
Abstract
Surgical management of head and neck sarcomas presents significant challenges, particularly in advanced stages where curative options are limited. In such cases, palliative care becomes essential to alleviate symptoms and enhance the patient’s quality of life. When chemoradiation therapy fails to provide adequate symptom control, palliative surgery may be a viable option. We report the case of a 24-year-old male diagnosed with an extensive and aggressive maxillary chondroblastic osteosarcoma. Despite multiple chemoradiation regimens, the disease progressed rapidly. Due to the substantial deterioration in the patient’s quality of life, he underwent major palliative surgery. The procedure involved a left total maxillectomy, right subtotal maxillectomy, left segmental mandibulectomy, orbital exenteration, and resection of the left upper lip, cheek, and nose. Reconstruction was performed using an osteocutaneous fibula free flap and an anterolateral thigh flap. Postoperatively, the patient experienced significant symptom relief without major complications. He was followed for 12 months before being lost to follow-up, remaining disease-free for approximately 8 to 10 months. This case illustrates that in select patients with unresectable and extensively invasive tumors, major palliative resections combined with microvascular reconstruction may offer meaningful improvements in quality of life.
Significance Statement
By focusing on symptom relief, complication management, and improving quality of life, palliative surgery offers significant benefits beyond traditional curative approaches, with the potential to substantially enhance a patient’s overall quality of life. Careful patient selection, timing, and a multidisciplinary approach are essential to maximizing the positive impact of these interventions.
Introduction
The purpose of this paper is to report the course of an extensive and very aggressive maxillary chondroblastic osteosarcoma in a young patient from the Gaza Strip, Palestine. Osteosarcoma is a malignant mesenchymal tumor characterized by the production of osteoid matrix. 1 While osteosarcomas mainly affect the long bones, those occurring in the head and neck region are particularly uncommon, comprising only 6% to 9% of all osteosarcomas and fewer than 1% of all head and neck malignancies.2-4 The mandible is often the most commonly involved bone, and head and neck osteosarcoma rarely involves the maxilla. 5 Chondroblastic osteosarcoma is characterized by the predominant presence of chondroid matrix, which is identified in a quarter of all new osteosarcomas. Its histopathological diagnosis is based on the predominance of chondroid matrix. 5
Head and neck osteosarcoma is often diagnosed in patients between the ages of 13 and 66 years. 6 Various risk factors have been associated with the pathogenesis of osteosarcomas, including chronic osteomyelitis, fibrous dysplasia, Paget’s disease, retinoblastoma, and previous exposure to radioactivity.7,8 The most common symptoms of osteosarcoma include persistent pain, edema, and paresthesia or anesthesia. General signs of the disease, such as fever or considerable weight loss, are rare.
Given the rarity and complexity of sarcomas in the head and neck area, specifically in the maxilla, we present a unique and very aggressive case of chondroblastic osteosarcoma located in the maxilla. This report focuses on the ethical dilemma of performing a very extensive and radical surgical resection and reconstruction in the palliative setting to improve quality of life and extend life for a severely debilitated patient.
Case Report
Medical History
A 24-year-old male, otherwise healthy patient from the Gaza Strip, Palestine, presented to a local hospital in the Gaza Strip with a painful and rapidly growing cheek and upper jaw mass. A transoral biopsy was obtained at a local hospital, and chondroblastic osteosarcoma was diagnosed. Cisplatin-adriamycin systemic therapy was initiated with a transient and partial response following the first cycle, followed by rapid progression thereafter. The mass was found to invade the left orbit and hard palate bilaterally, the anterior soft palate, zygoma, cheek, and lip, despite continuous chemotherapy. Next-generation Sequencing was performed, revealing an NTRK-2 Fusion. The patient was transferred to a tertiary hospital in Jerusalem, Israel, for treatment with Larotrectinib as part of a clinical trial. He received 2 cycles of Larotrectinib without any clinical response while developing thyroiditis. The tumor continued to grow significantly at a rapid pace. He was then transferred to Tel Aviv Sourasky Medical Center in Tel Aviv, Israel, for consideration of surgical therapy.
