
Abstract
Objective:
Airway management in patients with severely-narrowed tracheal lumens presents significant challenges, especially when traditional intubation methods are not feasible. In such cases, failed intubation attempts can worsen airway compromise and cause life-threatening complications. Extracorporeal membrane oxygenation (ECMO) offers an alternative approach to ensure oxygenation and ventilation during complex airway surgeries. The objective of this study was to assess the safety and feasibility of using venovenous ECMO to ensure oxygenation before attempting intubation in patients with severely-narrowed tracheal lumens undergoing head and neck surgery.
Methods:
This is a retrospective case series of 3 adult patients who underwent venovenous ECMO-assisted intubation for head and neck surgeries at a single institution between 2010 and 2023. The primary outcome was the successful establishment of an airway and the avoidance of respiratory failure during the surgical procedure.
Results:
All 3 patients successfully underwent ECMO-assisted intubation. None of the patients experienced major complications directly attributable to ECMO, and all were extubated within 24 hours postoperatively.
Conclusions:
Venovenous ECMO provides an effective strategy for managing difficult airways in patients with severely-narrowed tracheas, enabling safe anesthesia induction. This technique may be crucial in preventing complications associated with traditional airway management methods.
Introduction
Airway management poses a complex challenge in head and neck surgeries when the tracheal lumen is significantly narrowed due to radiation therapy, congenital stenosis, or, most commonly, obstruction. 1 In these cases, an unsuccessful attempt at intubation can result in further damage to the existing airway. Furthermore, induction of anesthesia results in a collapse of respiratory and airway tissues that may further obstruct the impacted airway.
For anticipated difficult airways, preventive measures can be used to avoid loss of a stable airway during the operation. Typically, mechanisms such as jet ventilation or tracheotomy could be performed to ensure adequate ventilation. However, there are scenarios in which these options are not feasible, such as obstruction below the level of the larynx. In such cases, alternative methods of intubation must be considered.
The use of extracorporeal membrane oxygenation (ECMO) has been previously described in various cases to ensure adequate respiratory support during tracheobronchial procedures. 2 Intubation itself poses risks including cardiovascular collapse from hypercapnia and hypoxia. Preemptively ensuring oxygenation via ECMO may help mitigate some of these risks. 3 Here, we describe 3 cases of successful anesthetic management of patients with severely-narrowed tracheal lumens, where venovenous ECMO was electively initiated prior to attempted intubation.
Methods
Identification of Patients
Institutional review board approval was obtained. A retrospective chart review identified 3 patients at a single institution who underwent ECMO-assisted intubation prior to head and neck surgery between January 1, 2010, and December 31, 2023. In each case, ECMO was initiated prior to anesthesia.
ECMO-Induced Anesthesia Operative Procedure
This procedure is performed in conjunction with a cardiothoracic surgery team. The patient is placed supine on the operating table, and mild sedation is used at the anesthesiologist’s discretion with careful consideration for the risk of airway collapse. The right and left groins are infiltrated with 1% lidocaine. The existing venous lines are accessed with wires, and the patient is heparinized to achieve an activated clotting time (ACT) of over 160 seconds. For the 3 cases described below, this required between 5000 and 10,000 total units. Under fluoroscopic guidance, wire placement is confirmed to be in the superior vena cava. The left common femoral vein is serially dilated, and a venous cannula is placed, with the tip just below the diaphragm. The right pulmonary vein is then similarly dilated and cannulated with the tip in the right atrium. After confirming an ACT greater than 160 seconds, venovenous ECMO is initiated. Anesthesia staff then initiates general anesthesia for the head and neck surgical team to begin.
ECMO is weaned after successful intubation and discontinued once adequate ventilation is confirmed. Protamine is administered to reverse the heparin. The case is then returned to the head and neck surgical and anesthesia teams.
Due to institutional use of ECMO equipment from more than 1 manufacturer during the study period, readers should be aware that individual patients in this series may have received support from different ECMO systems. Settings and protocols should be adjusted according to the specifications of the model being used.
