
Abstract
The management of refractory chronic rhinosinusitis (CRS) in children with cystic fibrosis (CF) remains a challenge, especially in those who are not candidates for highly effective modulator therapy. These patients often have severe sinus disease that does not improve with medical treatment, requiring surgery as the definitive treatment. We report a case of a 9-year-old female patient with CF and refractory CRS presenting with significant nasal obstruction, postnasal drainage, and frontal headaches that severely impacted her quality of life. A hybrid technique that involved balloon catheter dilation (BCD) along with endoscopic sinus surgery (ESS) allowed the management of complex anatomical problems associated with the severe polyposis, copious purulence, and narrow frontal recesses during the surgery. This improved our ability to visualize the surgical field, minimize blood loss, and better preserve the mucosa, which ultimately led to better surgical and clinical outcomes. Our findings suggest that hybrid BCD-assisted ESS may offer an effective solution to manage severe CRS in pediatric CF patients, particularly for those who have limited therapeutic options.
Keywords
Introduction
Chronic rhinosinusitis (CRS) occurs in approximately 2% of all children and nearly 100% of children who have cystic fibrosis (CF). CRS can significantly affect quality of life, interfering with childrens’ daily functions and causing frequent discomfort or sinus pain.1–3 In pediatric patients, CRS is defined as the presence of two or more of the following symptoms –nasal congestion, nasal discharge, facial pressure, or cough – along with endoscopic evidence of mucosal edema or purulent discharge, or characteristic findings on imaging. 4 CRS is particularly common in pediatric patients with CF since the underlying pathophysiology of the genetic disease impairs mucociliary clearance and leads to thickened mucus secretions and recurrent sinus infections.5,6
Pediatric care of CF-CRS has a few unique challenges. These patients have high recurrence rates due to persistent bacterial colonization and the presence of nasal polyps, which exacerbate inflammation and worsen sinus drainage. 5 More recently, highly effective modulator therapies (HEMTs), such as Elexacaftor/Tezacaftor/Ivacaftor (ETI), have revolutionized CF care. 7 HEMT are small molecule drugs that are based on restoring cystic fibrosis transmembrane conductance regulator (CFTR) protein function, thereby enhancing mucociliary clearance and reducing airway inflammation. 8 HEMT is indicated in patients with at least one F508del CFTR mutation, which is the most frequent in the United States. 9 ETI have proven to result in improvements in sinonasal symptoms, decrease in sinus opacification, and increase in quality of life within the first few months of treatment.9,10 However, patients who experience rare or limited CFTR mutations are left ineligible for treatment. 11 In such patients, and in those with persistent symptoms despite treatment, endoscopic sinus surgery (ESS) is an important adjunct. 12
Surgical management in pediatric CF-CRS patients is also complicated by both anatomical and physiologic factors. The small size of the nasal and sinus anatomy in children increases the technical difficulty of performing ESS, and edematous mucosa and thick secretions may obscure visualization with increased risk of bleeding. 13 In addition, minimizing anesthesia time is important to reduce the risk of pulmonary complications and potential impacts on neurodevelopment. 14 The Food and Drug Administration (FDA) warns against repeated or extended use of general anesthetics in children and recommends that procedures be limited to under 3 hours to reduce risks to brain development. 15
Addressing these challenges requires surgical techniques that can improve visualization and efficiency while minimizing risk in anatomically complex cases. We present a pediatric patient with CF and refractory CRS who was unfortunately not eligible for HEMT. A hybrid approach combining balloon catheter dilation (BCD) and ESS was used to navigate these challenges.
Case Presentation
A 9-year-old female with CF presented with worsening postnasal drainage, nasal obstruction, and frontal headaches. Her medical history was notable for growth failure requiring a gastrostomy tube for nutritional support and a diagnosis of Mycobacterium avium complex lung disease. Her copious postnasal drainage frequently triggered coughs, which resulted in vomiting of tube feeds and complicating her nutritional management.
Computed tomography (CT) showed extensive mucosal inflammation and thickening of the frontal sinuses (Figure 1), correlating with her clinical presentation. These findings, along with worsening of her symptoms, prompted the Pulmonology CF team to recommend ESS to improve nasal obstruction, sinus drainage, and the delivery of topical rinses to the sinuses.