Upon arrival, the tumor had completely replaced the hard palate and anterior soft palate bilaterally, and most of the upper dentition was floating inside a necrotic tumor mass (Figure 1). The tumor involved the left coronoid and mandibular ramus, frontal and nasal processes of the left maxilla, with direct invasion of the orbital floor and the orbital globe. On repeat MRI and Computed Tomography (CT) scans, the tumor measured 15 cm at its greatest dimension (Figure 2) and showed invasion into the greater wing of the sphenoid, without apparent dural or brain invasion, nor evidence of regional or distant metastasis on total-body CT images. The patient was in a miserable state, suffering from intractable pain and unable to swallow any form of diet. He was isolated in his hospital bed with a strong necrotic odor, refusing to communicate with his family or his young son, whom he had not met for 3 months due to severe cosmetic disfigurement. After a multidisciplinary discussion with head and neck and sarcoma oncologists, it was evident that the tumor was chemo-resistant and so extensive that cure was not a realistic option. We discussed the above situation with the patient, and we offered palliative and supportive care to relieve his suffering and to allow him to return home and be with family. However, the patient insisted on pursuing curative or palliative surgical management, regardless of the surgical risks and the high risk of progression and early recurrence. The patient understood the risks and the palliative aim of the surgery well.

Clinical images of the mass involving the maxillary bone bilaterally and the left orbit and nose (A–D).
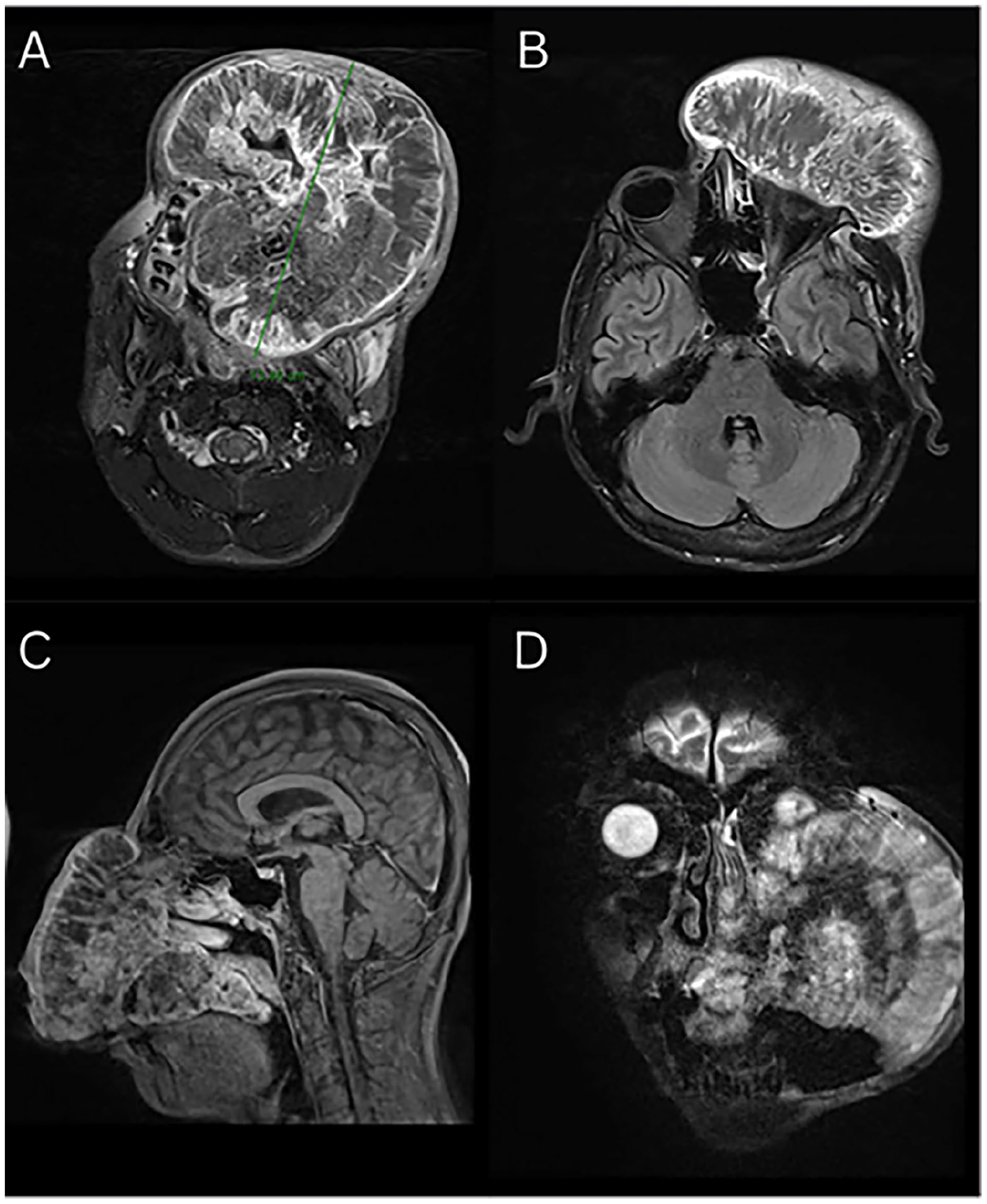
Head and neck MRI: Axial T2 showing massive mass involving the maxillary bone and hard palate bilaterally, left orbit, and left nasal bone (A, B). Sagittal T1 with contrast (C). Coronal T2 with mass involving the left maxilla and invading the orbital floor (D).
