
Abstract
Vestibular schwannomas are benign tumors originating from Schwann cells of the 8 cranial nerve. Patients with vestibular schwannoma most commonly present with hearing loss, followed by tinnitus and disequilibrium. We report the case of a 73-year-old gentleman who initially presented with an asymmetric hearing loss and was subsequently diagnosed to have a unilateral vestibular schwannoma. The patient elected to proceed with a wait-and-scan management approach. During his follow-up period, imaging showed there was limited growth of the tumor with solidification of a cystic component of the tumor. Notably, during the same period, his high-frequency sensorineural hearing loss (SNHL) worsened to a severe SNHL in all frequencies with very poor speech discrimination. At subsequent 1-year follow-up, his hearing had improved to a serviceable hearing level. While the natural history of vestibular schwannoma suggests hearing loss over time, this case highlights the variable nature of hearing changes, including slow decline, sudden hearing loss, and even some return of hearing function. This report underscores the potential for hearing recovery in conservatively managed vestibular schwannoma with implications for hearing rehabilitation and patient-centered decision-making.
Keywords
Introduction
Vestibular schwannomas originate from Schwann cells of the eighth cranial nerve and are the most common benign tumor of the cerebellopontine angle (CPA). Hearing loss is the most common initial presenting symptom for vestibular schwannoma (VS), occurring in 90% of cases, followed by dizziness or imbalance and tinnitus. Oftentimes, a wait-and-scan, or active surveillance approach to initial management is undertaken, and patients are followed with serial magnetic resonance imaging (MRI). 1 Radiographic studies have shown a 10% to 20% rate of spontaneous volumetric shrinkage in observed vestibular schwannomas, though with progressive worsening hearing loss. 2 Herein, we present the case of a spontaneously regressing vestibular schwannoma with improvement in hearing.
Case Report