Results
Case 1
A 71 year-old male presented with a mediastinal mass, which had been present for over 17 years. His medical history was significant for thyroid nodules and previous radiation to his neck as a child. He presented to the emergency department with 2 days of worsening dyspnea and nonproductive cough. A computed tomography (CT) scan revealed a partially-calcified mass originating from the left thyroid lobe that measured 9.3 × 9.5 × 7.7 cm. The mass significantly narrowed the distal trachea and displaced it toward the right. The minimum tracheal diameter was approximately 2 mm.
The patient’s physical exam findings indicated that a tracheostomy would be problematic because his distal trachea was significantly narrowed secondary to compression near the carina. In the operating room, multiple attempts to lay him flat while awake resulted in dyspnea. The decision was then made to initiate ECMO before attempting intubation. After ECMO was initiated as described previously, general anesthetic was administered. An attempt was made to place a 5.5 endotracheal tube (ETT), which could not be passed beyond the tumor, but did succeed in obtaining some ventilation. The decision was made to remain on ECMO until the tumor was excised and the ETT could be advanced.
Once the tumor was resected via sternotomy and low neck exploration (Figure 1A-D), a left chest tube was placed and the patient was weaned from ECMO. The sternotomy was closed, followed by the neck. A 6.5 ETT was placed prior to the patient’s transfer to the intensive care unit (ICU). He was extubated post-op day 1 without complications.
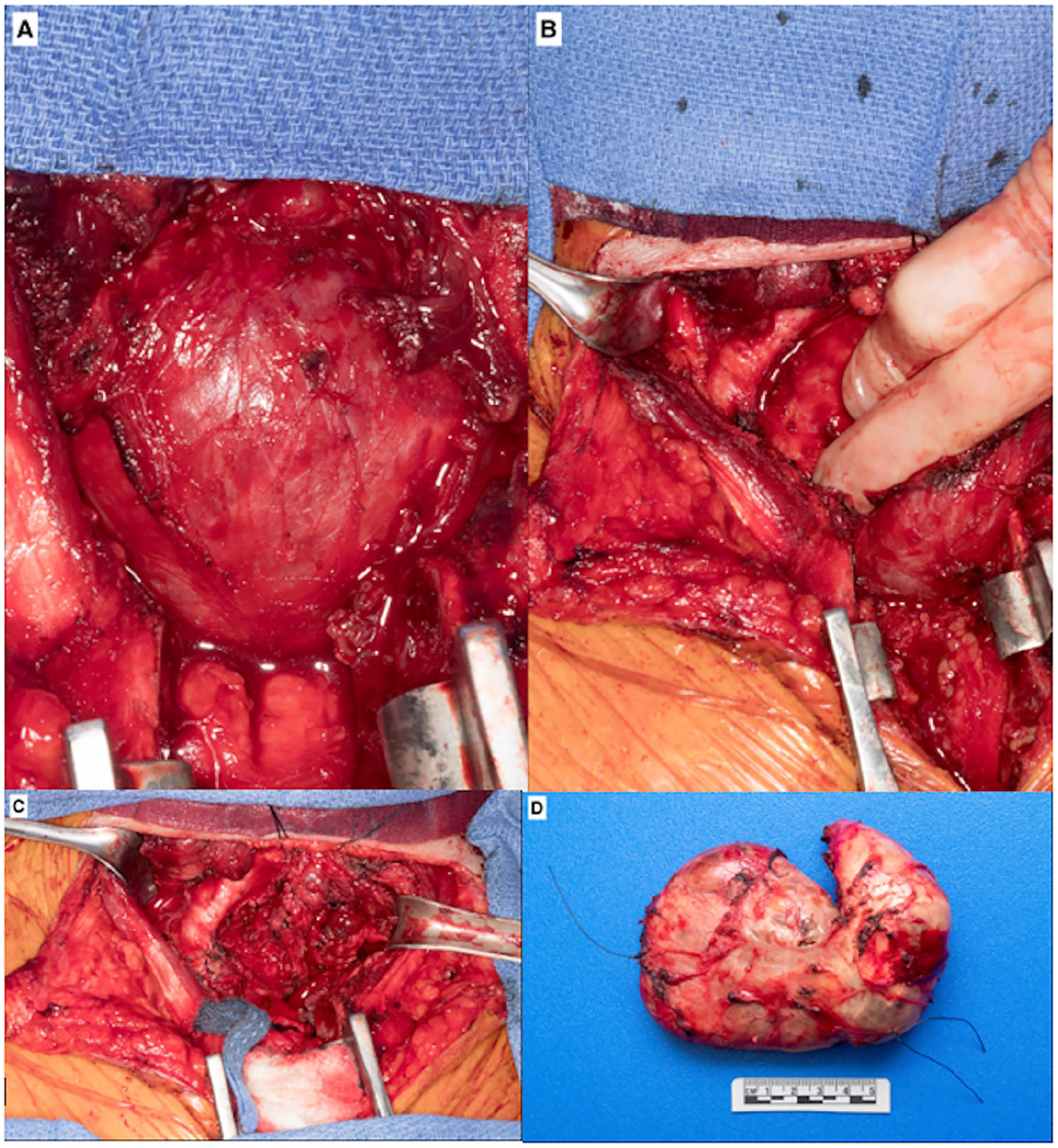
A 71 year-old male presented with a mediastinal mass originating from the left thyroid lobe that measured 9.3 × 9.5 × 7.7 cm on CT scan. His minimum tracheal diameter was determined to be 2 mm. He was electively placed on ECMO prior to the initiation of general anesthesia and intubation, and remained on ECMO until the tumor was resected via sternotomy and low neck exploration. (A) Visualization of the enlarged mass after median sternotomy was performed. The trachea is completely obstructed from view. (B) Once the mass is gently pushed to the side, the trachea can be visualized superolaterally. It is seen being severely deviated and compressed by the enlarged mass. (C) After the resection of the mass, the trachea can be more clearly visualized. (D) Fully-resected mediastinal mass with fibrous encapsulation, measuring 12.0 × 10.0 × 4.7 cm and weighing 195 g. The single stitch marks the thyroid isthmus, and the double stitch marks the inferior thyroid. CT, computed tomography; ECMO, extracorporeal membrane oxygenation.