Surgical Treatment and Pathological Findings
In February 2023, the patient underwent a percutaneous gastrostomy insertion and a tracheostomy, followed by extensive ablative surgery, including a left total maxillectomy, a right subtotal maxillectomy, a left segmental mandibulectomy that included the ramus and left condyle, a left upper lip resection, cheek skin resection, a left nose resection, and a left orbital exenteration. The greater wing of the sphenoid bone was found to be involved and was drilled out by the neurosurgeon until a normal-looking dura was achieved (Figure 3). The patient was then reconstructed with 2 microvascular free flaps by the plastic-reconstruction team. An osteocutaneous fibula free flap was utilized to reconstruct the left lateral maxillary buttress and anterior alveolar ridge, with its skin pedicle reconstructing the soft and hard palate mucosa, and an Anterolateral thigh (ALT) flap to reconstruct the left orbital and cheek defect (Figure 3).
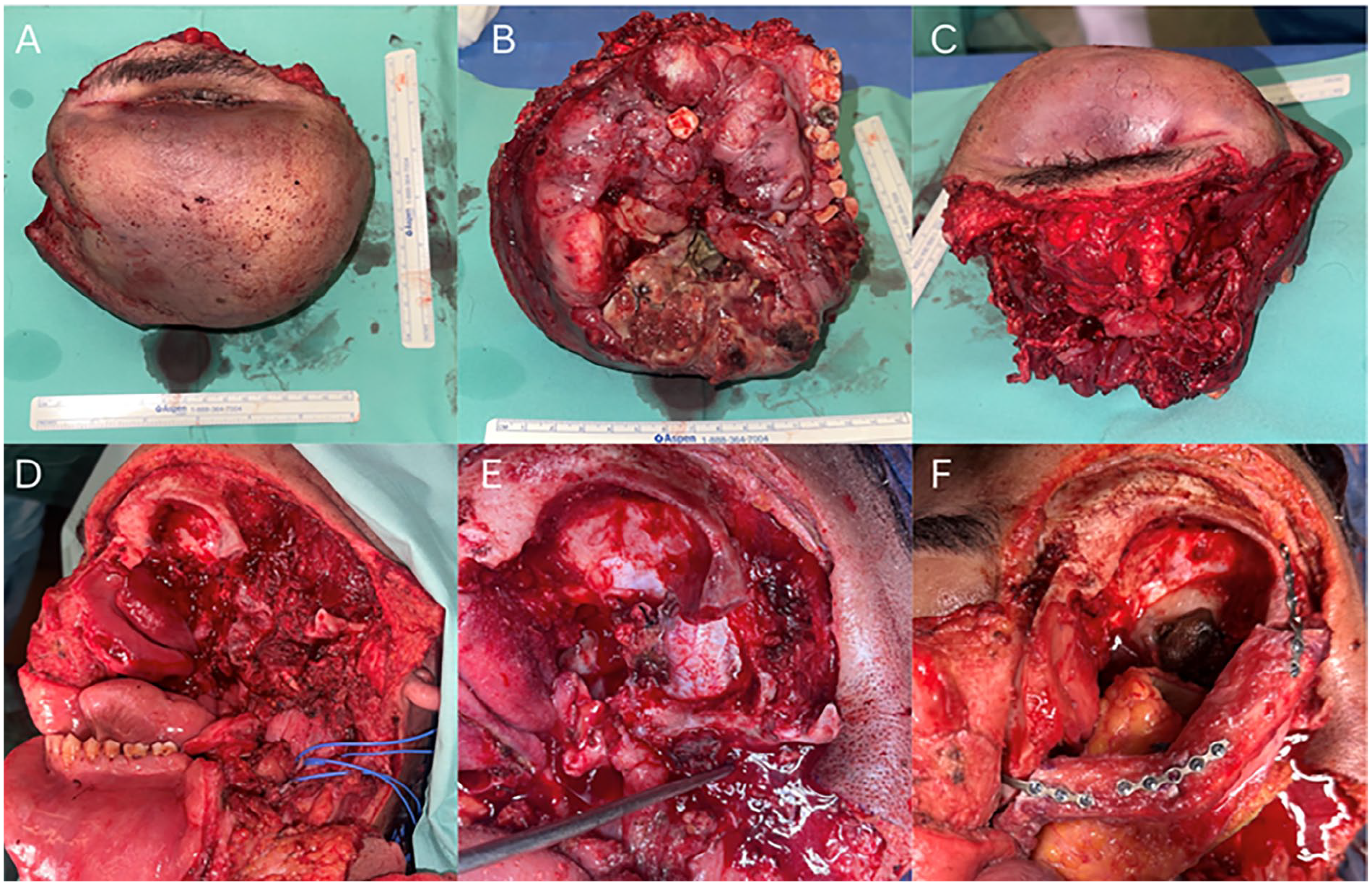
Clinical images of the mass after resection involving the cheek, upper lip, orbit, and nose (A, B) and alveolar ridge bilaterally and palate (C). Images of the surgical defect following the resection (D). Sphenoid bone drilling with dura exposure (E). Reconstruction of the lateral orbital wall and anterior alveolar ridge with fibula free flap.
Histopathological analysis confirmed high-grade chondroblastic osteosarcoma with a viability of at least 90% of tumor cells (Figure 4).
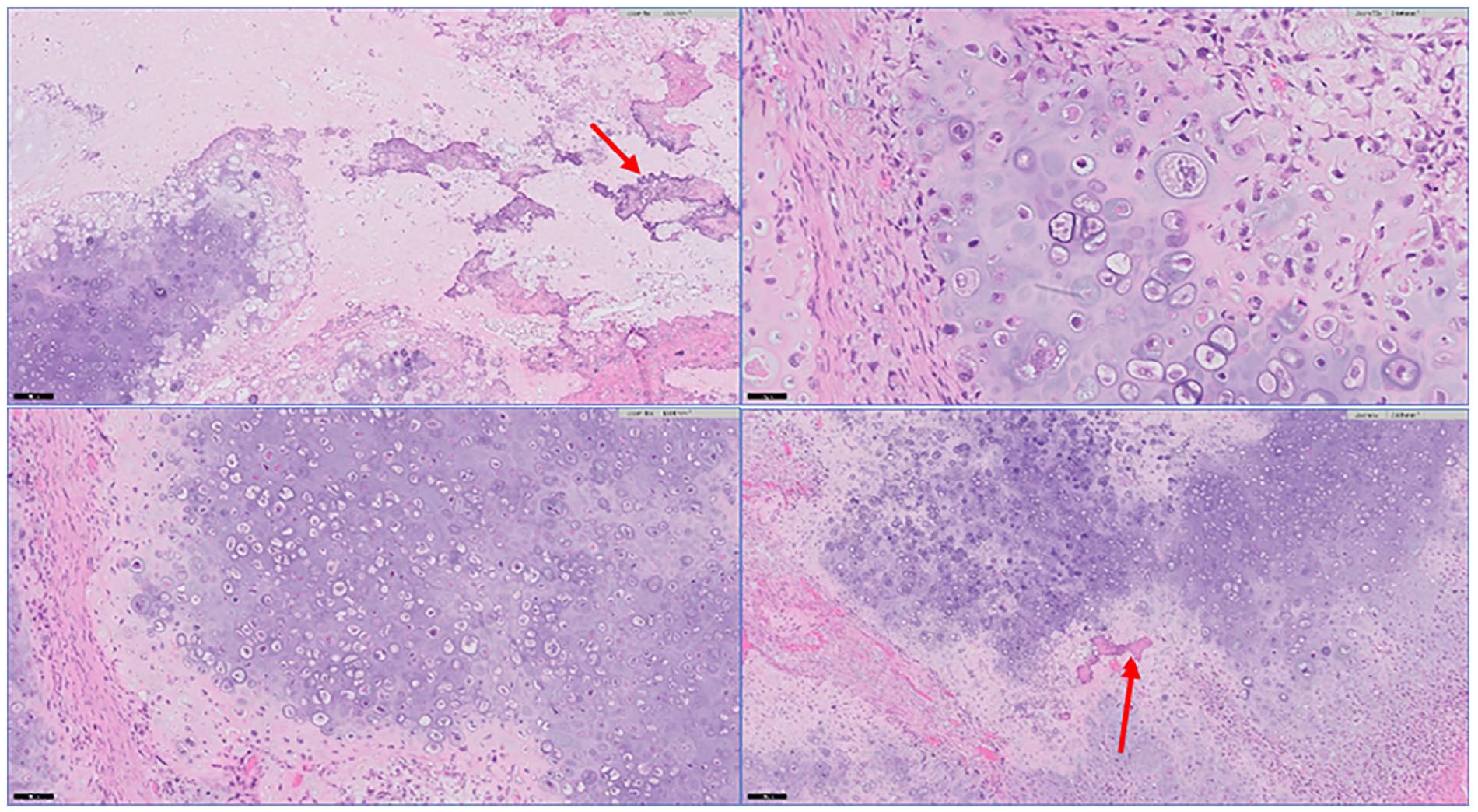
