
Abstract
Middle ear trauma from foreign body (FB) impaction or its removal can lead to tympanic membrane (TM) perforations and ossicular chain disruption. We present a case of a 29 year-old male who developed acute right-sided hearing loss, aural fullness, and tinnitus after an attempt at removing a cotton-tipped applicator (Q-tip) impaction in the ear canal. Physical examination revealed a dislocated incus protruding through the TM, and audiometry confirmed moderate conductive hearing loss. The patient underwent tympanoplasty with ossicular chain reconstruction with incus interposition, which resulted in significant hearing improvement and resolution of tinnitus. This case highlights the importance of proper diagnosis and intervention in trauma-related ossicular dislocation.
Keywords
Introduction
Unfortunately, patients frequently present with self-inflicted middle ear trauma from foreign bodies, especially from cotton-tipped applicators (Q-tips). Studies have shown that Q-tips are a common cause of tympanic membrane (TM) perforations, especially in children.1,2 While these injuries often resolve spontaneously, they can lead to more severe complications, such as ossicular chain disruption, conductive hearing loss (CHL), vertigo, and facial nerve paralysis. 3 Delayed diagnosis or inadequate management may exacerbate these issues, with potential long-term auditory dysfunction. In cases of significant ossicular dislocation or fracture, surgical intervention may be required for optimal outcomes. 4
Ossicular injuries require prompt diagnosis due to their potential impact on hearing. 4 Studies indicate that ossicular dislocations, particularly incudomallear and incudostapedial, can occur after trauma, with hearing improvements following ossiculoplasty.5,6 We hereby present a case of ossicular dislocation, which occurred from an attempt at removal of a foreign body (FB) from the ear canal by an urgent care provider.
Case Presentation
A 29 year-old male presented to an urgent care with aural fullness, otalgia, and otorrhea, which occurred after using a cotton-tipped applicator. At the urgent care, the provider attempted to remove the FB with an alligator forceps, which caused acute pain, decreased hearing, and tinnitus. The patient subsequently presented to us for management. He denied any history of prior otologic surgeries.
On physical examination, the patient was noted to have a protrusion of the incus through the posterior superior quadrant of the right TM (Figure 1). Audiometry revealed moderate CHL on the right side (Figure 2A), with a flat tympanogram. A computed tomography (CT) scan of the temporal bone was obtained, which revealed a dislocated right incus with the long process protruding through the TM and the incus body positioned in the mesotympanum (Figure 3).
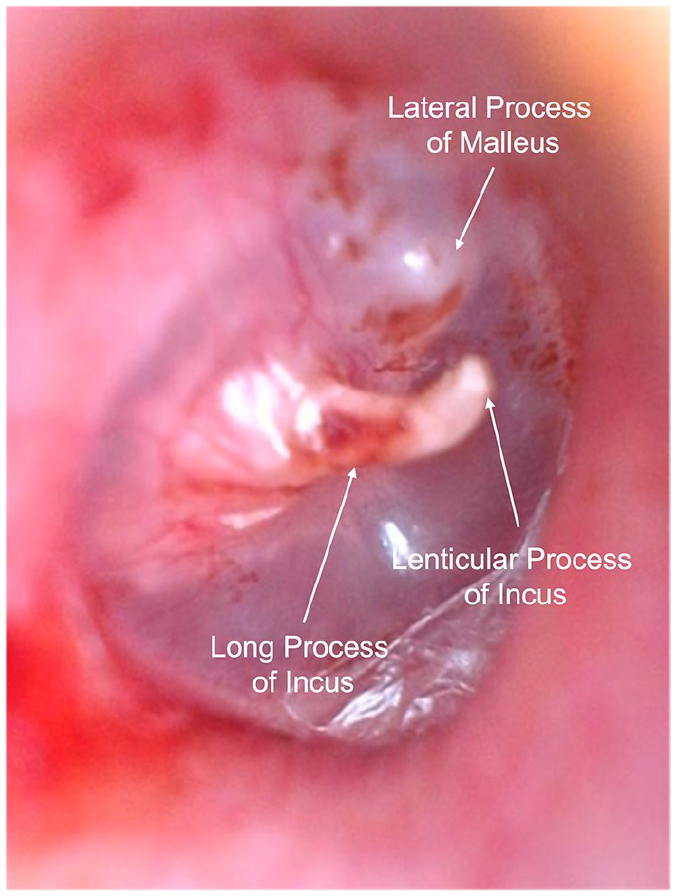
Otoscopic image of the patient’s TM showing the protrusion of the incus through the posterior superior quadrant of the TM. TM, tympanic membrane.
