
Abstract

Significance Statement
Intraparotid lymphadenitis should be considered in the differential diagnosis of parotid masses, particularly in patients with recent upper respiratory symptoms, given its potential to cause significant cervical cellulitis and airway compromise. This case underscores the broader impact of COVID-19 on salivary gland pathology and highlights the need to consider SARS-CoV-2 in parotitis-like presentations, even in vaccinated individuals. Clinicians must be cognizant of the potential for airway compromise and significant cervical cellulitis, as this condition can present substantial diagnostic and management challenges.
Case Presentation
In late 2022 to early 2023, amid the continuing COVID-19 pandemic, a 54-year-old male with a medical history of hypertension and obesity presented to the emergency department with fever, left-sided erythematous cervical edema, and progressively worsening dyspnea that had developed over the past few hours. Notably, he had experienced influenza-like symptoms a few days prior following familial exposure. The patient also had a previously resolved dental infection, which had been managed through multiple consultations without the need for intervention.
Cervical CT (Figure 1A and B) imaging showed extensive infiltration of the left submandibular and parapharyngeal spaces causing near-total tracheal occlusion with rightward displacement. A hypodense mass was noted near the inferior parotid gland with adjacent fat infiltration, but no ductal dilation, sialolithiasis, or dental source. Internal jugular veins were patent, and cervical lymph nodes showed no necrosis.
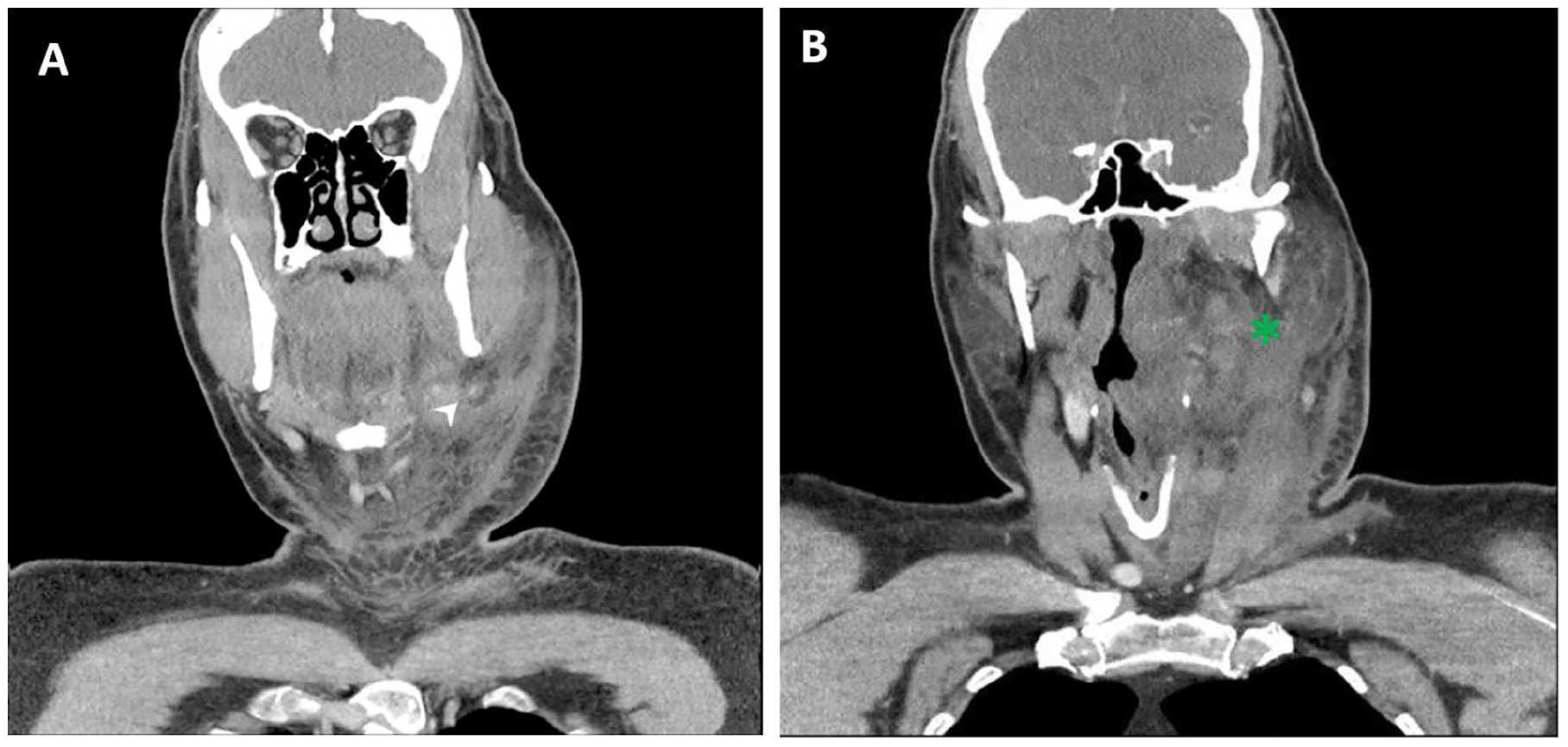
CT images. Cervical CT imaging, axial (A) and coronal reconstruction images (B) demonstrated extensive infiltration of the left submandibular and parapharyngeal spaces (*), extending caudally to the hypopharynx, resulting in near-total tracheal occlusion and rightward displacement. A hypodense mass (arrowhead) was identified in the inferior portion of the parotid gland, accompanied by adjacent fat infiltration, but without dilation of the Stensen duct or involvement of the parotid gland itself. No sialolithiasis or left-sided dental focus was observed. Vascular assessment revealed preserved patency of both internal jugular veins, with no evidence of venous thrombosis. Several lymph nodes were identified in the left cervical region, with no signs of necrotic adenopathy.