Light microscopy examination with hematoxylin and eosin staining showing chondroblastic osteosarcoma with cartilage and cartilage-like tissue in various stages of maturation associated with osteoid matrix (A–D). Red arrow showing osteoid matrix (A, D).
Postoperative Course
Mild complications arose, including anemia requiring transfusion and minor dehiscence of the ALT flap, which were managed conservatively. The patient then remained hospitalized for an additional 2 months (due to the complexity of the case and the limited resources in the Gaza Strip) to complete an adjuvant radiation therapy course using Volumetric Modulated Arc Therapy technique, receiving 66 Gray in 2 Gray fractions. A postoperative multidisciplinary discussion concluded that no additional adjuvant chemotherapy or targeted therapy is warranted, given the limited response to preoperative chemotherapy. The patient was discharged home 2.5 months following surgery.
Follow-Up Visits
The patient returned to the Gaza Strip and stayed with his family. For the initial 8 months post-surgery, the patient maintained regular telehealth video follow-ups (over WhatsApp) without any notable issues. He experienced minimal pain, and resumed a soft oral diet. The patient was satisfied with his appearance, the relief of pain, and the reduction of foul odor (Figure 5). He was able to socialize with his family and his toddler, and was satisfied with the surgical outcome.
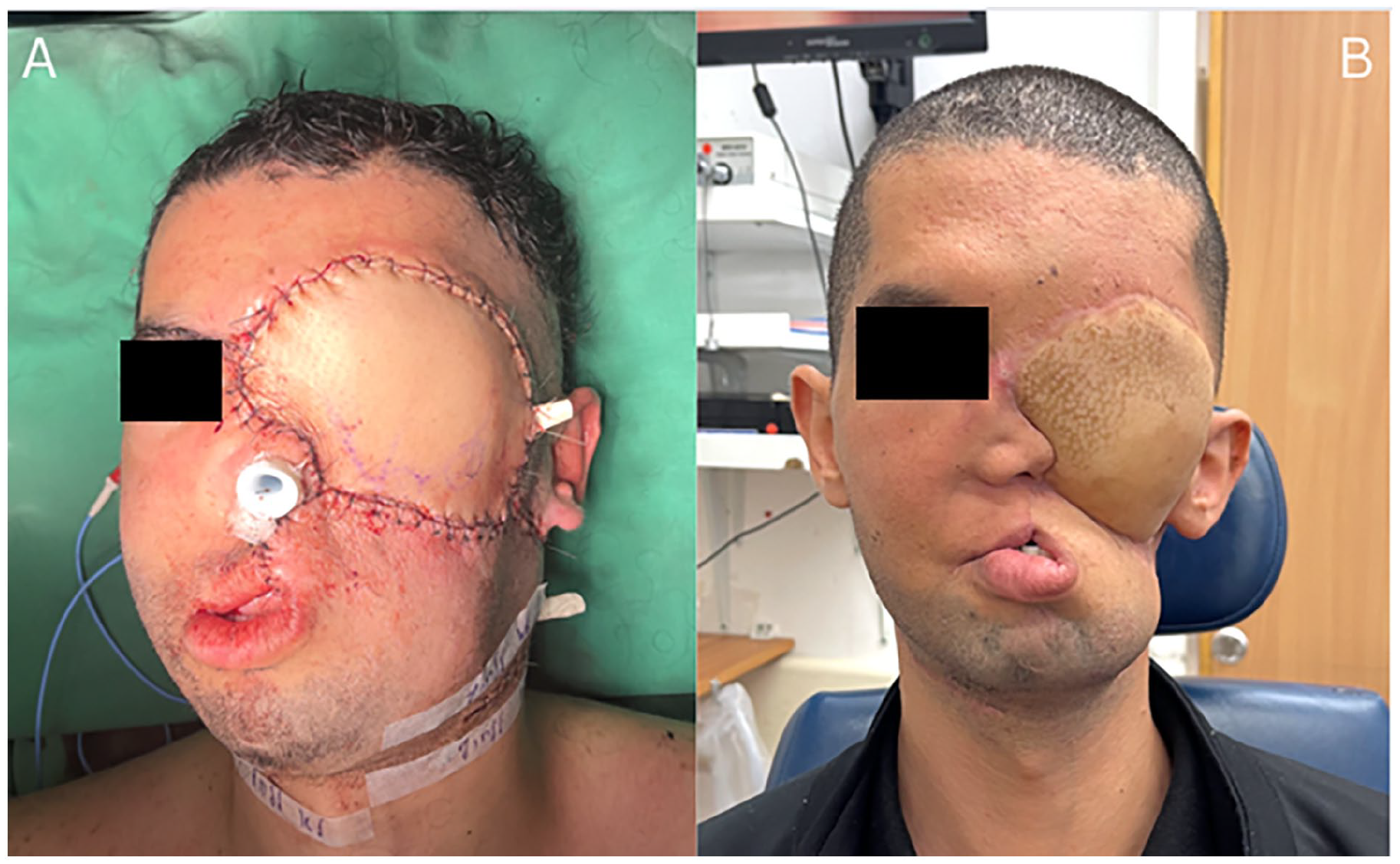
Clinical images of the patient immediately after surgery (A) and 8 months following surgery (B).