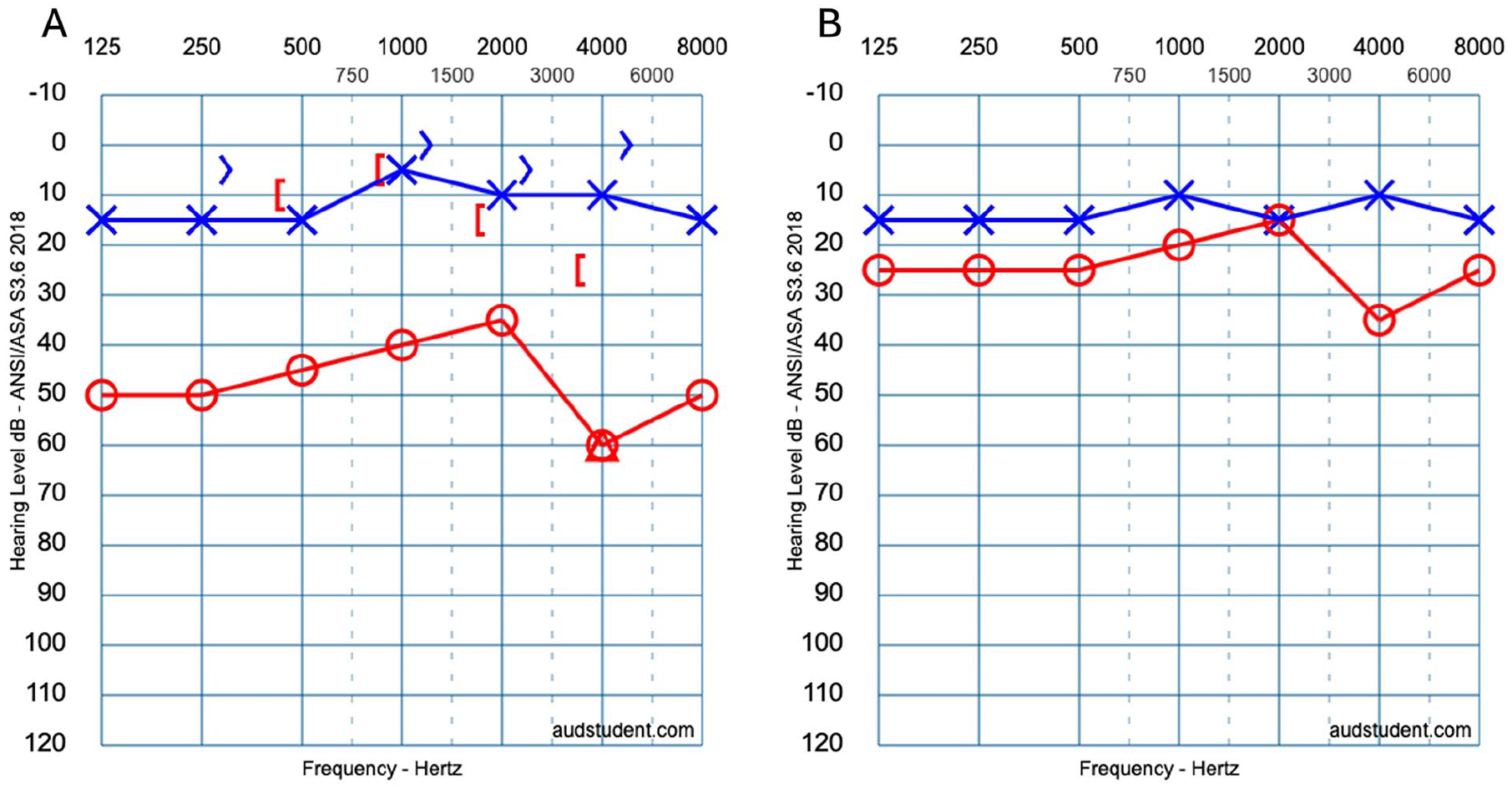
Audiometry pre-operatively and post-operatively Audiometry showing moderate CHL at the time of presentation (A), which was reversed postoperatively (B). CHL, conductive hearing loss.
