
Abstract
Background:
Orbital complications of acute pediatric rhinosinusitis, such as subperiosteal and orbital abscess, meningitis, and intracranial extension, represent time-sensitive conditions requiring prompt diagnosis and management. Improved understanding of the anatomic, microbiologic, and clinical factors contributing to these complications is essential for optimizing outcomes.
Methods:
This review synthesizes current literature on the diagnosis and management of orbital complications in pediatric acute sinusitis, with emphasis on risk stratification, imaging indications, and surgical decision-making. Two representative case studies are included to illustrate diagnostic and therapeutic considerations.
Results:
While pediatric patients may improve with medical therapy alone, abscess formation or progressive complications despite antibiotics often necessitate surgical intervention. Clinical presentation, ophthalmologic examination findings, and abscess characteristics are critical in risk stratification and determinants for surgical management.
Conclusion:
A high likelihood of suspicion of an underlying sinus disease is warranted when evaluating children with periorbital redness and swelling. Monitoring and further evaluation with imaging are critical to prevent acute rhinosinusitis with orbital complications and vision-threatening sequelae.
Introduction
Acute sinusitis is defined by symptoms lasting between 10 days and 12 weeks or by an acutely complicated clinical course, such as concomitant orbital abscess or meningitis. While viral upper respiratory infections are common in children, occurring 6 to 8 times annually, only 0.5% to 5% progress to acute bacterial sinusitis. 1 Still, sinusitis accounts for nearly 6 million visits to a pediatrician annually. 2 Orbital complications, which comprise 74% to 85% of all acute sinusitis complications, are disproportionately seen in pediatric patients, reflecting the population’s thinner bony barriers and evolving sinus anatomy. 3 Thus, the clinical course of pediatric rhinosinusitis is distinct from adults due to both anatomic immaturity and age-specific risk factors, such as frequent viral infections and immunologic immaturity.
Pathogenesis and Predisposing Factors
The primary pathophysiologic mechanism in sinusitis is obstruction of the sinus ostia, most commonly at the osteomeatal complex (OMC), due to mechanical obstruction or mucosal inflammation and edema. OMC obstruction impairs mucociliary clearance, leading to retained secretions, hypoxia of the sinus mucosa, and ciliary dysfunction, which, in turn, predispose patients to secondary bacterial infection. Orbital complications typically arise from ethmoid involvement, given the thin lamina papyracea, though imaging may reveal extension from other sinuses or bilateral disease.
An additional pathogenic mechanism involves bacterial exotoxins and the formation of biofilms, which contribute to a symptomatic immune response and reduced antibiotic efficacy. Wang et al demonstrated that staphylococcal superantigens can activate T cells and contribute to chronic inflammation in patients with nasal polyps. 4 Sanclement et al identified biofilms in the sinus mucosa of 80% of patients undergoing functional endoscopic sinus surgery (FESS), in contrast to their absence in healthy controls. 5 Additional studies confirmed the presence of biofilms in the adenoidal tissue of children with chronic upper airway infections and chronic rhinosinusitis. 6 These findings suggest that exotoxins and biofilms play a significant role in the pathogenesis and persistence of bacterial sinus infections in pediatric patients.5,6
Beyond local obstruction and infection, pediatric sinusitis may arise from mechanical obstruction of the concha bullosa or systemic factors such as primary ciliary dyskinesia. Specifically, congenital anomalies or dehiscence of the bony orbital wall may predispose individuals to orbital complications. 7 Gastroesophageal reflux disease (GERD) in particular, as an inflammatory contributing factor, is prevalent among children with chronic rhinosinusitis.8,9 In a retrospective study, Bothwell et al demonstrated a significant decrease in the need for sinus surgery among children on anti-reflux therapy. 8 These findings support a broader diagnostic framework required when assessing persistent symptoms and surgical candidacy in pediatric rhinosinusitis patients.
Microbiology of Acute Sinusitis
While the bacterial pathogens Streptococcus pneumoniae, Moraxella catarralis, and nontypeable Hemophilus influenzae remain the primary targets of empiric antibiotic therapy in acute bacterial rhinosinusitis, emerging research suggests a more nuanced microbial landscape. 10 Recent studies challenge the longstanding view of sterile paranasal sinuses, and instead identify a resident sinus microbiota with potential protective roles. 11 Abreu et al described a reduced diversity of sinus microbes in patients with sinusitis in comparison to healthy controls, with notable depletion of Lactobacillus sakei, a species hypothesized to exert colonization resitance. 11 Such studies probe the possibility of whether microbiome disruption, due to broad-spectrum antibiotics or frequent upper respiratory tract infections, contributes to pathogenesis or recurrence in pediatric patients. Such data underscore the potential need to balance antimicrobial therapy with preservation of microbial homeostasis in recurrent or refractory cases.