Sadly, the patient was not able to perform any follow-up scans in the Gaza Strip or attend any in-person follow-up visits in Israel. Eight months following the completion of treatment, the patient was expected to follow-up with the head and neck surgery clinic physically; however, his visit was canceled with the onset of war between Hamas and Israel. Communication with the patient was lost for a few months before it was briefly resumed via WhatsApp messages when the patient was transferred out of the Gaza Strip to Abu Dhabi, UAE, for medical therapy (10 months following surgery). On repeat MRI, the patient was found to have a significant deep recurrence involving the base of the skull and the sphenoid bone with intracranial extension. The patient remained asymptomatic, with no notable pain or swallowing difficulty. The patient was started on Larotrectinib without radiological response, followed by different chemotherapy regimens. The patient then started to report headaches and sight deterioration in the remaining right eye due to compression of the optic chiasm by the tumor, in addition to a rapidly enlarging subdermal forehead mass. The patient decided to stop all medical therapy and return home to be with his family in the Gaza Strip. Communications were then lost with the patient, and he was assumed to have succumbed to his disease.
Discussion
Osteosarcoma of the maxillofacial skeleton is a rare and highly aggressive osteoid-producing malignant tumor, presenting significant challenges in both diagnosis and treatment. Management typically requires a multidisciplinary approach, aiming to achieve adequate surgical margins while preserving vital adjacent structures and maintaining the patient’s quality of life.9-16
While surgery is well-established as a curative intent, its role in palliative care is less frequently explored. Palliative surgery, defined as the removal of cancer tissue to improve a patient’s quality of life without aiming for complete eradication of the cancer, involves various interventions in incurable head and neck cancer.17,18 These interventions typically range from tracheostomy and gastrostomy placement to different shapes of resection.19,20
However, radical procedures such as total laryngectomy and laryngopharyngectomy, as well as the use of free flaps for palliative purposes, are currently limited to case reports and small case series.21-25 For instance, in a retrospective study involving 25 patients who underwent regional or free flap procedures with palliative intent for head and neck malignancies with extensive skin involvement, 88% were discharged without the need for extensive wound care and only 3 patients experienced major wound complications, suggesting that these procedures could play a role in enhancing the end-of-life experience for patients. 21 Another case series described 3 cases in which the latissimus dorsi free flap was used after palliative resection of extensive basal cell carcinoma. 22 Shinozaki et al reported the use of a free jejunal flap after palliative total laryngopharyngectomy in 2 patients. 23
Herein, we present a case of advanced-stage osteosarcoma, refractory to several chemotherapy regimens, that underwent extensive palliative surgery, contributing to the limited body of literature on the subject.
