
Abstract
Objective:
To explore the effectiveness of surgical intervention in treating refractory rhinitis medicamentosa (RM) and determine whether laser posterior nasal neurolysis improves outcomes.
Method:
This is a retrospective cohort study from February 2023 to June 2025, which enrolled patients with RM refractory to medical treatment who received either radiofrequency ablation turbinate reduction (RF) alone or combined RF ablation with laser posterior nasal nerve neurolysis (RPN3).
Results:
The study included 37 patients with refractory RM (RF group = 9, RPN3 group = 28). During the 12-month follow-up, 35 patients (94.6%) withdrew from nasal constrictors successfully. For the entire cohort, the baseline reflective total nasal symptom score was 6.6 ± 2.9, decreasing to 1.5 ± 2.1 during the 12-month follow-up (P < .001). The baseline nasal obstruction symptom evaluation score was 13.3 ± 4.7, decreasing to 1.6 ± 2.7 during the 12-month follow-up (P < .001). The RF group showed significant improvement in congestion (P-value < .001), rhinorrhea, and sneezing (P-value < .05) but not in itching during the 12-month follow-up. The RPN3 group showed significant improvement in all subscores from the 1st to 12th month follow-up (P < .001).
Conclusions:
Surgical intervention successfully eliminated nasal decongestant dependency in patients with RM while improving their quality of life. The RPN3 procedure, which combines laser posterior nasal nerve treatment, may offer additional benefits by providing enhanced control of nasal itching and achieving earlier response in rhinorrhea and sneezing control.
Level of Evidence:
III
Introduction
Rhinitis medicamentosa (RM) is a drug-induced, nonallergic form of rhinitis, a condition characterized by rebound nasal congestion due to prolonged use of topical nasal decongestants. It typically results from excessive use of topical vasoconstrictors, such as oxymetazoline and phenylephrine. While these medications initially relieve nasal congestion, prolonged use causes a paradoxical worsening of symptoms upon discontinuation, creating a cycle of dependency.1-3 RM mainly occurs in young and middle-aged adults who have had access to over-the-counter vasoconstrictor nasal sprays and suffer from recurrent nasal obstruction. 2 Diagnosis primarily relies on the patient’s history and clinical presentation, including persistent nasal congestion, rhinorrhea, and nasal itching. In some cases, nasal endoscopy may be performed to assess the nasal mucosa condition and to rule out other causes of nasal obstruction, such as tumor or chronic rhinosinusitis. 4 RM is treatable, requiring patient cooperation and patience. Symptoms typically improve after discontinuing the offending medication, allowing the nasal function to normalize. Awareness of this condition is crucial for patients and health care providers to prevent unnecessary complications. 3 However, predisposing factors, such as allergic or parasympathetic-mediated rhinitis, which trigger the initial recurrent chronic rhinitis symptoms and lead to decongestant dependency, may remain uncontrolled. This leaves patients at risk of resuming nasal decongestant use.
Surgical intervention is considered when conservative treatments fail to relieve persistent nasal congestion caused by prolonged decongestant use. In a prospective study, Neiderman et al. 5 reported that all RM patients withdrew from nasal decongestants and experienced improved quality of life after inferior turbinate radiofrequency ablation (RFA). Margulis et al. 6 found that inferior turbinate reduction in RM reduced decongestant use and improved quality of life compared with medical treatment. Li et al. 7 reported that surgical treatment of medically-refractory RM led to 91.1% decongestant cessation and significant nasal symptom improvement, with a median follow-up of 3.4 (1.6-6.2) years. Thus, with careful patient selection, surgery may be an effective treatment for refractory RM.
Recent advances in posterior nasal nerve neurolysis (PNNN) offer effective alternatives for refractory rhinitis, focusing on rhinorrhea control rather than conventional septum and turbinate approaches. 8 Studies show that PNNN significantly reduces chronic rhinitis symptoms, with similar efficacy to allergic and nonallergic rhinitis, with patients experiencing improved nasal congestion, rhinorrhea, and sneezing for several months post-procedure. Recovery time is typically short, allowing patients to resume normal activities within 24 hours.9,10 PNNN has a favorable safety profile, with rare complications and minor postoperative discomfort being the most-commonly-reported issues. 11
To break the cycle of RM dependency, a combined approach addressing turbinate congestion and postsurgical chronic rhinitis symptoms may be considered. Our study hypothesized that by adding PNNN to RF turbinate reduction, post-operation parasympathetic-mediated rhinitis mechanism symptoms, including rhinorrhea, itching, and sneezing, could be obtained with more significant control. This study aimed to examine the safety and efficacy of the innovative RF turbinate reduction combined with laser PNNN (RPN3) surgical approach compared with RF turbinate reduction alone in managing RM unresponsive to conventional therapies.
Materials and Methods
Study Design and Patient Population
This retrospective cohort study evaluated patients with refractory RM seeking treatment for chronic rhinitis between February 2023 and June 2024, with the last patient follow-up until June 2025. The study was approved by the Ethics Committee of Chiayi Christian Hospital (No.: CYCH2024022; April 12, 2024). The institutional review board waived the need for informed consent due to the study’s retrospective nature.
