
Abstract

Dear Editors,
We read with great interest the report by D’Arcangelo et al, describing successful one-stage reattachment of near-complete ear avulsion without microsurgical replantation, relying on an intact skin pedicle. 1 This method achieved excellent cosmetic results while avoiding major complications. Although traumatic ear amputation (EA) is rare and microsurgical replantation remains the traditional gold standard, 2 it presents challenges including vessel reconstruction difficulty, distinguishing arterial from venous systems,3,4 and the need for specialized facilities and highly skilled microsurgeons. We commend the authors’ achievement in repairing near-complete EA (NEA). However, while the study emphasizes postoperative anticoagulation to promote venous outflow, it does not address the crucial role of drainage. We propose adapting a specialized drainage technique, routinely used in staged auricular reconstruction, to the repair of near-complete traumatic ear avulsion.
First, survival of replanted ears depends on maintaining both arterial inflow and venous outflow. The auricle’s rich vascular network with multiple anastomoses and low metabolic rate allows survival even with a narrow pedicle at the helix root. 5 Venous congestion from thrombosis or inadequate drainage, however, remains a leading cause of failure. 6 Conventional methods, including leech therapy, mechanical drainage, and heparin injection, may improve outflow but can increase transfusion requirements and prolong hospitalization. 7 In the second case reported by D’Arcangelo et al, severe avulsion with substantial bleeding yielded good results, yet refinement is possible. We propose an embedded “dual-ended single-tube” drainage system placed through the ear base, with both ends connected to a simple negative-pressure device for continuous drainage and optional irrigation (Figure 1). This configuration avoids the high irrigation pressures and potential tissue damage associated with single-ended tubes, while minimizing risks of dislodgement, kinking, or blockage. Our team has applied this method in the first stage of microtia reconstruction with consistently favorable results, and it could similarly reduce edema, prevent fluid accumulation, and enable selective topical low-molecular-weight heparin irrigation in venous congestion without impairing wound healing.
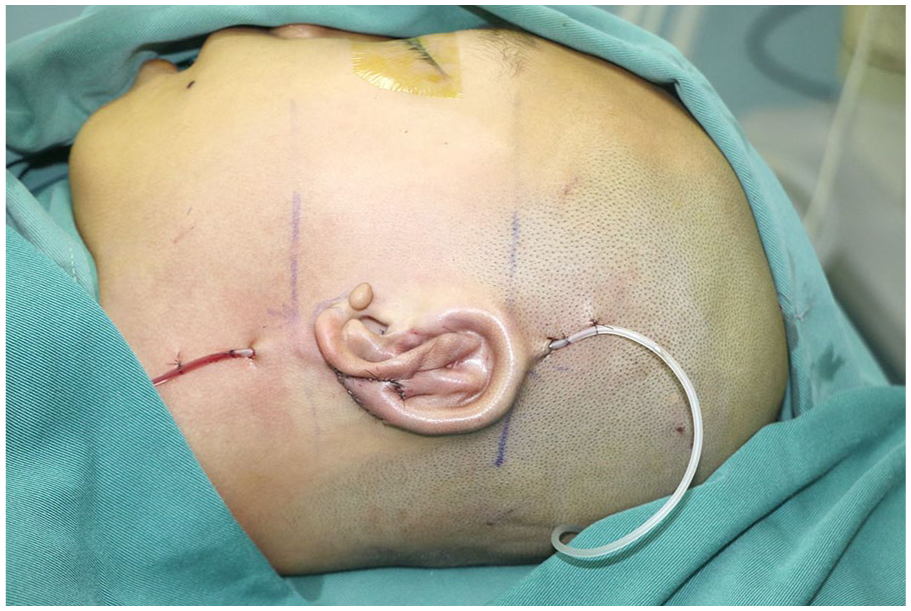
“Dual-ended single-tube” drainage technique.
Second, the mechanism and severity of injury, presence of complications, and surgical expertise are critical in selecting a reconstructive strategy. 8 For NEA involving the auricular root and periauricular soft tissues, we advocate a comprehensive approach to optimize survival and esthetics. Conchal packing with compression sutures can maintain contour, reduce exudation, and promote tissue adherence. When lobular congestion occurs from inadequate venous drainage, fine-needle puncture with topical low-molecular-weight heparin can relieve stasis, minimizing bleeding risk compared with injection, eliminating the need for complex tapering protocols, and remaining feasible in primary care settings lacking microsurgical capabilities.
In conclusion, the “dual-ended single-tube” drainage technique offers advantages over conventional single-ended drainage by improving patency, reducing pressure-related injury, and enhancing postoperative flap viability. Its extension to near-complete traumatic auricular avulsion may broaden reconstructive options and benefit more patients with complex ear injuries. We share the authors’ goal of refining surgical strategies to achieve optimal functional and esthetic outcomes.
Footnotes
Acknowledgements
We sincerely acknowledge the technical guidance provided by Professor Xiaojun Liu from the Department of Plastic and Aesthetic Surgery, Nanfang Hospital of Southern Medical University.
Consent for Publication
Written informed consent was obtained from the patient for the publication of this work, including any recognizable photographs or other identifiable information. The consent was submitted with the article, and the patient was informed that this information may be publicly available.
Author Contributions
Hanghang Zhou: investigation, writing – original draft. Chao Lian: conceptualization, writing – original draft. Jianxiong Qiao: conceptualization, writing – review and editing. Xiaojun Liu: resources, writing – review and editing. Xuanfen Zhang: supervision, writing – review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.