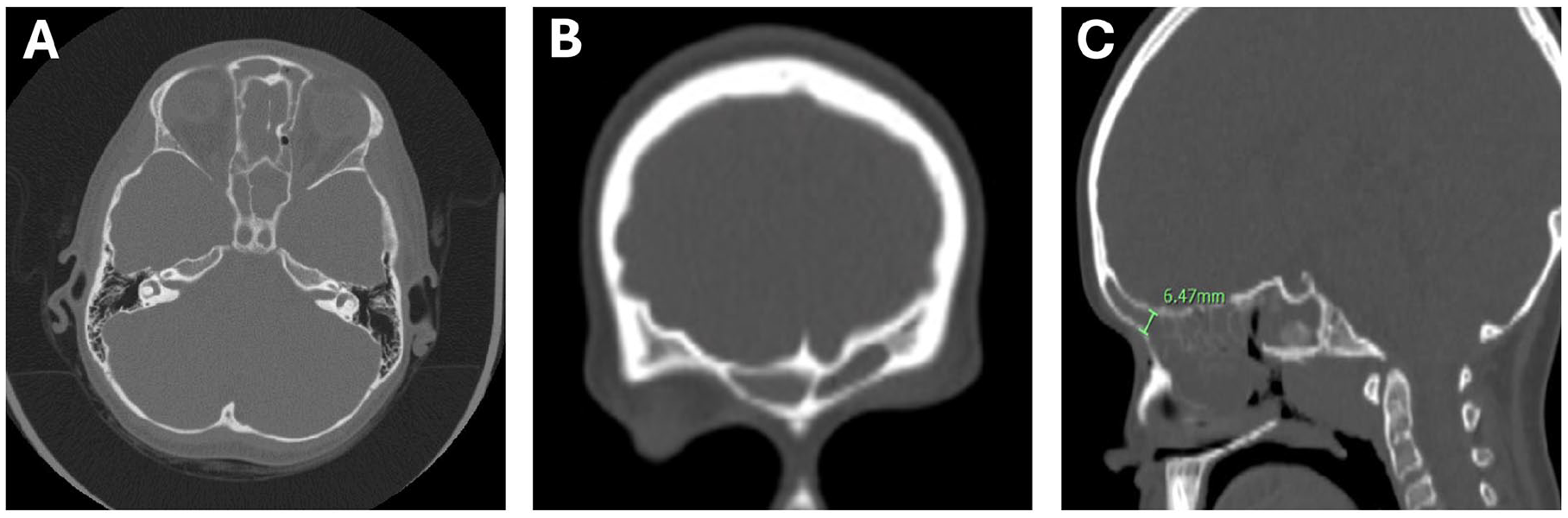
CT) images. (A) Axial, (B) coronal, and (C) sagittal views showing diffuse mucosal thickening and inflammation involving the frontal sinus.
During surgery, heavy inflammation and purulence obstructed the view, making clear visualization of the surgical field difficult (Figure 2A). There was also a concern that aggressive instrumentation could lead to mucosal injury and potential long-term stenosis of the sinus. Given the patient’s small stature and underlying lung disease, the surgical team prioritized minimizing bleeding and reducing the overall anesthesia time.