Inclusion criteria were age 18 to 65 years and refractory RM resistant to medical treatment for >6 months. RM was diagnosed with dependency on a vasoconstrictor nasal spray, used daily for over 6 months to manage recurrent nasal obstruction, with no evidence of other nasal pathology. The medical treatment includes cessation of vasoconstrictor nasal spray use and prescription of intranasal corticosteroid with oral antihistamine. Failure of medical treatment was defined as continuation of vasoconstrictor use or persistent nasal congestion and/or rhinorrhea with quality of life impairment after 1 month of medical treatment, necessitating more advanced treatment despite medical treatment, and treatment with either RF turbinate reduction alone or RPN3. Ipratropium was not prescribed or tested due to lack of availability in the author’s practicing country. Exclusion criteria included prior nasal surgery, acute or chronic rhinosinusitis, and anatomic obstructions limiting RF or CO2 PNNN performance. Surgical options were discussed and determined by shared decision-making and endoscopy exam findings. Both surgical options were presented to the patients. Patients typically opt for the combined RPN3 procedure when experiencing more severe symptoms beyond nasal congestion, such as rhinorrhea, nasal itching, and sneezing (score ≧ 1 in each TNSS subscore). This choice is made despite the longer surgery duration and the potential for discomfort or complications, including epistaxis. Data collected included patients’ age, sex, smoking habits, obstructive sleep apnea history, mild-to-moderate deviated nasal septum, and preoperative and follow-up reflective total nasal symptom score (rTNSS) and nasal obstruction symptom evaluation (NOSE) scale scores. The use of steroid nasal sprays, antihistamines, and nasal irrigation was not restricted before surgery. No nasal spray or oral antihistamine was prescribed during follow-ups.
Procedure
All surgeries were performed by a single otolaryngologist (C-YH) under local anesthesia in the operating room. No septoplasty was performed. Preoperative anesthesia included bilateral inferior turbinate packing with a cotton strip soaked in 2% lidocaine and epinephrine (1:1000) and a 2% lidocaine injection into the bilateral inferior turbinate heads and lateral nasal walls to infiltrate the posterior nasal nerve distribution area.
RF turbinate reduction was performed using the CelonLab ENT (Celon AG Medical Instruments, Teltow, Germany). A disposable stylus delivered bipolar RF energy at 15 W to 15 to 30 nonoverlapping positions on the inferior turbinates, shrinking the turbinates and ablating intraturbinate neurovascular structures. The procedure took approximately 20 minutes for both sides.
RPN3 involved RF turbinate reduction followed by CO2 PNNN. PNNN was performed using a 2 W continuous wave AcuPulse™ CO₂ laser (Lumenis Ltd, Yokne’am Illit, Israel) transmitted via a nasal probe angulated at 20° with a straight-tip 90° mirror and smoke evacuation. The posterior middle meatus and superoposterior portion of the inferior turbinate were cauterized, targeting the posterior nasal nerve region. The procedure took approximately 3 to 4 min per side.
After RF or RPN3, the inferior turbinate was covered with Hemopatch (Baxter International, Deerfield, IL, USA), a 2 mm-thin sealing hemostat that absorbed tissue discharge within 1 to 2 days. No compression tamponade or nasal irrigation was required postoperatively. Patients received antihistamines, antibiotics, and analgesics for 3 days and were followed up at the 1st week, 4th week, every 3 months until the 12th month.
Surveys
Patients were evaluated using the 24 hour rTNSS and NOSE scale.12,13 The 24 hour rTNSS is a 4-item questionnaire scoring symptoms of nasal congestion, rhinorrhea, itching, and sneezing from 0 to 12. The NOSE scale is a 5-item questionnaire assessing nasal symptom-related quality of life, with scores ranging from 0 to 20. Postoperative complications were recorded at each follow-up visit.
Outcome Evaluation
The primary endpoint was the cessation rate of vasoconstrictor nasal sprays during the follow-up period. The secondary outcomes were interval change in rTNSS and NOSE scores, including individual item scores, during follow-ups. Treatment effects were assessed, and complications such as epistaxis, dry eyes, and headaches were documented.
Statistical Analysis
Continuous data are presented as mean ± standard deviation for normally-distributed variables and as median (interquartile range) for skewed data. Categorical data are reported as counts (percentages). Changes in survey scores from baseline were analyzed using 2-tailed paired t-tests for normally-distributed data and Wilcoxon signed-rank tests for skewed data. The chi-squared test for trend assessed severity-outcome correlations, with Fisher’s exact test used for sample sizes <5 per cell. Statistical analyses were performed using PASW Statistics (version 18.0.0; SPSS Inc, Chicago, IL, USA).
Result
A total of 46 patients were identified during the retrospective period, fulfilling the inclusion criteria. After exclusion from previous nasal surgery and combined septoplasty surgery, 37 patients were enrolled in our study cohort (Figure 1). Among these 37 participants, there were 9 patients receiving RF and 28 patients receiving RPN3. The baseline characteristics of the enrolled study cohort are presented in Table 1. The study population had a mean age of 38 ± 8.9 years and a mean body mass index (BMI) of 26.5 ± 4.5, with no significant differences between the RF group and the RPN3 group. Symptom scores, including rTNSS (mean 6.6 ± 2.9) and NOSE (mean 13.3 ± 4.7), showed no significant variations between groups. The prevalence of deviated nasal septum (27%), obstructive sleep apnea (27%), and cigarette, defined as current smoker before receiving the operation, use (18.9%) were similar across both groups, with all comparisons yielding no statistically-significant differences. These findings suggest that demographic and clinical characteristics were largely consistent across the study groups.