Streptococcus species remain the predominant pathogens in pediatric orbital cellulitis and cases complicated by subperiosteal abscess. 12 The incidence of S. pneumoniae and H. influenzae has declined following widespread implementation of the pneumococcal conjugate vaccine and Hib vaccine.10,12 Nevertheless, recent series continue to report S. pneumoniae and Staphylococcus aureus as leading isolates in sinusitis-associated subperiosteal abscess, particularly in children under 7 years of age. 13 Furthermore, Streptococcus anginosus, a member of the Streptococcus milleri group, has emerged as an increasingly prevalent organism.10,13,14 These shifts in microbial patterns likely reflect a combination of changing vaccination coverage and host immune maturation.12,15,16 As such, empiric antibiotic selection for orbital complications must continue to account for evolving pathogen profiles, including coverage for anaerobic species.
Salonna et al proposed that indirect effects of the COVID-19 pandemic contributed to a rise in orbital complications of acute rhinosinusitis among pediatric patients. 17 Comparing cohorts from 2018 to 2020 and 2021 to 2023, they observed an increased incidence of complicated acute rhinosinusitis in patients aged 9 to 16 years, consistent with findings from other groups.17,18 Streptococcus species remained the predominant pathogens in both periods; however, the post-pandemic cohort uniquely exhibited less commonly implicated organisms such as Enterobacter, Klebsiella, Coxiella, and Aspergillus. 17 These findings raise the possibility that pandemic-related restrictions, such as reduced environmental antigen exposure, may have altered normal immune maturation and disrupted the sinus microbiome, predisposing patients to more severe or atypical infections. This evolving microbial landscape highlights the need for continued surveillance and reinforces the role of the sinus microbiome in mucosal defense.
Diagnosis
While anterior rhinoscopy informs nonspecific inflammation (Figure 1), fiberoptic sinonasal endoscopy facilitates the identification of purulence drainage at the middle meatus, indicating anterior ethmoid or maxillary involvement. These observations can help guide decisions for patient workup. In younger children, the predominance of ethmoiditis as the source of orbital complications reflects not only the underdevelopment of other sinuses but also the intimate anatomical and venous continuity between the orbit, ethmoidal, and paranasal sinus.7,19,20 This emphasizes the need for a low threshold to escalate care in pediatric patients with early orbital symptoms, even in the absence of overt systemic signs.
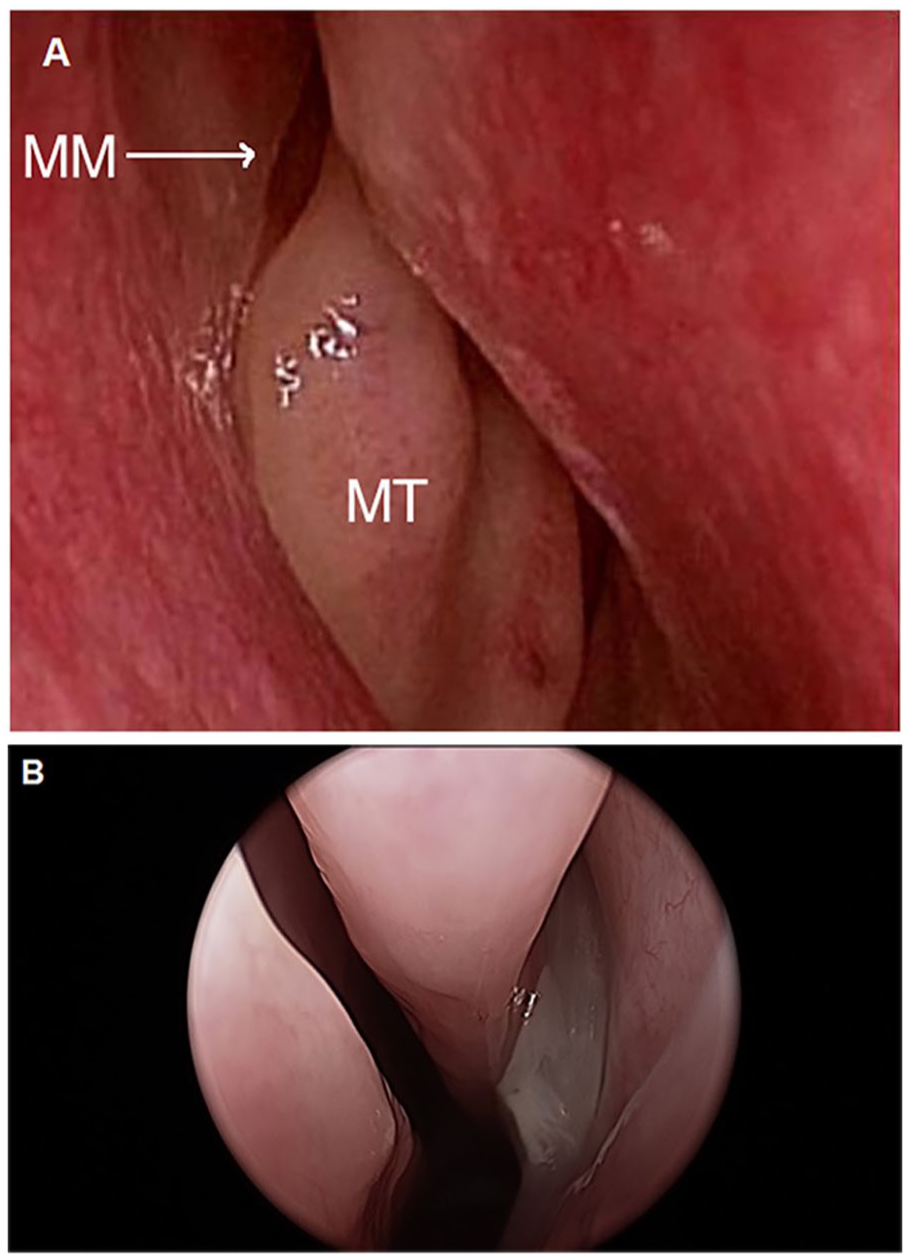
(A) Normal anterior rhinoscopy with a view of the MT and MM. (B) Anterior rhinoscopy demonstrating purulent drainage from the middle meatus. MT, middle turbinate; MM, middle meatus.