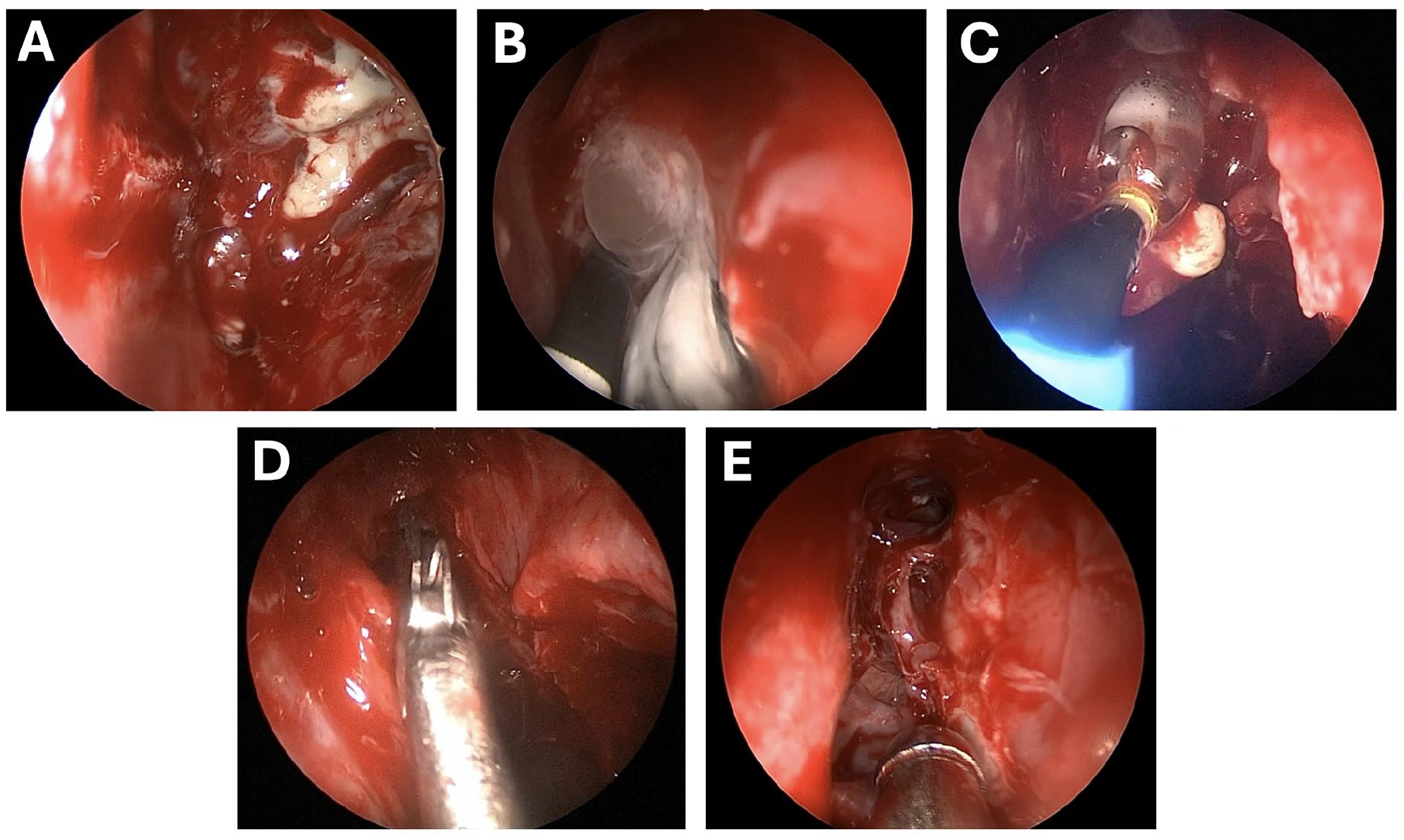
Intraoperative views of hybrid balloon-assisted ESS. (A) Obstructed nasal cavity with extensive inflammation, nasal polyposis, and purulent secretions. (B) Narrow and inflamed frontal recess with limited surgical access. (C) BCD of the frontal recess to improve access to the sinus. (D) Saline irrigation delivered through the balloon catheter. (E) Postoperative appearance showing improved sinus patency and resolution of obstruction.
A balloon catheter was used to assist with access to the frontal sinus (Figure 2B). Afterward, the guide wire was inserted into the frontal ostia and transillumination was confirmed. The balloon was then advanced over the guide wire and inflated to the appropriate pressure (Figure 2C). After retraction of the guide wire, irrigation was instilled into the sinus through the balloon device (Figure 2D). Once irrigation was completed, the balloon device was subsequently removed, and the dissection of the frontal recess was completed using curved through-cutting forceps and standard techniques.
The patient tolerated the procedure well with minimal bleeding, and the surgery was completed well within the desired anesthesia time of under 3 hours. At her second-look debridement 4 weeks later, both frontal ostia remained patent (Figure 2E).
Discussion
Management of refractory CRS is difficult for children with CF, especially when conventional interventions fail. The presence of inflammation, excessive mucosa, and narrow sinus anatomy added significant barriers in planning and surgical intervention in our patient. To solve those matters, we applied a hybrid BCD-assisted ESS, which enhanced the visual field, reduced blood loss, and preserved the mucosa during the procedure.