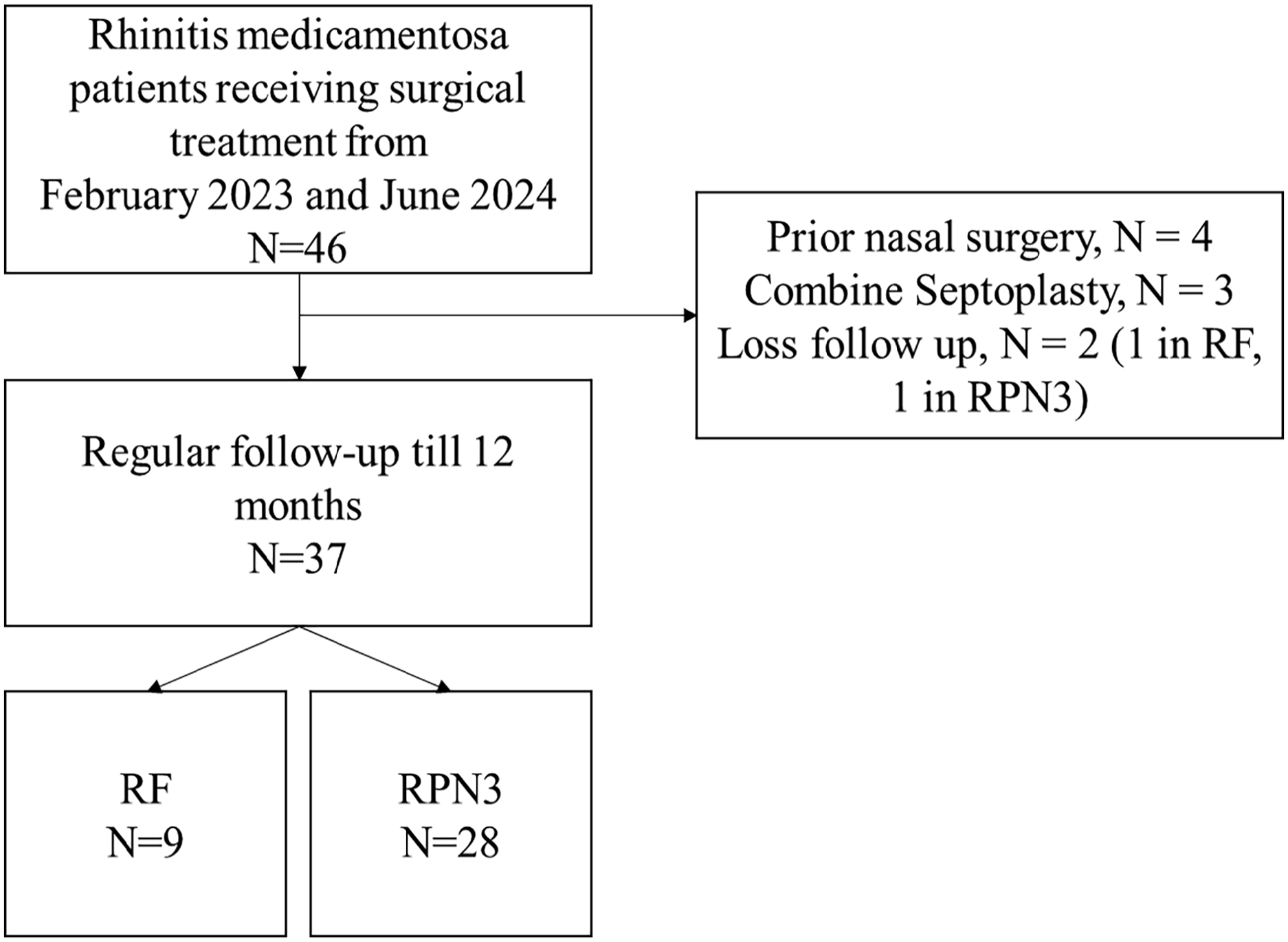
Patient disposition using a retrospective database. RF, radiofrequency ablation of inferior turbinates; RPN3, radiofrequency ablation of inferior turbinates with laser posterior nasal nerve neurolysis.
Characteristics of the Enrolled Patients With Refractory Rhinitis Medicamentosa.
