the esophagus failed. Postoperatively, the patient presented dyspnea. Chest X-ray concluded to a pneumothorax which was drained. The patient was referred to PICU, and the foreign body was removed few days later via a flexible esophagoscopy in the pediatric surgery department.
Analysis of predictors of complications concluded that sharp FB and batteries was significantly predictive of complication occurrence after esophagoscopy (P = .022). However, esophageal FB complications were not correlated with the age of the patients (P > .05), time delay of FB removal (P > .05), or the location of the lodged FB (P > .05) (Table 4).
Risk Factors of Esophageal Foreign Body Complication.
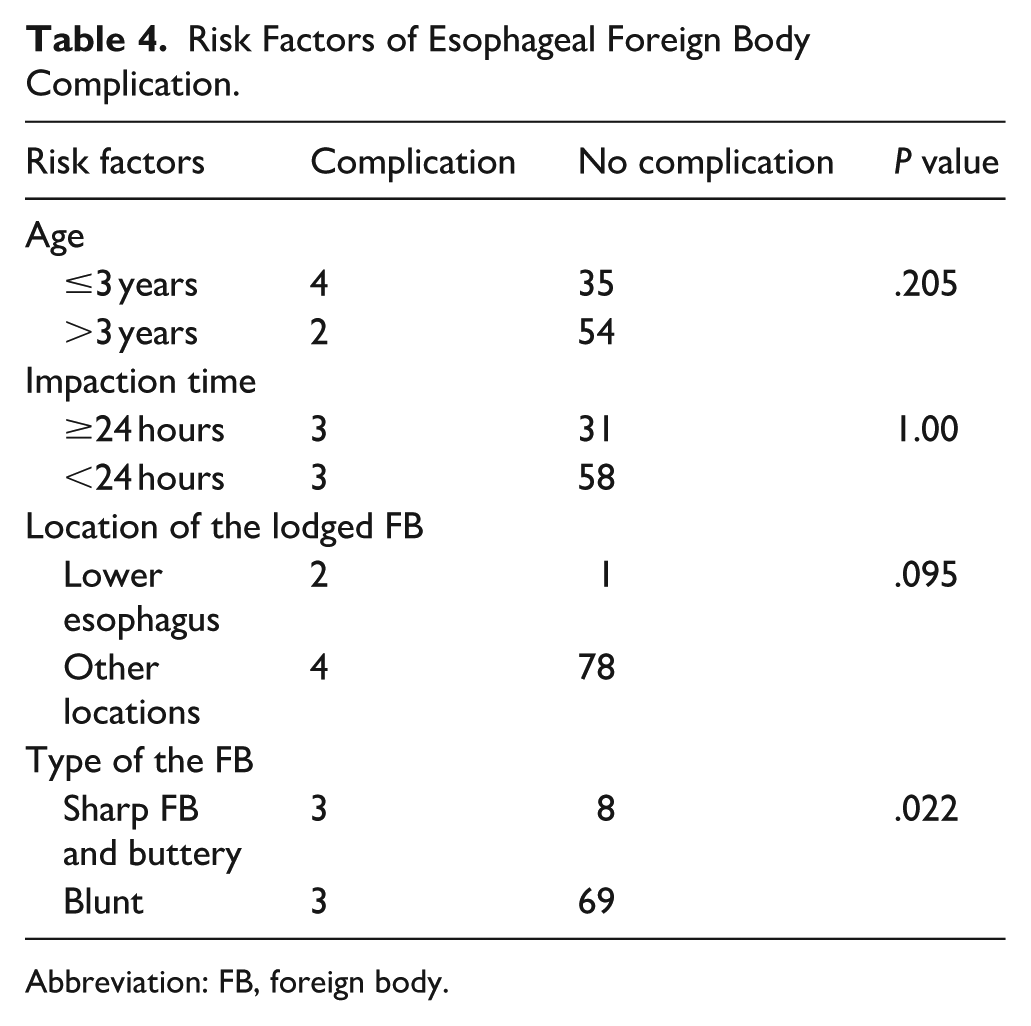
Abbreviation: FB, foreign body.
Discussion
FBs ingestion is a common pediatrics emergency occurring mainly in children under 5 years.1,3 In our study, the mean age was 4 years, which is consistent with the literature.
The esophagus remains the most common site of impaction. 6 Owing to anatomical narrowing and the common objects swallowed by children, the majority of these foreign bodies are impacted in the upper esophagus. 1 In our study, 62.1% of EFB were lodged in the upper esophagus.
Coins were the most frequent EFB in our study (78.9%), which is consistent with the results of other studies.3,9,10 Even if button battery ingestion has been increasingly described and is currently in second place after coins,11,12 only 2 cases were illustrated in our study. This may be explained by limited access of children to toys using button batteries and parents’ increasing awareness.
Main clinical complaints in children with EFBs are drooling and vomiting.2,9 However, toddler may present with atypical symptoms such as unexplained crying, hoarseness, laryngeal stridor, or dyspnea.11,13 Moreover children may be completely asymptomatic especially those without underlying esophagus pathology.14,15 In these cases, the diagnosis may be delayed and the complications rate is higher. In our study, dysphagia and drooling were the major discomforts. Children were asymptomatic in 31 cases.