A 73-year-old gentleman with a history of type 2 diabetes mellitus initially presented with a complaint of high-frequency unilateral hearing loss in 2017. MRI undertaken for asymmetric hearing loss showed a right intracanalicular vestibular schwannoma extending slightly into the CPA (Koos grade 2) with a maximum linear length of 17.6 mm in 2017. He elected to proceed with a wait-and-scan approach to management of the tumor. Serial imaging from 2017 to 2019 showed limited growth of the CPA component of the tumor associated with some cystic changes. From 2019 to 2024, the cystic components of the tumor solidified, and the overall size of the tumor decreased (maximum linear length 16.9 mm). MRI T1 fat-suppressed post-gadolinium contrast-enhanced sequences from 2017 to 2024 are shown in Figure 1.
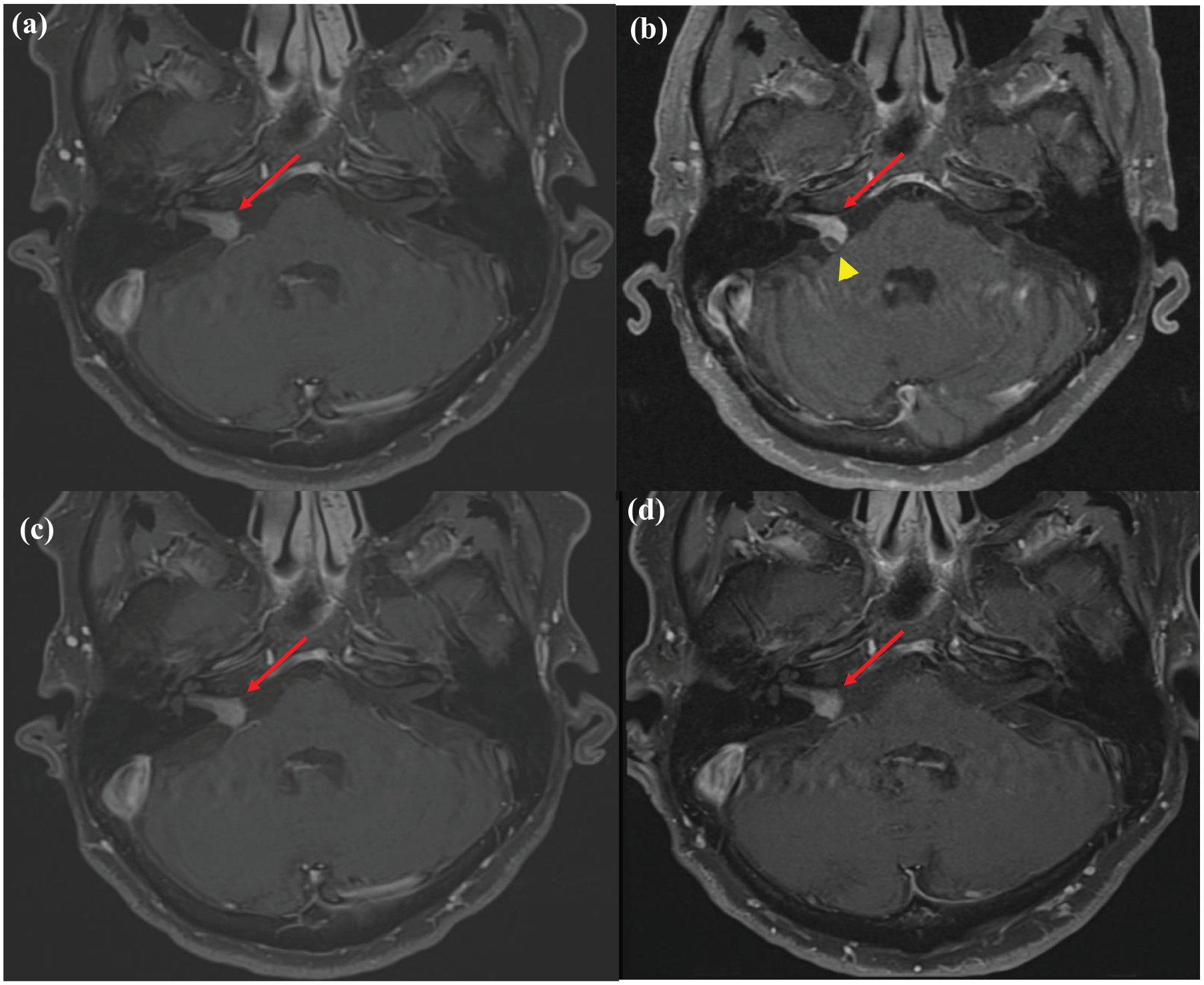
MRI T1-weighted, fat-suppressed, post-gadolinium enhanced contrast sequences showing a right vestibular schwannoma (red arrows) from 2017 to 2024. The yellow arrowhead shows the cystic component seen in 2019. (a) 7 years prior (initial), (b) 5 years prior, (c) 1 year prior, and (d) most recent.
Regarding his hearing, he presented with a mild to severe high-frequency sensorineural hearing loss (SNHL) in the right ear, specifically at 6 and 8 kHz. He had a drop in mid-range frequency at 1 and 1.5 kHZ to mild-moderate SNHL in 2018. At his follow-up in 2023, his hearing had significantly worsened to severe SNHL in all frequencies (pure tone average [PTA] 80 dB) and very poor speech discrimination (4% word recognition score), or Gardner-Robertson hearing grade IV (non-serviceable). At his next follow-up in 2024, his hearing had improved dramatically, especially in the low frequencies (PTA 46 dB) and improved speech discrimination (56% word recognition score), with improvement to Gardner-Robertson grade II (serviceable). See Figure 2 for audiograms. Other than taking a multivitamin, no major lifestyle changes or new medications had been started. After the discussion, he decided to continue with the observation of the tumor and would consider undergoing a hearing aid evaluation.