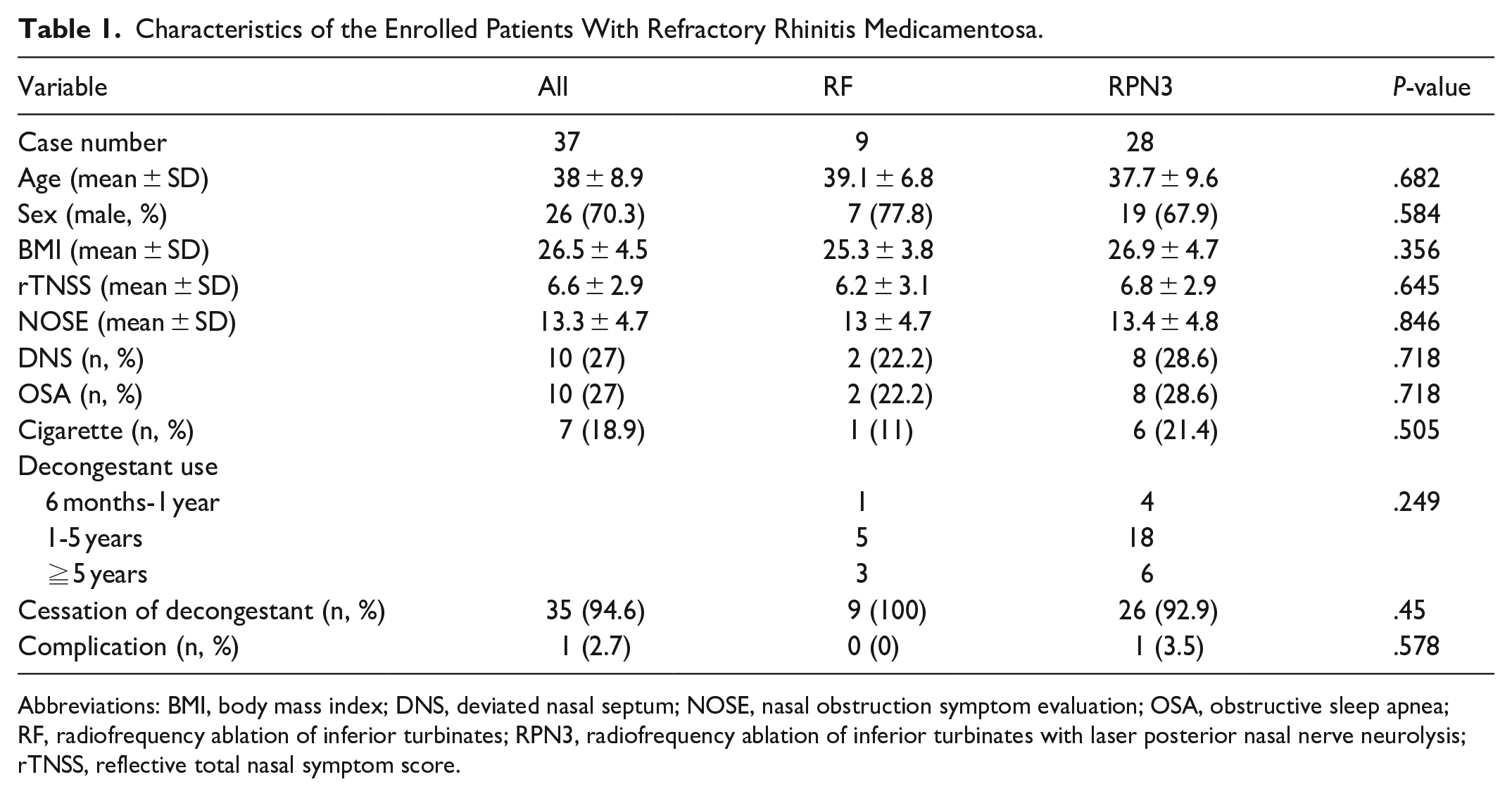
Abbreviations: BMI, body mass index; DNS, deviated nasal septum; NOSE, nasal obstruction symptom evaluation; OSA, obstructive sleep apnea; RF, radiofrequency ablation of inferior turbinates; RPN3, radiofrequency ablation of inferior turbinates with laser posterior nasal nerve neurolysis; rTNSS, reflective total nasal symptom score.
During the follow-up period, 35 out of 37 patients (94.6%) successfully discontinued decongestant nasal sprays with no difference between the RF and RPN3 groups. However, 2 patients in the RPN3 group resumed vasoconstrictor use within 12 months. The first case involved a 57-year-old male patient with RM and a caudal nasal septum deviation. He presented with an rTNSS score of 4 and a NOSE score of 15, along with a history of hypertension, coronary heart disease, and 5 coronary stents, requiring antiplatelet therapy. After holding antiplatelet medication for 1 week, he underwent RPN3 without complications or epistaxis. During the 3 month follow-up, he was free from decongestants and other rhinitis medications. However, by 6 months post-operation, the patient experienced recurrent turbinate hypertrophy and resumed decongestant use, opting not to undergo revision surgery. The second case was a 58-year-old male patient with RM, an rTNSS score of 2, and a NOSE score of 10. He underwent RPN3 surgery without complications and successfully discontinued decongestants and other medications during the 3 month follow-up. However, he experienced recurrent nasal obstruction triggered by cold air and resumed decongestant use 6 months post-operation. On endoscopy examination, bilateral recurrent hypertrophic inferior turbinates were noted with no synechiae or other complication. The patient later requested revision surgery, and a revision RF procedure was performed 10 months after the initial RPN3 surgery, yielding excellent results with no further decongestant dependency.