Several studies have investigated the utility of clinical and laboratory findings during the initial 24 hours of presentation to predict orbital complications.19 -21 Yosefof et al demonstrated that proptosis, ophthalmoplegia, and an absolute neutrophil count (ANC) >10 000 correlated with the presence of a subperiosteal abscess on computed tomography (CT). 21 Notably, these clinical and laboratory findings were observed in both early and late scans, with earlier scans not associated with an increased rate of surgical interventions. 21 However, few studies provide consistent cutoff values for laboratory findings, limiting their utility in accurately assessing the severity of orbital complications and guiding management decisions in the absence of imaging. Consequently, radiologic imaging remains essential when clinical suspicion is high.
Radiologic evaluation of children with sinusitis is usually reserved for cases of persistent or recurrent symptoms unresponsive to medical therapy or when complications are suspected. Although plain films have largely fallen out of favor due to limited sensitivity and anatomic overlap, recent emphasis on radiation stewardship has prompted some clinicians to defer imaging. CT remains the gold standard for delineating sinus anatomy and orbital or intracranial extension (Figure 2); however, recent literature has supported restraint in the use of CT scanning in children due to concerns of excess radiation exposure.22,23 While some studies advocate reserving CT imaging for medically refractory orbital cellulitis or when operative intervention is being considered, the presence of early orbital findings or neurologic symptoms typically justifies prompt imaging to define the extent of disease. 24 The American Academy of Pediatrics and the American College of Radiology both endorse contrast-enhanced CT or MRI as appropriate modalities when orbital or intracranial complications are suspected, though MRI may offer superior soft tissue detail in select cases. 25 In practice, CT remains the more accessible and time-efficient option in acute settings.
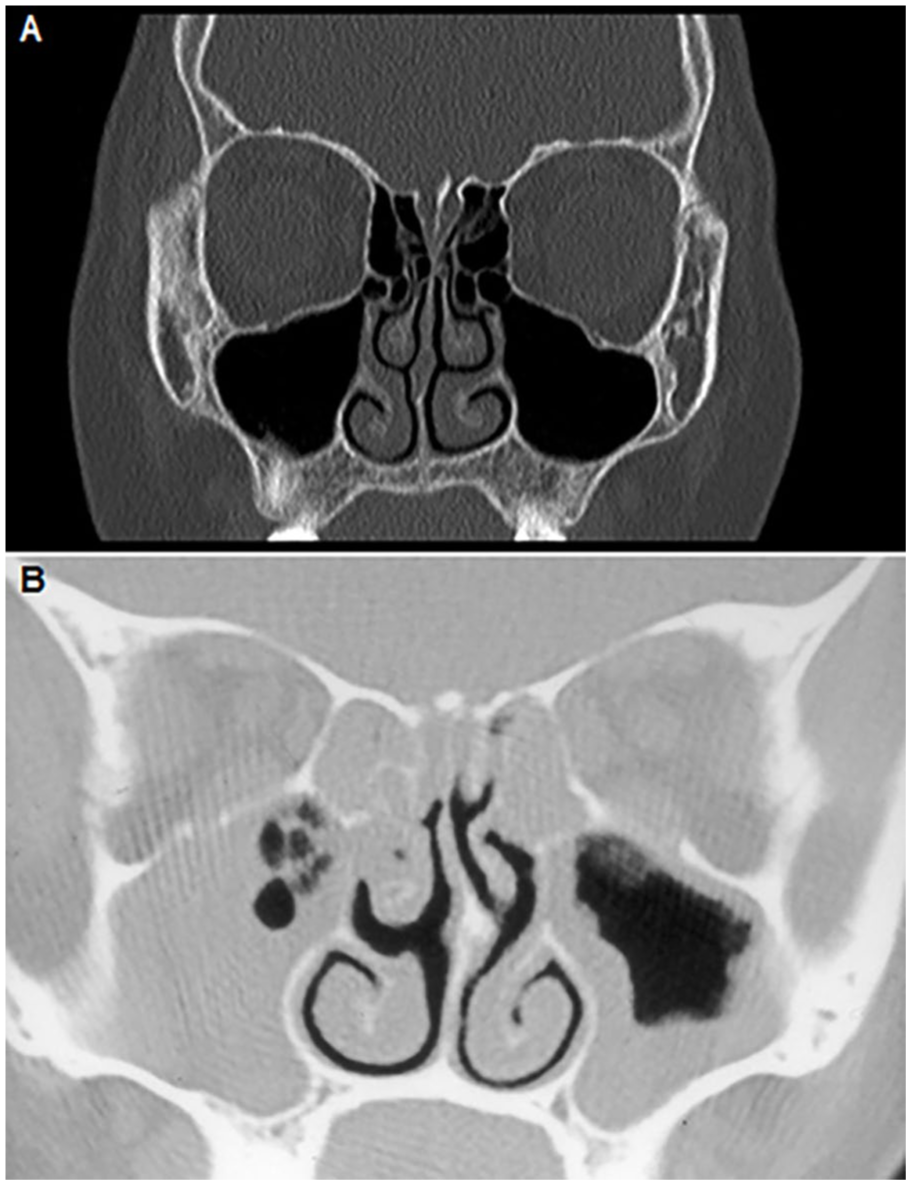
(A) A normal coronal CT scan of the sinuses. (B) A coronal CT scan of the sinuses demonstrates bilateral ethmoid sinus opacification, maxillary sinusitis on the right, and mucosal thickening within the maxillary sinus on the left. CT, computed tomography.