The patient underwent awake intubation in the emergency department and was subsequently transferred to the intensive care unit for respiratory monitoring. Intravenous empiric antibiotic therapy with amoxicillin and clavulanic acid was initiated. A rapid progression of cervical edema was noted following admission, while erythema remained unchanged. Blood cultures and bronchial aspirate cultures were obtained, both of which returned negative results. The patient later tested positive for SARS-CoV-2.
He was extubated on day 5. While the cervical swelling resolved, an indurated, painless mass persisted at the tail of the parotid gland. Ultrasound-guided fine-needle aspiration cytology of the lesion revealed lymphocytes with no significant distortion, neutrophils, and no evidence of malignant or atypical cells. At the 3-month follow-up, magnetic resonance imaging demonstrated complete resolution of the lesion, with no evidence of residual mass or cyst.
Discussion
Among the salivary glands, the parotid glands are unique in that they arise from the oropharyngeal ectoderm and undergo encapsulation later in embryological development, resulting in the entrapment of lymphatic tissue within both the parotid capsule and parenchyma.1-3 The parotid lymph node group includes the subcutaneous pre-auricular nodes, superficial and deep intraparotid nodes, and subparotid nodes. 4 Cadaveric studies indicate that the superficial lobe accounts for about 90% of all intraparotid lymph nodes, which are predominantly situated along the retromandibular vein, particularly within the parotid tail.1,2 The superficial lobe typically harbors 4 to 7 lymph nodes, while the deep lobe generally has no more than three. 3 Normal intraparotid lymph nodes typically measure less than 6 mm in diameter.1,2
Similar cases have been described in the literature, notably by Mannuru et al., 5 where a 51-year-old male with COVID-19 developed acute neck swelling due to diffuse cellulitis and reactive sialadenitis without a drainable abscess. 6 The authors emphasize that SARS-CoV-2 may contribute to systemic inflammatory responses or secondary bacterial infections, leading to atypical head and neck presentations. 5 Given that COVID-19 has been associated with an increased risk of secondary bacterial infections, reported in 6.9% of cases in a meta-analysis by Mannuru et al., 5 it is plausible that SARS-CoV-2 infection predisposed this patient to a superimposed deep neck space infection.
Friedrich et al. 7 described a case of severe COVID-19 complicated by parotid gland abscess formation requiring surgical drainage. The authors highlighted that xerostomia and mechanical factors during intensive care may predispose to parotitis in COVID-19 patients. 7 SARS-CoV-2’s affinity for salivary glands via angiotensin-converting enzyme 2 (ACE2) receptors supports direct viral involvement, with glands acting as viral reservoirs contributing to the spread. 7 The case also raised questions about the potential role of immunomodulatory therapy (eg, tocilizumab) in the pathogenesis. 7
Lechien et al. 8 described 3 cases of COVID-19 patients presenting with parotitis-like symptoms characterized by unilateral ear pain and retromandibular swelling. The patients recovered with symptomatic treatment, but persistent anosmia remained. 8 The authors proposed that intraparotid adenitis may impair salivary gland function by obstructing Stensen’s duct, leading to saliva retention and inflammation. 8 This mechanism differs from classic viral parotitis, such as mumps, and highlights the role of immune-mediated lymphadenitis in SARS-CoV-2 infection. 8 The presence of ACE2 receptors in parotid tissue supports possible direct viral involvement. 8
Chern et al. 9 and Capaccio et al. 10 both reported cases of acute nonsuppurative sialadenitis involving the parotid and submandibular glands in patients with confirmed SARS-CoV-2 infection, suggesting that salivary gland involvement may represent an early or atypical manifestation of COVID-19. This is supported by animal studies demonstrating viral tropism for salivary duct epithelial cells and by the consistent detection of high viral loads in saliva, reinforcing the hypothesis of direct viral infection of the salivary glands.9,10
Small, normal intraparotid lymph nodes are frequently observed on imaging, specifically on MRI. 3 Occasionally, these nodes undergo reactive enlargement, often due to conditions such as upper respiratory infections, and may be mistaken for parotid tumors. 3 Enlarged intraparotid lymph nodes typically present with a homogeneous appearance, exhibiting computed tomography (CT) attenuation and magnetic resonance imaging (MRI) signal characteristics similar to extraparotid lymph nodes, and should not be confused with tumors. 3 Reactive hyperplasia generally involves multiple nodes and is frequently accompanied by extraparotid nodal enlargement. 3 By contrast, Warthin’s tumor, which can be multifocal and extend into extraparotid tissue, appears more heterogeneous, with cystic areas, nodules, and intense enhancement, making it distinguishable from lymph nodes. 3
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Consent to Participate
Written informed consent was obtained from the participant included in the report.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.