This patient tolerated the procedure well; however, his recovery was complicated by a right pneumothorax and pneumomediastinum. These were improved by the placement of a right-sided pigtail chest tube. He recovered well and was discharged post-op day 7. Final pathology confirmed the mass to be follicular adenoma.
Case 2
A 64 year-old female presented with an enlarged multinodular thyroid, which was known about for over a year. She presented to the emergency department complaining of months of difficulty breathing that had acutely worsened in the past week. A CT angiogram of the chest revealed a large thyroid mass compressing the trachea. The minimum tracheal diameter was approximately 4 mm.
The main concern in intubating this patient was that a failed attempt to advance an ETT past the thyroid mass could result in significant airway bleeding. Tracheostomy was also not feasible because of the substernal location and enlarged size of her thyroid. Thus, the decision was made to initiate ECMO under sedation prior to initiation of general anesthesia and placement of an ETT.
After the initiation of ECMO, general anesthesia was induced and a 5-0 ETT was placed successfully. The patient was adequately oxygenated, and ECMO was discontinued. The tumor was resected without complication, and she was extubated prior to transfer to the postoperative care unit.
The patient tolerated the procedure well and recovered with no complications. Final pathology confirmed the mass to be classical type papillary thyroid carcinoma.
Case 3
A 25 year-old female with type 1 diabetes and morbid obesity (body mass index = 38) presented with severe tracheal stenosis secondary to prolonged intubation after an attempted suicide 4 months prior. She complained of persistent shortness of breath and hoarseness. She had reportedly been previously intubated for 12 days, and in the setting of type 1 diabetes, this resulted in severe cartilaginous tracheal stenosis.
A CT scan showed subglottic stenosis just below the thoracic inlet, starting at tracheal ring 2 and measuring approximately 3 cm in length. Posterior glottic stenosis extended to the level of the vocal folds. Endoscopic examination of the airway revealed the minimal tracheal diameter to be approximately 3 mm.
Given the rigid, cartilaginous nature of the stenosis, endoscopic treatment was deemed unlikely to succeed. Awake tracheotomy was not pursued given the patient’s severe orthopnea, her concern for aphonia, and the risk of injuring healthy tracheal tissue. As a result, the decision was made to perform a tracheal resection and anastomosis and to initiate ECMO before general anesthesia and endotracheal intubation.