To minimize unnecessary radiation exposure, a conservative diagnostic approach may involve using MRI as the initial imaging modality for orbital complication identification, followed by CT, reserved for cases requiring preoperative evaluation and surgical planning.18,21 CT remains essential when surgical intervention is anticipated, particularly when image-guided intraoperative navigation is utilized in pediatric sinus surgery. However, limitations of MRI, such as availability, longer acquisition time, and frequent need for sedation in young children, may constrain its use as a sole alternative. Yosefof et al reported cases where initial CT imaging was non-diagnostic, leading to delayed surgery despite clinical deterioration, underscoring the importance of serial reassessment and a low threshold for repeat imaging. 21 This suggests that initial MRI combined with vigilant clinical observation may, in select cases, obviate the need for excessive CT imaging.
MRI with contrast is typically preferred for evaluating suspected intracranial extension due to its superior soft tissue differentiation and clear contrast resolution in the orbit.7,24 While contrast-enhanced, fat-suppressed T1-weighted imaging remains the gold standard for distinguishing abscess from inflammatory edema in the orbit, data on direct comparisons between CT and MRI for orbital infections are limited. 24 When contrast is contraindicated, diffusion-weighted imaging offers a reliable adjunct to conventional non-enhanced MRI, with increasing evidence supporting its utility in detecting both orbital cellulitis and abscess formation.26,27 These considerations highlight the importance of tailoring imaging modality and protocol to the suspected complication and patient contraindications to contrast agents.
Point-of-care ultrasound has been proposed as a supplementary tool in the evaluation of orbital complications, particularly in settings where rapid assessment is required. However, its utility remains limited by operator dependency, acoustic shadowing from adjacent bony structures, and insufficient validation in high-quality studies. 24 A systematic review by Anwar et al found no prospective observational studies or randomized trials assessing its diagnostic accuracy for orbital cellulitis or abscess, with existing data limited to small case series and retrospective analyses. 28 Given these limitations, ultrasound may have a role in preliminary ophthalmologic evaluation but may not currently replace cross-sectional imaging in the workup of suspected orbital complications of acute rhinosinusitis.
Cases
Case 1 – Chandler III
A 4-year-old boy presented to his pediatrician with a 2-day history of right eye swelling and conjunctival erythema. He was otherwise healthy. He was referred to a local emergency department, where he was treated with IV clindamycin and corticosteroids and then discharged home on oral clindamycin. Over the next day, his swelling worsened, and he developed pain with right eye movements. After referral to a tertiary center, he was admitted and treated with IV ceftriaxone and vancomycin. His clinical examination at that time demonstrated significant periorbital edema and chemosis (see Figure 3A). A CT scan of sinuses was obtained for further evaluation, demonstrating scattered bilateral sinus disease, opacification of the right ethmoid sinus, and a right-sided subperiosteal abscess (see Figure 3B). The decision was made to take this patient to surgery for right-sided FESS with right medial orbital wall decompression and endoscopic drainage of subperiosteal abscess. Cultures from the OR grew S. pneumoniae. The child’s condition improved rapidly following surgery, and he was able to be discharged home on oral antibiotics on postoperative day 2. On further follow-up, he made a complete recovery with no loss of vision and normal extraocular movement.