Upon examining the potential yield of palliative surgery, most studies have focused on symptom relief, including alleviating foul odors, pain, bleeding, and infection associated with skin wound complications. Although survival rates may not improve significantly, palliative surgical interventions have shown positive outcomes in symptom management. One study examined the outcomes of surgical interventions for managing symptoms in advanced head and neck cancer, including procedures such as debridement, debulking, mandibulectomy, maxillectomy, free flap reconstruction, and major vessel ligation. The study concluded that surgical palliation can be safely performed, providing symptom relief in a carefully selected group of patients. 17 Another retrospective study by Cho et al involving 18 patients who underwent palliative surgery for head and neck cancer between 2002 and 2017 also reported significant reductions in pain scores and improvements in cancer-related wounds. 25 Interestingly, Jang et al, in their case series of 22 patients, proposed that although palliative surgery did not extend overall survival, it could alter the course of disease progression, allowing patients to die of distant metastases while sparing them the suffering of fungating tumors during their final months. 21
In our case, the patient experienced debilitating symptoms, including foul odor, dysphagia, and cosmetic deformity, which hindered his ability to engage with his family and his toddler. The surgery alleviated his pain and suffering, enabling him to resume life with an acceptable quality for almost 1 year following surgery.
When considering palliative surgery, particularly one that involves free tissue transfer, several important factors must be taken into account. The first challenge is determining how long it can effectively provide symptom relief in patients with incurable head and neck cancers. Previous studies have indicated that tumors often start to regrow within 1 to 9.5 months after surgery. In our patient, recurrence was noted 10 months after the procedure.24,25 However, he remained with an acceptable quality of life for almost 1 year following surgery, and his recurrence was completely hidden and asymptomatic for a longer period of time.
Second, some might argue that free tissue transfer is unnecessary or not recommended in a palliative context, considering the potential operative and postoperative complications. However, the utilization of free flap reconstruction in the palliative setting allows the oncological team to perform more radical surgery, with better chances of achieving the targeted relief of symptoms. In addition, a 2-team approach does not significantly increase operative time in most cases and is often highly reliable with a low rate of complications.
Third, the cost-effectiveness of microvascular surgeries is also a concern. Generally, microvascular surgery is expensive, with postoperative care costing between $30 000 and $50 000/case. On the other hand, palliative care is also expensive when considering office visits, wound management, and medications with a cost of almost 5000$ a month.26-28
These considerations highlight the need for careful patient selection, as individuals with poor overall health and multiple comorbidities may have a higher surgical risk for this type of palliative intervention. The approach and extent of surgery should be individualized according to each patient’s needs, wishes, and performance status, as this can provide them with a dignified quality of life.
Conclusions
By focusing on symptom relief, complication management, and improving quality of life, palliative surgery offers significant benefits beyond traditional curative approaches, with the potential to substantially enhance a patient’s overall quality of life. Careful patient selection, timing, and a multidisciplinary approach are essential to maximizing the positive impact of these interventions.
Footnotes
Ethical Considerations
This case report was conducted in accordance with the ethical guidelines for medical research and publication.
Consent to Participate
The patient’s confidentiality was strictly maintained to ensure that no identifying personal information was disclosed. Images used in the report were altered to ensure that the patient’s identity could not be disclosed.
Consent for Publication
Written informed consent was obtained from the patient for the publication of this case report.
Authors Contributions
Eiman Abu Bandora: methodology, writing—original draft, visualization. Nariman Abd Elhadi: writing—original draft, visualization. Sofi Matot: writing—original draft. Arik Zaritski: conceptualization. Ofer Merimsky: conceptualization. Orit Gutfeld: conceptualization. Leonor Leider-Trejo: conceptualization. Nidal Muhanna: supervision, writing—review and editing. Jobran Mansour: supervision, writing—review and editing, project administration.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.