The patient was brought to the operating room and ECMO was initiated, followed by general anesthesia. After the glottic and subglottic regions were examined using a laryngoscope, a potassium titanyl phosphate laser was used to make an incision into the posterior glottic stenosis. Balloon dilation to 18 mm at the level of the glottis was performed, then a balloon was inserted through the tracheal stenosis and serially dilated. A 6.5 Parker Flex ETT was used to attempt intubation but was unable to be advanced past the stenosis. Instead, a 5.5 Parker Flex ETT was used, which successfully passed through the area of stenosis. The laryngoscope was then removed with the ETT left in place.
Based on the evaluation of the stenosis, which involved tracheal rings 3-9, the decision was made to proceed with resection. The patient was adequately oxygenated with the orotracheal ETT, and ECMO was discontinued.
The patient was extubated prior to transfer to the ICU. She tolerated the procedure well and recovered with no postoperative complications.
Operative and Postoperative Outcomes
An airway was obtained in all 3 cases with varying degrees of difficulty. All 3 patients tolerated the procedure well and did not experience any complications from being placed on ECMO. Table 1 compiles the patient characteristics and treatment course of these 3 cases.
Patient characteristics.
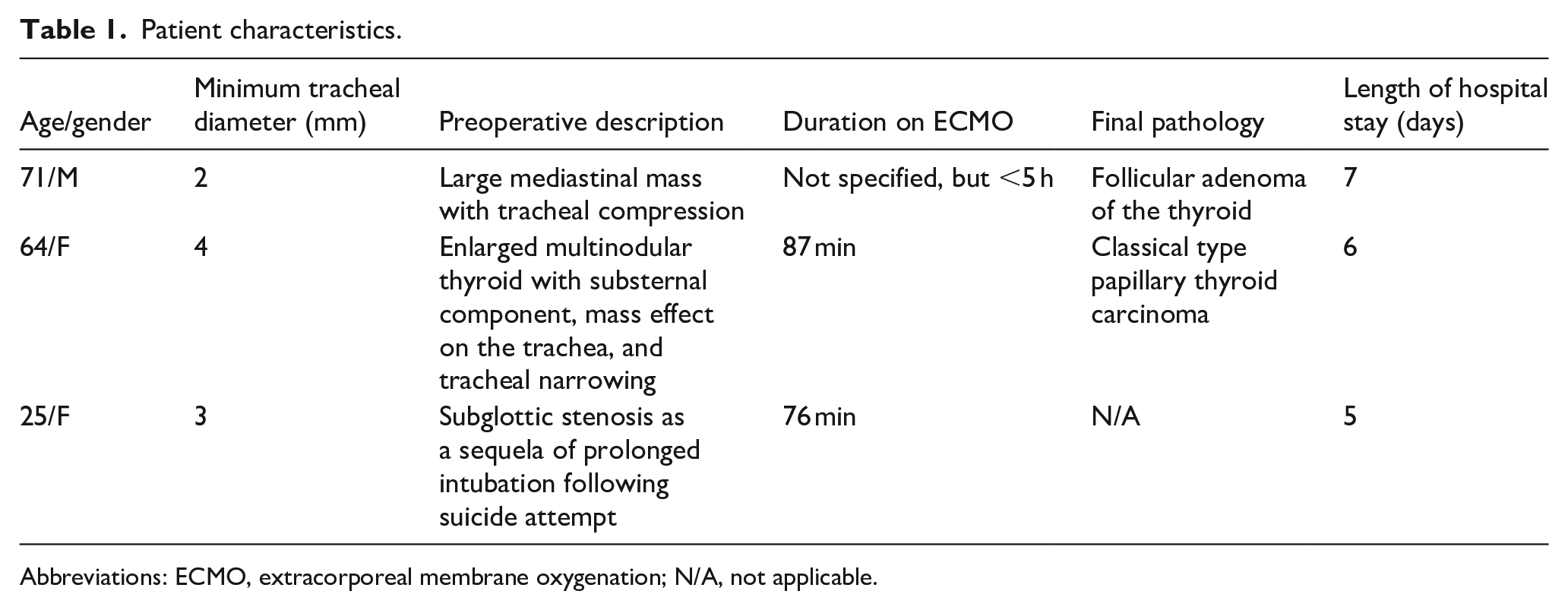
Abbreviations: ECMO, extracorporeal membrane oxygenation; N/A, not applicable.
