
Abstract

Significance Statement
This case emphasizes the educational value of recognizing rare intranasal ectopic teeth as a potential cause of unilateral nasal obstruction. It underscores the importance of correlating endoscopic findings with imaging and maintaining a broad differential to avoid misdiagnosis in routine rhinology practice.
A 36-year-old man presented with several months of progressive right-sided nasal obstruction and foul-smelling rhinorrhea. Initial management at a local clinic was ineffective, prompting referral to our otolaryngology service. Anterior rhinoscopy revealed a firm, immobile mass partially obscured by crusts in the right inferior meatus, seemingly originating from the nasal floor (Figure 1A). The computed tomography (CT) showed a well-defined, radiopaque lesion measuring 1.7 × 0.8 × 1.1 cm, attached to the maxilla and projecting into the right nasal cavity (Figure 1B). Given its central calcification and location, a nasal osteoma was initially suspected. The patient subsequently underwent endoscopic surgical excision under general anesthesia. Intraoperatively, the lesion was found to be surrounded by inflamed granulation tissue but was otherwise well demarcated. A fully developed ectopic tooth was removed without mucosal injury or bleeding (Figure 1C). Intraoral dental examination revealed a complete dentition with no evidence of agenesis or supernumerary teeth. The postoperative course was uneventful, and the patient reported complete resolution of nasal symptoms during follow-up.
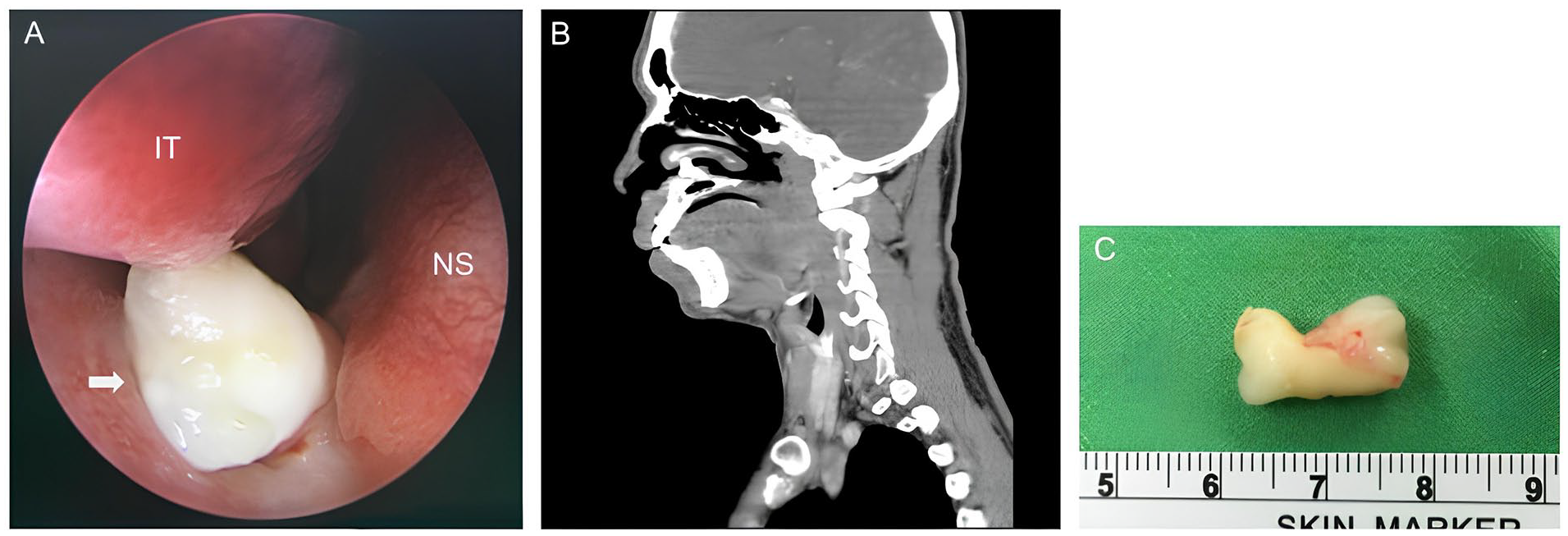
(A) Endoscopic view showing a white, hard mass (arrow) partially covered with crusts in the right IT, suspected to originate from the NS. (B) Sagittal CT scan revealing a well-defined radiopaque lesion (1.7 × 0.8 × 1.1 cm) attached to the maxilla, projecting into the right nasal cavity. (C) Gross specimen of the extracted ectopic tooth following endoscopic removal. CT, computed tomography; IT, inferior turbinate; NS, nasal septum.
Ectopic teeth developing in the nasal cavity are exceedingly rare, with an estimated prevalence of 0.1%–1% in the general population. 1 While most supernumerary or ectopic teeth are located in the palate or maxillary sinus, occurrence within the nasal cavity is highly unusual. 2 The etiology of ectopic intranasal teeth is not fully understood but may involve aberrant migration of dental lamina during embryogenesis, trauma, infection, or odontogenic anomalies. 3 Clinically, patients may present with nonspecific symptoms such as unilateral nasal obstruction, purulent or fetid rhinorrhea, epistaxis, facial pressure, or recurrent sinusitis. On endoscopy, intranasal teeth typically appear as firm white masses embedded in inflamed mucosa, often accompanied by granulation tissue or crusting. CT imaging plays a pivotal role in diagnosis, with teeth usually presenting as radiopaque structures of similar density to normal dentition. 1 However, close proximity to adjacent bony structures—such as the septum or turbinates—can complicate radiographic interpretation, leading to diagnostic confusion with osteomas, rhinoliths, or benign calcified lesions. 2 In our case, the septal location and dense calcification led to a presumptive diagnosis of osteoma, with definitive identification made intraoperatively. Differential diagnoses of radiopaque intranasal masses should include retained foreign bodies, rhinoliths, calcified polyps, ossifying fibromas, dermoid cysts, and neoplastic lesions. 3 Surgical removal is generally recommended in symptomatic patients to relieve obstruction and reduce the risk of infection, mucosal erosion, or septal perforation. 1 Endoscopic excision provides both diagnostic confirmation and therapeutic benefit. Our patient achieved full symptom resolution following endoscopic removal, underscoring the importance of considering ectopic intranasal teeth in the differential diagnosis of unilateral nasal symptoms, particularly when imaging reveals a calcified intranasal mass of unclear origin.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to Participate
Written informed consent was obtained from the patient for anonymized patient information to be published in this article.
Author Contributions
The authors confirm contribution to the article as follows: conception and design of the case report: Yung-Tsung Cheng, Keng-Ming Chang; data collection: Yung-Tsung Cheng, Keng-Ming Chang; analysis and interpretation of the case: Yung-Tsung Cheng, Keng-Ming Chang; draft manuscript preparation: Yung-Tsung Cheng, Keng-Ming Chang. All authors reviewed the results and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data underlying the results are available as part of the article and no additional source data are required.