Regarding complications, one 29-year-old female patient with RM and a deviated nasal septum opted to undergo the RPN3 procedure first, leaving the deviated septum untreated. During the 1st week follow-up, she had successfully discontinued all decongestants and other medications, with a smooth recovery. However, at the 24th day post-operation, she experienced anterior epistaxis, which was managed in the emergency room with anterior nasal packing for 3 days, resulting in no further sequelae. There was no headache, facial pain, dry eye, posterior nasal bleeding, or other severe complications were reported in the study cohort.
Preoperative and 3rd and 12th month follow-up rTNSS and NOSE scores are summarized in Table 2. The mean symptom scores of each questionnaire were not statistically different in all subscores at baseline. During 3 months, the RPN3 had significantly-more improvement in rTNSS score than the RF group (0.7 ± 0.8 vs 2.2 ± 1.4, P-value = .01). The minimum clinically-important difference (MCID) for the rTNSS is −1.0 points and −4.2 to −6.3 on the NOSE scale (on 0-100 scale, equal to −.84 to −1.26 in our result).11,14 During the 3 month follow-up, the RF group had achieved 88.9% MCD in rTNSS and 100% in NOSE. Other follow-up data showed 100% MCID across the entire cohort and in both groups during the 12 month follow-up.
Characteristics of Refractory Rhinitis Medicamentosa Patients rTNSS and NOSE Subscore at the Base Line and at the 3rd and 12th month Follow Up.
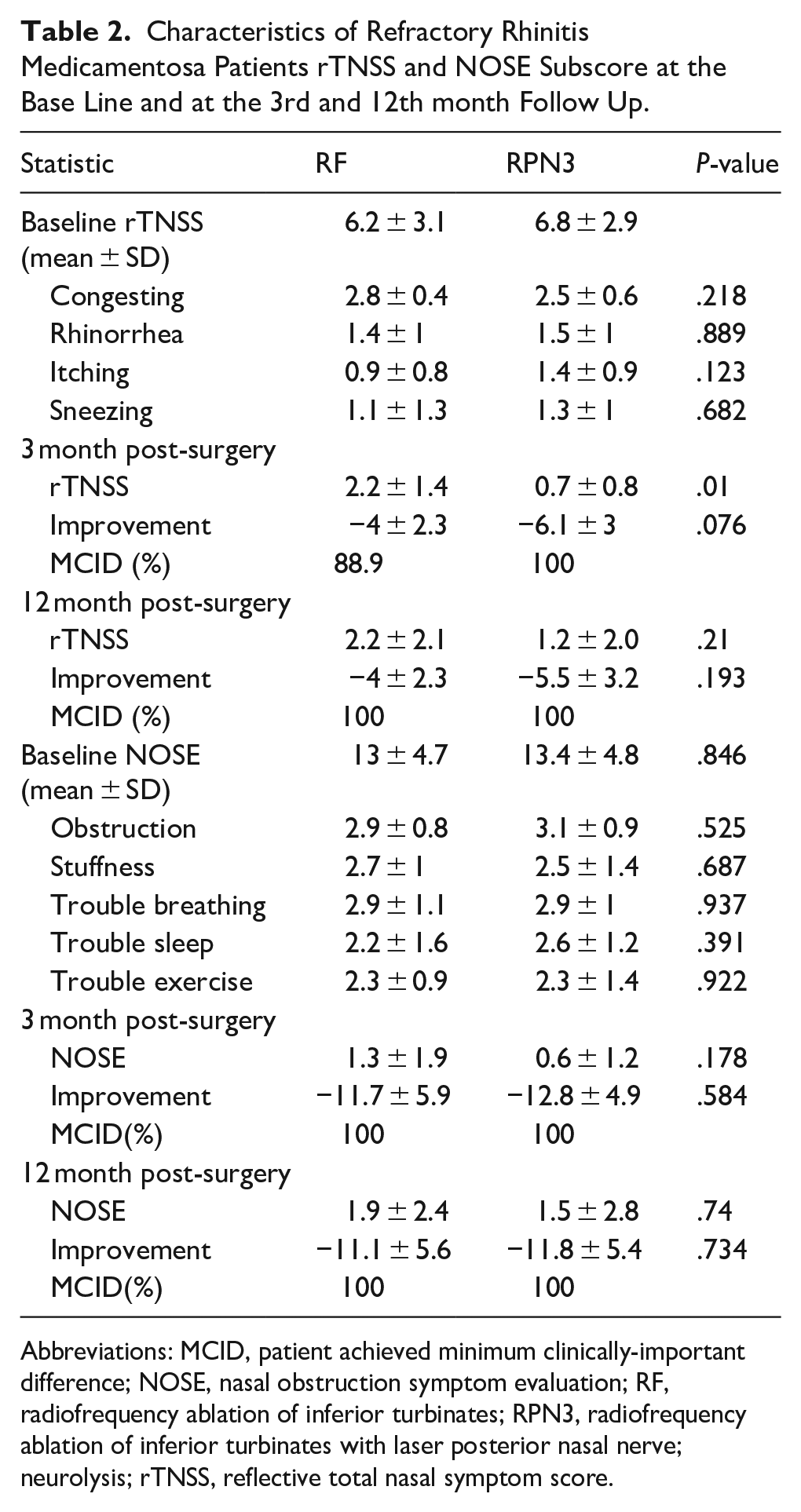
Abbreviations: MCID, patient achieved minimum clinically-important difference; NOSE, nasal obstruction symptom evaluation; RF, radiofrequency ablation of inferior turbinates; RPN3, radiofrequency ablation of inferior turbinates with laser posterior nasal nerve; neurolysis; rTNSS, reflective total nasal symptom score.