Treatment options for pediatric CF-CRS patients generally involve both medical and surgical therapy. 1 Initial therapy may include medical treatment to include antibiotics, nasal irrigation, and corticosteroids. While HEMT such as ETI have been demonstrated to relieve sinonasal symptoms for many children with CF, it is available only for those with specific CFTR mutations. ETI is currently indicated for those patients who have at least one F508del mutation or any of the FDA-accepted variants of CFTRs, such as I601F, G85E, S492F, M1101K, R347P, R74W, V201M, D1270N, and H1085R. Thus, patients with few functional variants or certain rare mutations are not treatable with ETI. 16 The annual cost of ETI is above $250,000, which demonstrates the challenges of bringing an affordable effective treatment to all the patients. 17
While HEMT has revolutionized medical treatment for numerous patients, it is not able to reverse preexisting anatomical defects within the sinuses. In the setting of extensive nasal polyposis and narrow frontal recesses, as in our present case, operative management is still needed to remove obstruction, ensure drainage, and restore full function to the sinuses. Even in HEMT patients, some residual disease is likely to remain, especially in cases of complex anatomy. In these cases, personalized, multimodal therapy including ESS is integral to the management of these patients. In such patients for whom HEMT therapy is inappropriate or whose symptoms remain severe and refractory to treatment, a surgical approach may be necessary.
In our case, BCD, also known as balloon sinuplasty, was used as part of the surgical approach. This method involves placing a small balloon into the sinus drainage pathways and gently inflating it to open up the space. Because it avoids cutting into tissue, it may reduce bleeding and may be safer in patients with higher surgical risk. 18 Although BCD has been used in pediatric CF-CRS and appears to be safe, the evidence on how well it works, especially as a standalone treatment, is still not sufficient. 19 Some studies suggest that it may be less effective than traditional surgery when used by itself, suggesting its role as an adjunctive therapy to other treatments instead.20,21
ESS is another common surgical procedure utilizing a nasal endoscope and cutting instruments to clear sinus obstructions in pediatric CF-CRS patients. It has been shown to be effective in pediatric patients, with often higher parent satisfaction and success rates compared to adenoidectomy alone.22,23 Its low rates of complications, including readmission and reoperation, also highlight its safety in the pediatric population. 24 While there have been concerns raised regarding its possible effects on midface growth, human studies showed no significant effect on facial development in children who underwent ESS. 25
Here, the use of BCD combined with revision ESS in those with more difficult anatomy has been described in a few studies. In difficult revision cases of frontal sinus surgery, BCD has been used to assist visualization and for safe access. 26 In one randomized study, the combination of BCD and ESS resulted in reduced bleeding and operative time, with frontal sinus openings remaining patent after one year. 27 Taken together these results indicate that the use of hybrid techniques may improve operating room productivity and patient healing in the setting of more complex sinus cases.
Conclusions
This case emphasizes the challenge of managing refractory CRS in children with CF, particularly in those who are ineligible for HEMT. The hybrid technique using BCD and ESS has promising therapeutic effects for the management of sinusitis with complex anatomy and inflammation. By improving surgical efficiency, reduced bleeding, and preserving mucosa, this approach may provide a promising option for the treatment of refractory CRS in this complex patient cohort.
Footnotes
Ethical Considerations
This case report did not require ethics committee approval.
Consent to Participate
Written informed consent to participate was obtained from the patient’s legal guardian.
Consent for Publication
Written informed consent for publication of the case details and accompanying images was obtained from the patient’s legal guardian.
Author Contributions
E.O.: Conception, design, literature review, writing – original draft, figure preparation. O.S.: Writing – review & editing, figure preparation. J.Z.: Writing – review & editing, figure preparation. B.O.: Data acquisition, writing – review & editing. E.H.F.: Conception, design, data acquisition, literature review, writing – original draft, figure preparation, supervision.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Elisabeth Ference is a paid speaker and consultant for Optinose and Regeneron/Sanofi. Other authors declare no potential conflicts of interest with respect to the research, authorship, or publication of this case report.
Data Availability Statement
Not applicable.