Since the clinical presentation is often nonspecific, standard neck and chest X-ray imaging is mandatory for the diagnosis, particularly when an opaque foreign body is suspected. Recently, artificial intelligence models are used to detect button batteries on neck and chest X-ray, thus avoiding misdiagnosis and complication occurrence. 16 In our study, the FB was radiolucent in 12.6% of cases. Normal neck X-ray imaging should not rule out the diagnosis of FB ingestion. Consequently, for patients presenting typical clinical symptoms or those strongly suspected of having ingested a FB, an endoscopic evaluation should be conducted, even if radiography results appear normal. 17 CT scan and even MRI are highly recommended in case of a delayed diagnosis (>12 hours) especially when button battery ingestion is suspected, atypical presentation or suspected complications.11,18,19
Prompt endoscopic removal remains the milestone of EFB management in children. Both RE and FE are safe, effective, and provide excellent visualization of the esophagus.1,20 However, RE allows sheathing of irregularly shaped and sharp foreign bodies and offers less traumatic removal. The success rate of rigid esophagoscopy ranges between 87% and 98%, with an estimated risk of perforation of 3%. The success rate with FE is documented to be between 80% and 98.5%, with a reported risk of perforation below 1%. 21 To our knowledge, experts in the field have not established consensus on the type of esophagoscopy to perform, according to the time delay of presentation, age of the patient, nature of the FB, or clinical presentation severity. Gmeiner et al advocated for FE as the initial approach, citing better patient comfort, shorter procedure times, and reduced postinterventional dysphagia. They recommended reserving RE as a secondary option, when flexible endoscopy fails (6.6% in their series). 22 Ergun et al preferred RE as it allows the use of optical forceps with a strong grasping ability for thick-edged FBs and a secure removal of sharp and pointed objects inside the rigid endoscope. 6 In our current study, rigid esophagoscopy was the first-line therapy for EFB retrieval, as flexible esophageal endoscopy was unavailable in our center.
Complications associated with foreign body ingestion were described in 6.3% of cases in our study. They were mainly due to the foreign body characteristics or the removal approach itself. As in our study, the main complications are mucosal injuries and lacerations.9,23 Esophageal perforation, tracheo-esophageal fistula, and esophageal stenosis are rare but may be fatal. Esophageal perforation is rare, occurring in less than 1% of EFB cases 1%. 23 Hydropneumothorax and mediastinal emphysema, as potential complications of esophageal perforation, carry significant life-threatening risk.
In children, esophageal complications could be attributed to a spectrum of various foreign bodies, each carrying its own set of potential challenges and risks. Several studies noted that sharp or pointed items and large foreign bodies were the most commonly implicated in esophageal mucosal tears and perforations. 3 In our study, sharp items were significantly predictive of complication’s occurrence.
Multiple magnet and button batteries, commonly found in households, are frequent culprits. These objects, when ingested, pose the risk of mucosal compression, chemical leakage, and electrical damage within the esophagus.3,24
Button batteries have seen widespread use in electronic products in recent years, leading to a gradual rise in the incidence of button battery ingestion. The presenting symptoms, often nonspecific, may be misattributed to common childhood illnesses. 11 Although, esophageal necrosis and life-threatening complications may occur within 2 hours of button battery ingestion, performing esophagoscopy within such a short timeframe remains challenging. 11 Delayed diagnosis may lead to esophageal perforation and stenosis even after FB removal. In our study, the 2 cases of esophageal stenosis were due to delayed removal of the button battery. Like our study, button battery ingestion was a significant predictor of complications in previous studies.25,26
Regardless of FB characteristics, the duration of impaction is a well-established risk factor of complications. 25 In fact, timely removal of EFBs is recommended preferably within 24 hours for smooth FB, and within 2 hours for button battery to prevent prolonged mechanical stimulation and mitigate the risk of esophageal injury.18,27 In our study, the duration of lodgment was not predictive of complications. This may be attributed to the reduced number of patients with delayed management.
The site of impaction is another predictor of complications. As in our study, esophageal perforations were more frequent when the FB was lodged in the lower esophagus. This suggests that as the risk of perforation increases, the more distally the scope enters the organ. 28 Flexible esophagoscopy may be safer to manage lower esophagus FB.
Our study has some limitations. First, it was an observational and retrospective investigation. Data compilation was based on retrospective medical records and endoscopy reports with the inherent limitations of case ascertainment bias. Second, our study was carried out in a single center with an unavailable pediatric surgery department and pediatric intensive care essential for prompt management of life-threatening complications. These severely complicated patients were referred to another center. Hence, detailed data on their interventions, follow-up, and long-term outcomes was missing. Finally, due to the relatively small number of cases with major complications, such as perforations and stenosis, it was difficult to analyze the risk factors for serious complications. Therefore, additional prospective studies with larger cohorts of patients are essential to validate these findings.
In conclusion, EFBs are a common pediatric emergency. While symptomatology is often typical in older children, the clinical presentation may be misleading in toddlers and many cases are even asymptomatic. In patients with typical clinical symptoms or those strongly suspected of having ingested a FB, an endoscopic evaluation is recommended. Rigid esophagoscopy remains a reliable approach to remove foreign bodies lodged in the esophagus, but complications may occur, especially when the FB is sharp or a button battery. These complications are associated with delayed management or improper approach. To avoid complications and prevent fatal outcomes, it is crucial to prioritize the education of parents, establish a prompt diagnosis with a multidisciplinary management.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for retrospective studies. Archival patient’s data were anonymized. We anonymously reported clinical and imaging information concerning our patients.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author on reasonable request.