The 3 to 12 month follow-up scores of rTNSS and NOSE for the 2 intervention cohorts were presented in Figure 2, with both groups showing a significant difference when compared to baseline at all times (P-value = .065 on 1 month NOSE, <.05-.001 in other follow-up for RF group and <.001 for all RPN3 group).
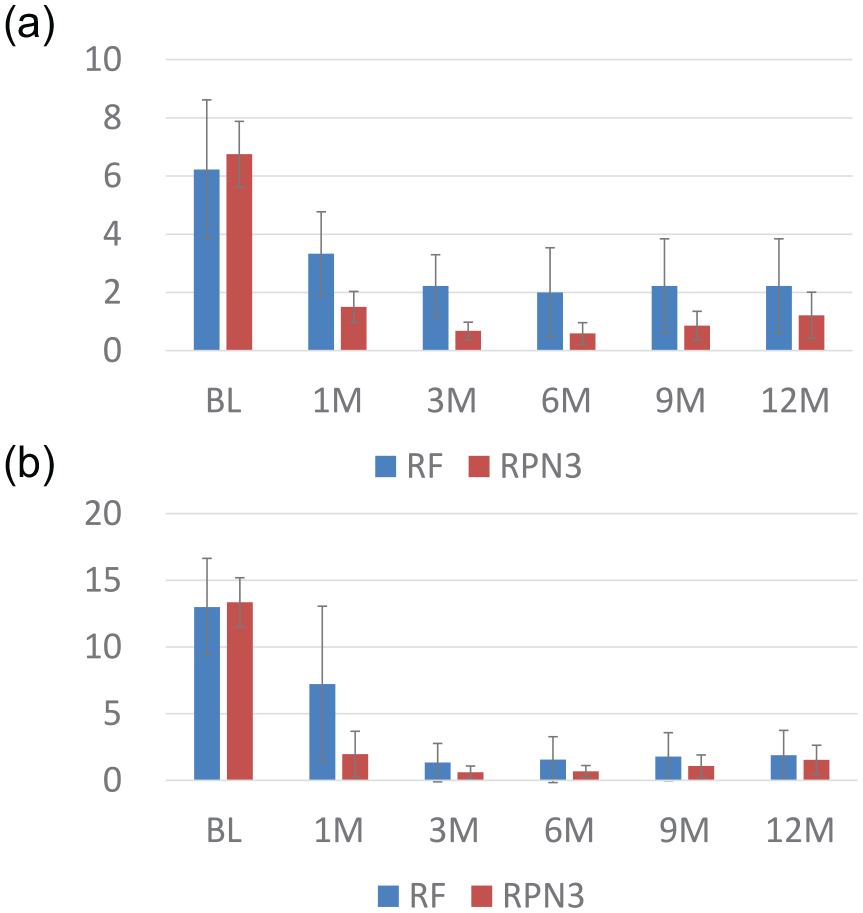
Baseline (BL) and postoperative 1 to 12 month rTNSS and NOSE score of patients with rhinitis medicamentosa receiving radiofrequency ablation of the inferior turbinates (RF, N = 9) alone or with posterior nasal nerve neurolysis (RPN3, N = 28). The error bar indicates a 95% confidence interval. (a) Change in rTNSS. All pre-operation to post-operation 1 month to 12 month changes were statistically significant (P-value = <.05 for RF 1 month, <.01 for 3-12 months for RF group, and <.001 for all RPN3 follow-up), (b) NOSE score. All pre-operation to post-operation 1 month to 12 month changes were statistically significant (P-value = <.001), except for the RF group 1 month follow-up (P-value = .065).
The changes in subscores of NOSE and rTNSS questionnaires are summarized in Figure 3. When comparing the changes in subscores during each follow-up until the 12th month, the most significant improvement was observed in nasal obstruction, with P-value < .001 in both the RF and RPN3 groups. The group undergoing RFA of the bilateral inferior turbinates (RF) demonstrated statistically-significant improvements in congestion scores (P-value < .001), rhinorrhea scores at the 6th month (P-value < .05), and sneezing scores at the 3rd month (P-value < .05). Although itching scores showed improvement, the changes were not statistically significant. In contrast, the RPN3 group exhibited statistically-significant improvements across all 4 symptom subscores at all follow-up time points (P-value < .001 for all).