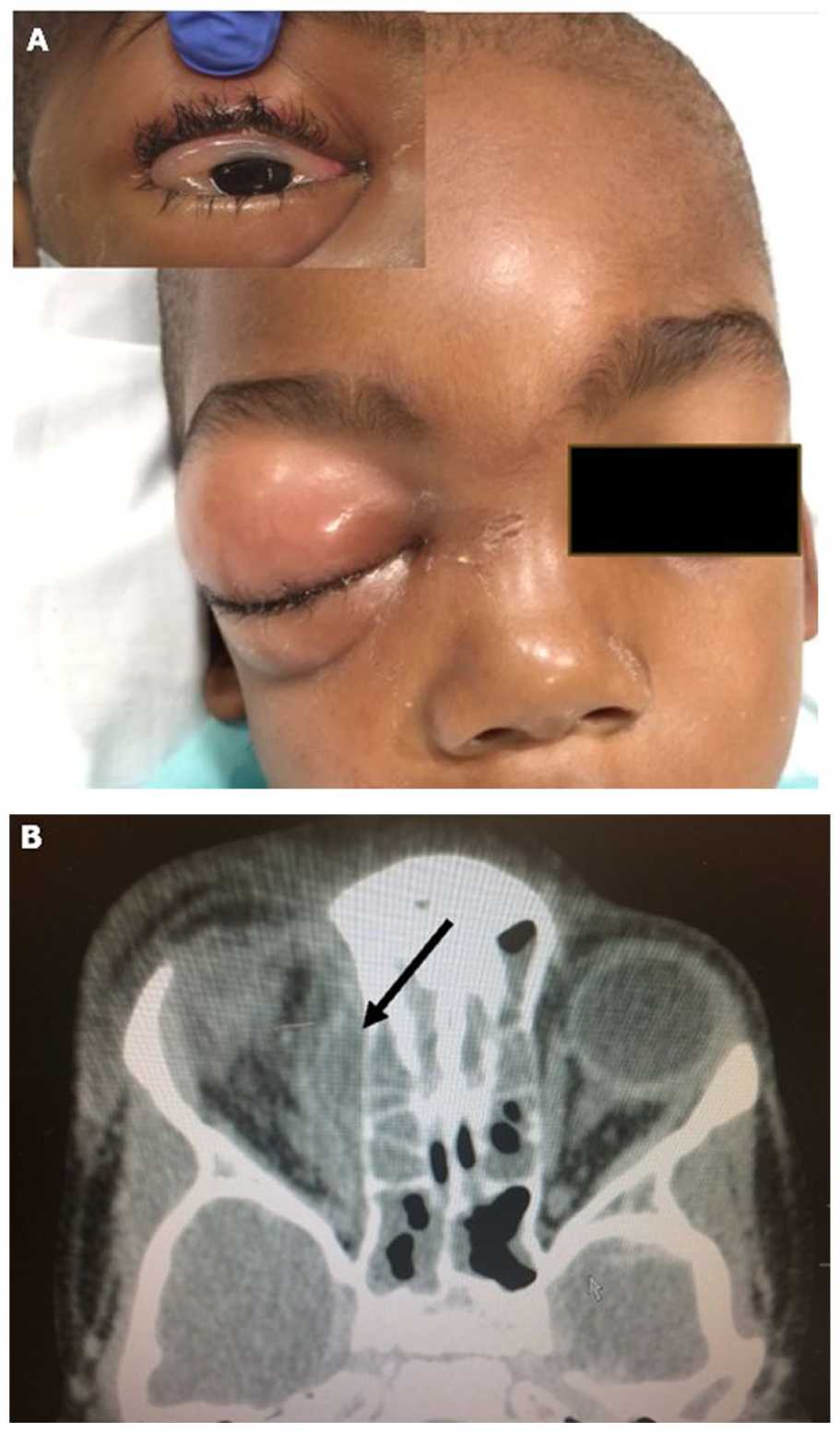
(A) A 5-year-old child with significant periorbital edema and erythema, as well as chemosis (subset), due to right-sided subperiosteal abscess. (B) Coronal CT scan of the sinuses from the same patient demonstrates scattered bilateral sinus disease, opacification of the right ethmoid sinus, and a right-sided subperiosteal abscess (arrow). CT, computed tomography.
This case demonstrates the combined medical and surgical approaches involved in the successful treatment of subperiosteal abscess (Chandler III) in children, as well as the finding of a typical bacterial pathogen. It highlights, as well, perhaps, the importance of vigilance and careful monitoring for potential complications of acute sinusitis, as the clinical condition can deteriorate rapidly. Although some studies simplify surgical decision-making algorithms by recommending medical management based on a Chandler stage I or II, this case and others demonstrate the importance of Chandler stage I, II, and III cases requiring close monitoring of symptom progression and frequent ophthalmologic evaluations.29,30 It seems reasonable to conclude that most children with even pre-septal cellulitis (Chandler I) should be hospitalized for close inpatient monitoring until their course of disease is clearly improving rather than worsening. Given the ophthalmic examination findings, this case also underscores the variability in what constitutes a concerning ophthalmic presentation. While the patient exhibited no signs of proptosis, the presence of pain with ocular movement still triggered high clinical suspicion. In addition, it emphasizes that although studies suggest children under 7 to 9 years of age often respond well to medical management alone, the presence of worsening symptoms irrespective of age may still necessitate imaging and surgical intervention.