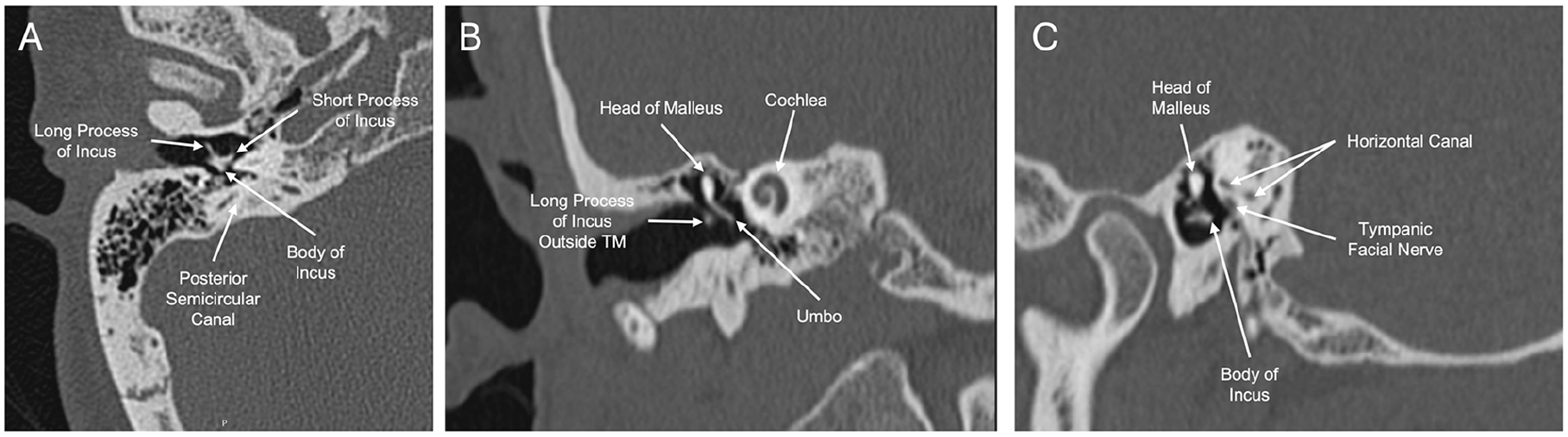
CT scan of the right temporal bone in the (A) axial plane, (B) coronal plane, and (C) sagittal plane.
Given these findings, a transcanal right tympanoplasty with ossicular chain reconstruction was performed. Intraoperatively, it was noted that the long process that was previously protruding through the TM had eroded away, and the TM had closed. The dislocated incus was successfully repositioned by placing the remnant of the long process onto the stapes capitulum and the body under the posterior superior TM with the short process pointing inferiorly. Postoperatively, the patient's hearing improved significantly, and his tinnitus resolved. He was followed up at the 6th month, with stable improved hearing (Figure 2B).