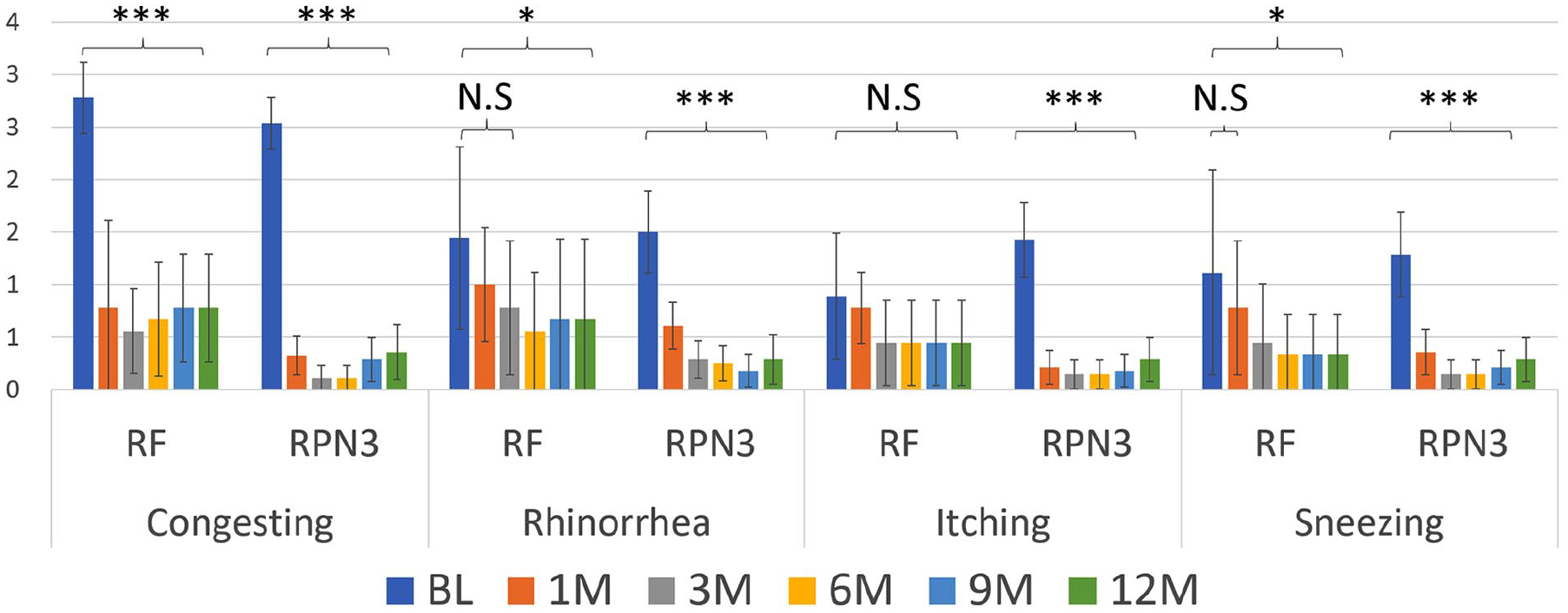
Refractory rhinitis medicamentosa patients’ post-surgery scores changed by 2 different surgical techniques from the 1st month to the 12th month. Error bar: 95% confidence interval. The radiofrequency ablation of the bilateral inferior turbinates (RF) group showed statistically-significant differences in the congesting score (***P-value < .001), rhinorrhea scores after 6 months (*P-value < .05), and sneezing scores after 3 months (*P-value < .05). The itching scores had improved but not statistically significant. The combined RF and bilateral posterior nasal nerve neurolysis (RPN3) group showed a significant difference in all 4 subscores at all follow-ups points (P-value < .001 to all).
Discussion
This study is the first to evaluate CO2 PNNN using the innovative RPN3 technique in RM patients, demonstrating promising results. With this procedure performed under local anesthesia, 94.6% of patients successfully discontinued nasal decongestant use for up to 1 year without serious complications. Our findings provide new evidence for treating medically-refractory RM patients, with or without concurrent allergic rhinitis.
Topical decongestants are classified into beta-phenylethylamine derivatives (eg, ephedrine, phenylephrine) and imidazoline derivatives (eg, naphazoline, oxymetazoline, xylometazoline), with the latter offering greater potency and prolonged effects. For example, 0.1% xylometazoline hydrochloride acts within minutes and lasts up to 10 hours. 3 In our study, patients undergoing medical treatment for over 6 months before surgery had used either oxymetazoline or xylometazoline.
The pathophysiology of RM remains unclear, with proposed mechanisms including chronic vasoconstriction-induced mucosal ischemia, adrenergic receptor desensitization and downregulation, vasomotor tone alteration, and prolonged beta-adrenergic activity.3,15,16 A study has been conducted on animal models or healthy subjects, analyzing the consequences of prolonged nasal decongestant use. 16 Histology changes, including loss of nasociliary function, goblet cell hyperplasia, epithelial edema, and squamous cell metaplasia, have been described in RM based on animal studies.3,15 Clinically, RM presents with nasal mucosa that may appear “beefy red” with punctate bleeding and minimal mucus or edematous with profuse, stringy, mucoid discharge.1,15,17 Persistent nasal congestion is the hallmark symptom, often accompanied by rhinorrhea, itching, and sneezing.
Management primarily involves discontinuing decongestants, along with intranasal corticosteroids and saline irrigation. In refractory cases, surgical intervention may accelerate symptom resolution. A study by Margulis et al. 6 found that surgical treatment significantly reduced decongestant use and improved Sino-Nasal Outcome Test-22 (SNOT-22) scores compared with conservative management.