Case 2 – Chandler IV
A 12-year-old girl was admitted to the hospital with significant periorbital edema associated with a recent upper respiratory infection, thought potentially complicated by acute sinusitis. She was intermittently febrile, and the examination demonstrated chemosis, proptosis, and limitation of extraocular movement on the right side. She reported both diplopia and ophthalmoplegia. She was otherwise healthy and without other past medical history. A CT scan of the sinuses revealed the presence of gas and orbital abscess formation within the right orbit as well as downward and lateral displacement of the globe (see Figure 4A). She was taken to surgery, where an open approach ethmoidectomy was performed and orbital abscess drained through a Lynch incision. Cultures from the operating room grew Streptococcus viridians. While the child’s overall condition improved, there was a subsequent breakdown of skin with loss of soft tissue of her upper eyelid as a result of the infection (see Figure 4B). Management of this wound required wet-to-dry packing until healed. While she had no permanent loss of vision, there was some significant scar formation with asymmetry of the right upper lid and periorbita. A referral was made to the oculoplastic team for evaluation and management of this soft tissue complication going forward.
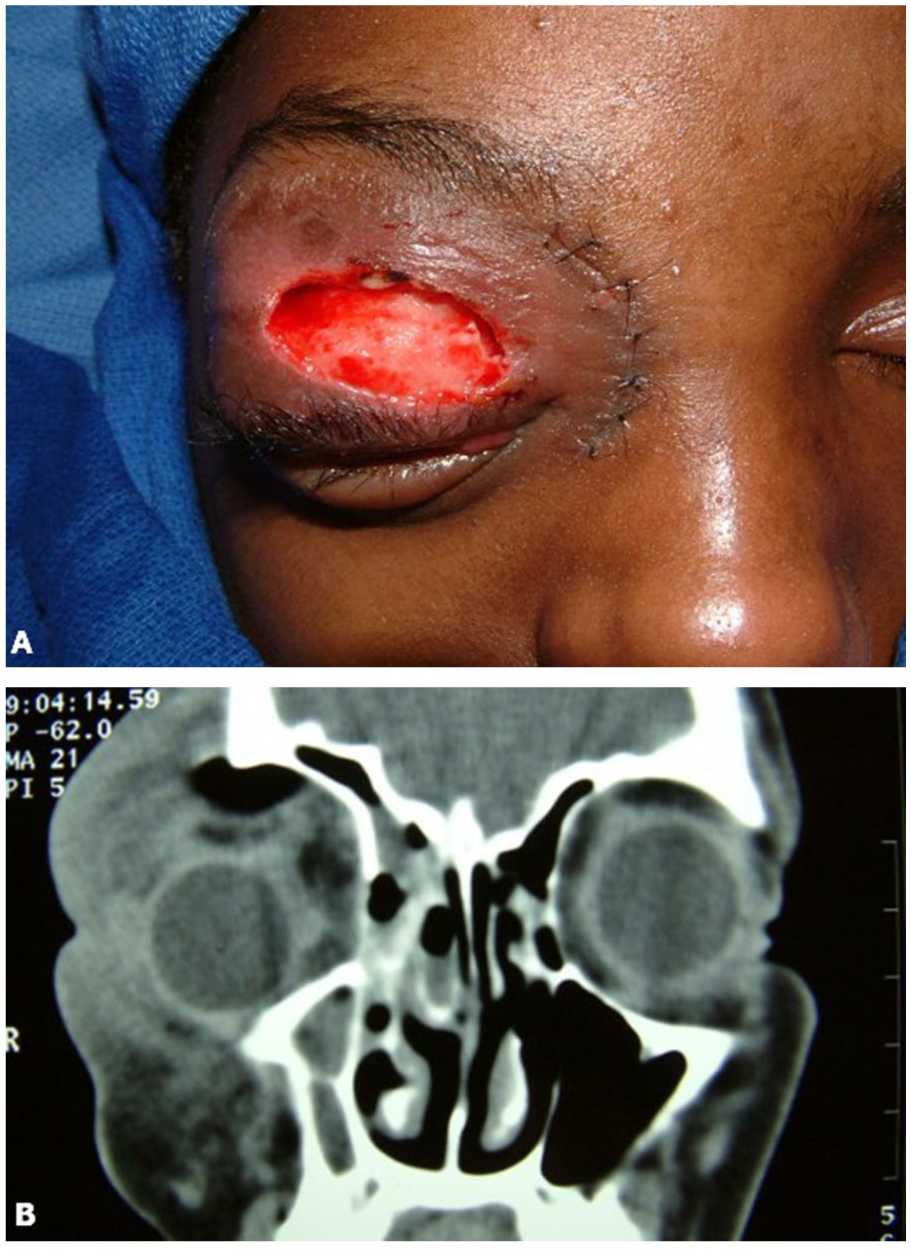
(A) A 12-year-old child with significant periorbital edema and loss of soft tissue due to right-sided orbital abscess. (B) Coronal CT scan of the sinuses from the same patient demonstrates the presence of gas and orbital abscess formation within the right orbit as well as downward and lateral displacement of the globe. CT, computed tomography.