Discussion
To our knowledge, this is the first report of a dislocation of the incus from the attempted FB removal with alligator forceps. In our case, the perforation of the TM was not a direct consequence of Q-tip insertion but rather resulted from inadvertent trauma during an attempt at its removal. The urgent care provider advanced the instrument through the TM and grasped the incus. This event highlights the risks associated with inappropriate or overly-aggressive removal techniques, especially in cases where an impacted FB is near the TM, and instrumentation is carried out under otoscopy when no microscopy is available.7 –9
The external auditory canal (EAC) is the most common site for FB impactions, especially in children, with the most frequent FBs being beads, paper, tissue paper, and popcorn kernels. 10 Removal methods typically include irrigation, suction, or other instrumentation, often with the aid of an operating microscope. Approximately 75% of FBs can be removed in the outpatient setting. 10 The most common complications from FB removal are excoriations and lacerations of the EAC skin, while less frequent but more serious complications include TM perforation and ossicular damage. 10 The vulnerability of the ossicular chain to trauma is due to incus and stapes being within 2 to 4 mm of the TM, which highlights the need for delicate technique in removing FBs especially with alligator forceps under otoscopy. FB removal from the EAC is best performed under microscopy when it is available.
Audiometry can help the clinician understand the degree of disruption to the ossicular chain. A large CHL (>35 dB air bone gap) in the low frequencies indicates that a more significant disruption has occurred. A smaller gap may indicate a fracture or smaller degree of dislocation, which may improve with time and scarring potentially. Sensorineural hearing loss indicates a possible oval window fracture. Tympanometry can help in understanding the presence of a microperforation, which can be a clue that middle ear trauma may have occurred. Dizziness during tympanometry is a good fistula test, which can point to a stapes footplate fracture. In a patient presenting on an outpatient clinic setting with a deep FB in the EAC, if feasible, audiometry prior to removal can help gain a better understanding of the degree of problems caused by the FB.
The management of ossicular dislocations or fractures resulting from trauma during FB removal requires a careful approach. Surgical exploration of the middle ear is often required for the correction of dislocated ossicles, 5 and in some cases, ossicular chain reconstruction with a prosthesis may be needed to restore hearing. 11 Unlike temporal bone fracture-related CHL hearing loss, which often improves over the 6 month post-injury, significantly-dislocated ossicles benefit from early-surgical intervention. This is due to the mechanical disruption of the ossicular chain, which does not typically resolve spontaneously.
In temporal bone fractures, CHL is often caused by the separation of the incudomalleal joint. This CHL improves in the first 6 months post-trauma from scar formation in the joint and leads to improved motion of the chain. Other scarring around the ossicles also softens over 6 months leading to improved hearing. However, significantly-dislocated ossicles are best treated early. If there is evidence of stapes footplate fracture (sensorineural hearing loss, concomitant vertigo, or a positive fistula test), then urgent intervention is warranted to prevent permanent sensorineural hearing loss. If urgent intervention is not possible, a middle ear blood patch procedure (injecting 0.5 cc of blood in the middle ear) can be performed in the office setting to seal a perilymph fistula until surgical planning can be performed. 12 Mantokoudis et al. 13 found that deviations in the malleus-incus axis on CT scans were predictive of poor hearing outcomes, indicating preoperative imaging can help in predicting long term outcomes. Ossicular reconstruction can be performed microscopically or endoscopically. 14 Due to normal Eustachian tube function in the posttraumatic ossicular dislocation, reconstruction procedures tend to have better outcomes than patients with cholesteatoma-related ossicular disruption in our experience.
Conclusion
This case highlights the danger of an untrained individual attempting to remove an ear canal FB and how the incus is vulnerable to dislocation due to its proximity to the TM. Surgical management of this type of trauma can be performed with a partial ossicular reconstruction prosthesis or incus interposition. In this case, incus interposition led to a less than 10 dB air bone gap with sustained improvement.
Footnotes
Acknowledgements
Not applicable.
Ethical Considerations
Ethics approval was not required for this case report. The patient was treated as part of routine clinical care, and no experimental interventions were performed.
Consent to Participate
Written informed consent to participate in this case report was obtained from the patient.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Hamid R. Djalilian is an advisor and holds equity in NeuroMedCare LLC, Elinava Technologies, and Cactus Medical LLC.
Data Availability Statements
Data sharing does not apply to this article as no datasets were generated or analyzed during the current study.