Our findings indicate that bilateral inferior turbinate RFA significantly improved nasal congestion, rhinorrhea, and sneezing during 1 to 12 months. Nasal itching showed improvement, but this was not statistically significant. Furthermore, combining RFA with CO2 PNNN (RPN3) yielded superior outcomes, significantly improving all rTNSS parameters at both follow-ups. Various surgical techniques have been used for nonallergic rhinitis, including inferior turbinate reduction, submucosal tissue and bone resection, electrocautery, RFA, laser and cryotherapy, microdebridement, lateral bone outfracture, and neural interventions such as vidian and posterior nasal neurectomy. 18 Among these, vidian and posterior nasal neurectomy are particularly effective for refractory cases. A systematic review by Senanayake et al. 19 demonstrated significant improvements in nasal symptoms—particularly rhinorrhea, congestion, and obstruction—following surgical or cryoablative neurectomy. Our study demonstrated that both RF and RPN3 groups achieved significant improvement in total nasal symptom control. However, RPN3, which targets parasympathetic nerve-related symptoms (primarily rhinorrhea), provided significant improvement across all symptoms, including rhinorrhea, nasal itching, and sneezing. This comprehensive symptom control with RPN3 offered superior outcomes compared with RF alone.
Radiofrequency turbinoplasty alone has been shown to alleviate both chronic rhinitis and RM. Li et al. 20 reported that RFA relieved nasal obstruction with a total mean reduction of 56.5%. Other studies showed that 85% of patients experienced improved nasal obstruction with minimal postoperative pain.21,22 Neiderman et al. 5 reported that 24 RM patients treated with RF turbinate reduction showed 76% improvement in NOSE score. Margulis et al. 6 reported 26 patients treated with turbinoplasty utilizing the medial flap technique, which showed 71.3% improvement in the SNOT-22 score. William et al. 7 reported that using medial flap turbinoplasty technique to treat 56 RM patients with 66.4% of improvement in the SNOT-22 score. Our study cohort demonstrated a 64.5% to 82.4% improvement in rTNSS scores and an 85.4% to 88.8% improvement in NOSE scores following the surgical management of RM patients, offering new evidence for the effective treatment of RM patients refractory to medical therapy.
Using a laser to complete PNNN was first published by Krespi et al., 23 who used a diode laser to treat 32 chronic rhinitis patients with promising results. Huang et al.24-26 demonstrated that combining RFA of the inferior turbinate with CO₂ laser PNNN resulted in better symptom control than radiofrequency alone and showed significant improvement until the 6th month follow-up and can be safely performed smoothly in 183 patients under local anesthesia. All the patient in the current study and previous published report could tolerate this procedure well under local anesthesia with a mean surgery time 34 minutes on average with 96% of patients using <10 cc lidocaine for bilateral nasal cavity anethesia. 25 This study is the first to assess CO2 PNNN using the innovative RPN3 technique for RM patients, which also showed promising results.
Limitations of this study include its retrospective design and potential patient selection bias, as surgical choices were based on shared decision-making and patient preference rather than on randomization or consecutive enrollment. As previously noted, patients with more severe symptoms of rhinorrhea, sneezing, and nasal itching (indicated by rTNSS subscores ≥1 in each category) were more likely to opt for the RPN3 procedure. However, there were no statistically significant differences in preoperative rTNSS and NOSE scores and subscores between groups. Future randomized controlled trials are warranted to provide more rigorous evidence and minimize selection bias. The small sample size and short follow-up period are additional limitations, though prior studies have shown the long-term stability of RF and CO2 PNNN effects after 3 months, supporting our findings as preliminary evidence for longer-term studies.7,9,27 Outcome assessment relied on subjective symptom evaluations, as no histological samples were available to confirm mechanisms. Allergy status was not assessed preoperatively, but given the confirmed RM diagnosis in all patients, further testing was deemed unnecessary. Additionally, the absence of psychological evaluation limited the assessment of the mental health impact of RM and the potential psychological benefits of surgery. Future prospective studies with larger cohorts, objective measurements, psychological assessments, and extended follow-up periods are warranted to validate and expand upon these findings.
Conclusion
Surgical management with RF or RPN3 effectively reduces RM symptoms, as demonstrated by significant improvements in rTNSS and NOSE scores during the 12-month follow-up. By adding CO2 PNNN to the RF (aka RPN3), a statistically-significant improvement in all 4 subscore (nasal obstruction, rhinorrhea, itching, and sneezing) was noted. Future randomized controlled trials are warranted to compare its efficacy with conservative management.
Footnotes
Acknowledgements
We thank Sheng-You Su in the Clinical Research Center at Ditmanson Medical Foundation Chia-Yi Christian Hospital for his contribution to data processing and to Hsin-Yi Yang at the Chiayi Christian Hospital Clinical Data Center for her valuable statistical consultation.
Ethical Considerations
The study was approved by the Ethics Committee of Chiayi Christian Hospital (No. CYCH2024022; April 12, 2024).
Consent to Participate
The institutional review board waived the need for informed consent due to the study’s retrospective nature.
Consent for Publication
All authors had consent to publish the article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Ditmanson Medical Foundation Chia-Yi Christian Hospital Research Program (R113-056).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statements
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.