This case demonstrates the potential severity of orbital infection as a complication of ethmoid sinusitis. In this case, an orbital abscess (Chandler IV) was further complicated by the breakdown of periorbital skin and soft tissue, leading to subsequent scarring and disfigurement. In alignment with current literature, the patient presented with alarming ophthalmic symptoms that warranted CT imaging and ultimately led to surgical intervention. The patient’s age also aligns with findings that suggest orbital complications are more severe in older children. The clinical course here further demonstrates the potential for open surgery as an option for adequate drainage of infection. This can be a useful option if significant edema and inflammation within the nasal cavity and sinuses preclude an endonasal approach with adequate visualization. Still, with current equipment and technology, most such cases are likely to be successfully managed with endoscopic sinus surgery techniques.
Discussion
The spectrum of orbital complications of acute sinusitis is commonly described by the Chandler criteria published in 1970.31,32 Chandler Group I represents preseptal cellulitis with edema and inflammation anterior to the orbital septum, as well as obstruction of venous channels. Generally, there is no associated loss of vision, and patients can be treated with antibiotics, steroids, and nasal decongestants. Group II indicates a progression to orbital cellulitis with increased edema on examination and the development of chemosis, proptosis, and ophthalmoplegia. While no abscess has yet formed, this infection has spread deep to the orbital septum. Although there is no visual loss, limitations in extraocular movements and pain may be noted. Group III disease is characterized by the formation of a subperiosteal abscess and has traditionally been the point at which surgery is considered for drainage. The abscess forms between the periosteum and bone of the medial orbital wall. Orbital cellulitis is also present, with erythema and an eye that is swollen shut on examination. The globe may be displaced laterally and/or downward. Subperiosteal abscesses account for 9% to 28% of orbital complications of sinusitis. 15 Group IV represents the formation of an orbital abscess with severe proptosis and chemosis. Ophthalmoplegia is present at this stage as well, and visual loss can result at a rate of 13% due to ischemia or neuritis of the optic nerve. Group V of the Chandler criteria indicates a significant spread of infection with bilateral ocular involvement. This state should also be suspected when clinical orbital findings are on the opposite side of unilateral sinus disease on CT scan or other imaging. The concern at this point is the development of cavernous sinus thrombosis, characterized by high fevers, severe headache, and photophobia. Proptosis and vision loss are characteristic at this stage. Cranial nerves II, III, IV, V1, V2, and VI may be impacted. Signs and symptoms of meningitis may be seen. Further progression may lead to intracranial complications such as subdural abscess, brain abscess, and death. The rate of mortality associated with cavernous sinus thrombosis is ~10%. 33
The Chandler system, while historically foundational, includes both pre-septal disease and advanced complications and thus spans a wide clinical spectrum. The Maloney modification refines this by explicitly distinguishing pre-septal from post-septal involvement based on septal penetration.31,32 Mortimore and Wormald 34 later proposed a simplified system focused on the prognostic relevance of abscess formation, subdividing post-septal disease into orbital cellulitis and abscess.35,36 Velasco e Cruz et al 37 further refined this approach by excluding pre-septal cellulitis altogether and categorizing disease into orbital cellulitis, subperiosteal abscess, and orbital abscess.35,38 While no single system has been universally adopted, understanding these frameworks supports more nuanced triage and management decisions.
Currently, there are no published guidelines from the American Academy of Otolaryngology-Head and Neck Surgery or the American Academy of Ophthalmology (AAO) for the management of pediatric orbital complications of acute sinusitis. Historically, due to the threat of vision loss and rapid progression of symptoms, the standard treatment for CT-diagnosed cases of subperiosteal abscess was surgical drainage. 16 However, since 2010, a trend toward more conservative, antibiotic-focused management has emerged, reflecting advances in antimicrobial therapy and earlier diagnosis. 39 Despite this shift, reported surgical intervention rates vary widely across studies, ranging from ~45% to over 70%, underscoring substantial practice variability.12,16 Notably in one study, a significant proportion of patients received antibiotics prior to hospitalization, yet many still required surgical drainage to prevent or address complications. 36 These discrepancies highlight the ongoing challenge of accurately identifying which patients will benefit most from conservative therapy versus early surgical intervention. This is a clinical decision that currently remains reliant on individualized assessment rather than standardized protocols.
Management of preseptal and orbital cellulitis secondary to acute sinusitis typically involves intravenous broad-spectrum antibiotics, including ceftriaxone, to address potential intracranial extension. Adjunctive topical oxymetazoline may facilitate mucosal edema reduction, while corticosteroid use remains controversial; meta-analytic data indicate steroids do not reduce surgical intervention rates but may shorten hospitalization duration. 16
However, despite agreement on antibiotic administration, uncertainty in guidance remains on whether a CT scan or surgical intervention is still warranted. For patients with Chandler criteria IV or V infection, surgery is generally indicated along with IV antibiotic therapy and, in some cases, anticoagulants for suspected cavernous sinus thrombosis. Treatment at this stage is often a multidisciplinary effort with ICU-level observation and monitoring. But in cases of subperiosteal abscess (Chandler III), it can be less clear whether surgical intervention is indicated.