Discussion and Literature Review
The first use of cardiopulmonary bypass (CPB) for airway surgery was reported by Woods et al., necessitated by unanticipated tumor extension from the carina into the trachea. 4 Subsequent CPB use in head and neck surgery was rare, mostly involving lung transplantation or acute respiratory distress syndrome.5,6 Coles et al. later described CPB-assisted anesthesia induction in 1976 for a patient with a large tracheal tumor that precluded intubation. 7
Walker et al. first reported using peripheral ECMO for airway surgery in 1992 for an infant who underwent tracheal resection for congenital airway stenosis. 8 ECMO was preferred over traditional CPB as it avoided a median sternotomy and required far less heparin. The success of this case encouraged broader ECMO use for complex intubation and anesthetic management in both adult and pediatric patients.9 -18
More recently, Chakalov et al. described using venovenous ECMO prior to general anesthesia in a patient with severe occlusion of the tracheal lumen, measuring less than 5 mm, at the level of the aortic arch. 19 The patient remained on ECMO for 19 hours. Karim et al. reported 4 similar cases where ECMO preceded intubation and was continued for at least 1 day postoperatively. 20
The use of ECMO in head and neck cases remains rare because typically, even when intubation is not possible, an airway can be established using conventional alternatives such as tracheostomy, jet ventilation, balloon dilation, or rigid bronchoscopy. Awake fiberoptic intubation is generally preferred for complex airways and has demonstrated safety and efficacy in both anticipated and unanticipated difficult intubations.21,22 However, in extreme cases where no feasible or safe alternatives exist—such as in our presented series, where the tracheal diameter was too narrow to permit passage of a fiberoptic scope—ECMO can serve as a bridge to secure the airway. In such scenarios, there is a critical concern that attempts at intubation or ventilation may fail entirely if the ETT cannot be advanced beyond the obstruction. While ventilation through a rigid bronchoscope can offer some capacity to manually bypass the narrowing, it carries similar risks if the obstruction cannot be traversed, potentially resulting in an inability to oxygenate or ventilate the patient adequately.
Additional consideration must be given to sedation prior to ECMO cannulation, as even mild sedation can precipitate airway collapse in these patients. Prophylactic measures should be taken to minimize airway compromise, and sedatives with minimal respiratory depression, such as dexmedetomidine, may be particularly useful in this setting. 23
Despite advances in the safety of ECMO over the past several decades, it still poses risks including bleeding and infection. 24 Thus, it is important to emphasize that this technique should only be considered in extremely-unusual or challenging airway situations. In all the above cases, the benefits of proceeding with ECMO outweighed the risks.
This study has some limitations. As a retrospective review of a surgical technique, there is no feasible way to provide control cases. Additionally, some patient data were incomplete, such as the precise duration that the patient in case 1 was placed on ECMO. Despite these limitations, this case series supports the safety and efficacy of using ECMO for the induction of anesthesia and intubation in complex airway operations.
Conclusion
ECMO has emerged as a safe technique of providing oxygenation without intubation in a variety of head and neck cases over the past decade, particularly in cases where a failed intubation attempt could prove disastrous. We present 3 cases in which ECMO was successfully used to permit anesthesia prior to intubation. Notably, each patient was weaned from ECMO intraoperatively after securing the airway, minimizing CPB duration and potentially reducing its associated risks.
Footnotes
Ethical Considerations
Approval was obtained from the Institutional Review Board of Mayo Clinic Hospital in Phoenix, Arizona. All patient information is de-identified, and as a retrospective study, individual patient consent was not required.
Consent to Participate
As a retrospective study, individual patient consent was not required. All information and photographs are fully de-identified.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data relevant to this study are presented in the manuscript. No additional data were utilized.