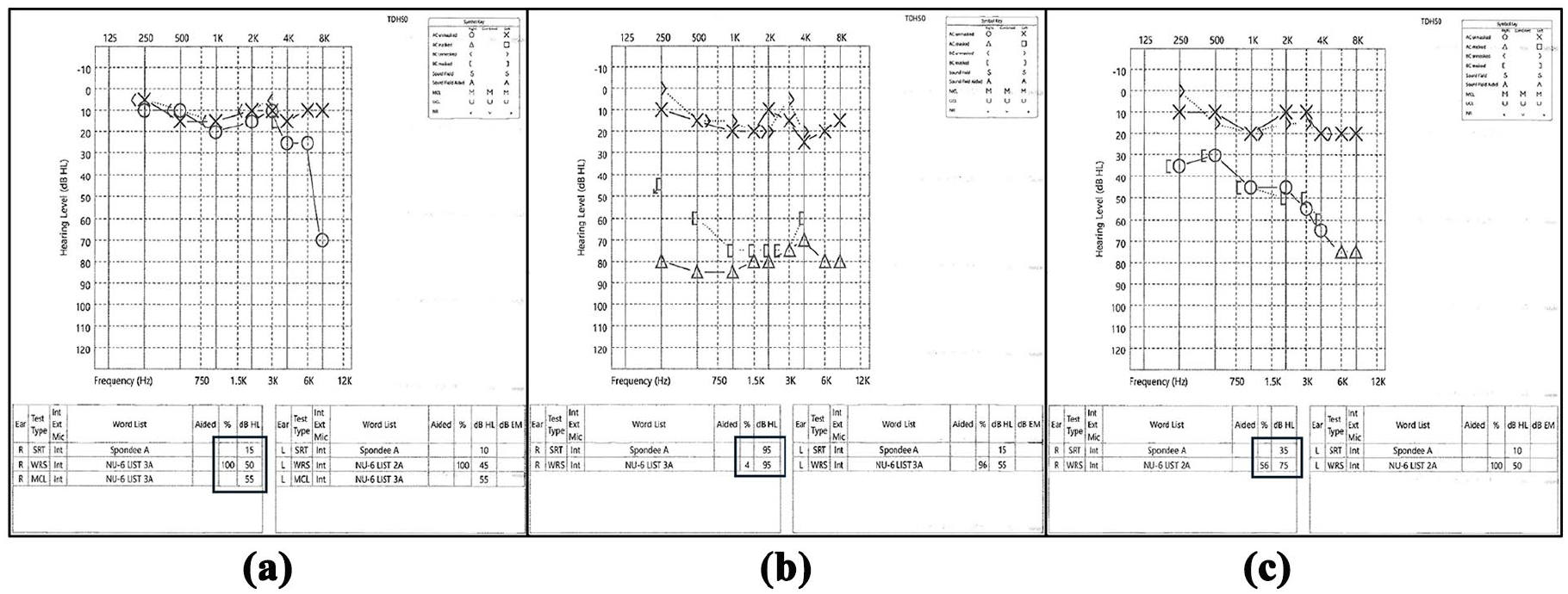
Audiograms from 2017 to 2024, showing severe SNHL with partial recovery to a serviceable hearing state. (a) Initial (7 years ago), (b) prior (1 year ago), and (c) most recent.
Discussion
A review of the literature identified a similar case from Wachi et al., 3 in which a middle-aged female presented with facial palsy and numbness, was discovered to have a moderate SNHL (PTA 50 dB) which improved to normal hearing level (PTA 25 dB) along with spontaneous regression of the tumor from 13.5 to 8.4 mm maximum intracranial diameter during 3 years of follow-up. This case is distinct in that the patient experienced a drop from essentially normal hearing to severe SNHL, and 1 year later with improvement to moderate SNHL, going from non-serviceable to serviceable hearing classification. There are other case reports of patients experiencing sudden hearing loss in the setting of a known vestibular schwannoma with hearing improvement after steroid treatment and subsequent tumor size regression. 4
The pathophysiologic mechanism for hearing improvement in the setting of a vestibular schwannoma is unclear and may be multifactorial. Daoudi et al. 2 showed that despite spontaneous regression of VS tumor size, hearing loss often progressed. Gurewitz et al. 5 highlighted increased risk of hearing loss with increased growth rate in a linear pattern, though not all patients progress in this manner, and the associations between tumor size and hearing loss are limited. 1 In this case, there was radiographic evidence of a cystic component of the tumor that regressed in size; it is possible that this relieved pressure on the cochlear nerve, allowing for hearing improvement. Besides mass effect, it is unknown whether the local tumor microenvironment or neurovascular interface played a role in the hearing recovery.
Conclusion
Spontaneous hearing recovery not associated with sudden hearing loss in the setting of a known vestibular schwannoma is extremely rare. Improvement in hearing in patients previously electing to proceed with a wait-and-scan approach may have implications on hearing rehabilitation options and patient-centered decision-making regarding future VS management.
Footnotes
Acknowledgements
None.
Ethical Considerations
Our institution does not require ethics approval for reporting individual cases.
Consent to Participate
Written informed consent was obtained from the patient for this work.
Consent for Publication
Written informed consent was obtained from the patient for the publication of this case report.
Author Contributions
JKA has no conflicts of interest to report and made a significant contribution to concept, design, acquisition, and interpretation of data, drafted the article, and approved the final version for publication. ZS has no conflicts of interest to report and made a significant contribution to the concept and design of the article, critically revised the article for intellectual content, and approved the final version for publication. GW has no conflicts of interest to report and made a significant contribution to concept, design, acquisition, and interpretation of data, critically revised the document for important intellectual content, and approved the final version for publication. All authors agreed to be accountable for all aspects of the work and resolved any issues related to its accuracy or integrity.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article, as no datasets were generated or analyzed during the current study.