Several studies have proposed comprehensive algorithms for management, identifying key factors, such as clinical presentation, ophthalmologic examination findings, and abscess characteristics. Generally, patients older than 9 years of age or those who show no clinical improvement after 48 hours of antibiotics, irrespective of age, are more likely to require surgery.15,19,40 However, high clinical suspicion should still be maintained for younger children, as Herrmann and Forsen reported a 9.3% risk of orbital and intracranial complications in children ≥7 years of age. 38 This is where the ophthalmologic examination remains pivotal in triaging urgency. Strong indicators for prompt imaging and possible surgical intervention, in addition to antibiotics, include proptosis exceeding 2 mm, decreased visual acuity, or the presence of relative afferent pupillary defect (RAPD), ophthalmoplegia, and elevated intraocular pressure.15,19,30,40 Notably, RAPD is particularly sensitive when assessing visual acuity, and gaze restriction is challenging. Abscesses that exceed 0.5 mL in volume, measure more than 4 mm in width, or are located non medially have a higher likelihood of requiring surgery.15,39,40,41,42 Medial subperiosteal abscesses have also been shown to respond more effectively to medical management, whereas superiorly located subperiosteal abscesses correlate with increased surgical intervention rates.40,43
Whether clinical factors such as high fever, elevated WBC, C-reactive protein (CRP), or ANC play a predictive role in surgical needs remains debated. Martin et al found no significant association between these laboratory markers and the need for surgery, and no correlation between these markers and the severity of CT findings.19,43 However, elevated WBC, ANC, and CRP levels have been observed more frequently in patients diagnosed with subperiosteal abscesses. 43 Yosefof et al suggest that WBC, CRP, and ANC may serve as early indicators warranting further evaluation. 21 Thus, while laboratory values alone should not dictate surgical management deferral, they can serve as adjuncts to ophthalmologic examination findings and support decisions to pursue early imaging. 42
Clinical deterioration and concerning findings on ophthalmologic examination remain the primary indicators for surgical management and, consequently, the initial decision to obtain imaging. The presence of air bubbles on imaging within the subperiosteal space, in addition to elevated CRP levels, may further support the diagnosis of abscess formation and the need for surgery. 19 In 2009, AAO published a systematic approach for determining the need for surgical treatment of subperiosteal abscess of the orbit based on clinical examinations, imaging, and consideration of patient age, and likely bacteriologic cause. 44
Given these indications, surgery is considered to help speed recovery and avoid further complications. In the past, drainage of such an abscess was performed, along with ethmoidectomy via an open approach such as a Lynch incision. However, as endoscopic equipment has improved and experience accumulated over the years, this is most commonly done currently via an endonasal approach. It would also be recommended, especially in children, to use intraoperative CT image guidance both for the localization of disease as well as the protection of normal structures as a part of this procedure. In addition, existing literature supports surgical management for superior subperiosteal abscesses. 40 More specifically, while FESS alone may be appropriate for medial subperiosteal abscesses, combined FESS and external drainage may reduce the risk of re-accumulation in superior subperiosteal abscesses. 40
Current literature, including several systematic reviews, is limited by sample sizes, heterogeneous study designs, and inconsistent reporting of clinical and laboratory thresholds.29,39,41,43 These factors constrain the ability to define high-grade evidence for specific decision points, such as ophthalmologic or inflammatory marker cutoffs. As management trends continue to favor initial medical therapy, there is a growing need to clarify the determinants of successful nonsurgical outcomes, particularly with respect to antibiotic selection, duration, and resistance patterns. Future research should prioritize large, prospective case series with standardized criteria, enabling the development of evidence-based treatment algorithms. In addition, further investigation into recurrence rates and the impact of antimicrobial resistance may also refine indications for nonsurgical versus surgical treatment strategies. 43
Conclusion
The successful diagnosis and treatment of orbital complications of acute sinusitis, such as subperiosteal abscess and orbital abscess, requires experience and a high likelihood of suspicion when children present with periorbital redness and swelling. An understanding of an appropriate treatment approach is critical to the timely management of outcomes. While there are other possible causes of pre-septal cellulitis, such as insect bites or other soft tissue infections, it is critical to include underlying sinus disease as a differential. Close monitoring for the progression of disease is of utmost importance, generally in an inpatient setting, and any deterioration rather than improvement in physical findings should prompt further evaluation with imaging to rule out a complication of acute sinusitis.
Footnotes
Consent to Participate
Written informed consent was obtained from a legally authorized representative for anonymized patient information.
Author Contributions
Hannah G. Luk: formal analysis; writing – original draft preparation, writing – review and editing. Austin S. Rose: conceptualization, methodology, formal analysis, investigation; writing – original draft preparation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article, as no datasets were generated or analyzed during the current study.