
Abstract

Significance Statement
Auricular pseudocyst (AS) is rare in infants without standardized treatment. While deroofing surgery with pressure dressing is commonly used, less-invasive options are preferred in infants due to anesthetic concerns. In this case, we demonstrate an infant successfully treated with continuous negative pressure aspiration, which is a safe, minimally invasive, and cosmetically favorable option. No recurrence or deformity was observed at 6 months follow-up, suggesting this approach as a promising alternative for AS in infants.
An 8 week-old female infant presented with a progressive, nontender, cystic swelling over the left auricle noted at 4 week-old. The swelling was located over the scaphoid fossa, triangular fossa, and concha cymba (Figure 1A), and nonerythematous, with no history of birth trauma or perinatal complications. There was no fever, external wound, or infection sign. Trauma and child abuse history was denied. The patient underwent intravenous antibiotics treatment and repeated needle aspiration at other hospital, but in vain. Based on the clinical history and laboratory data, a diagnosis of auricular pseudocyst (AS) was established. Given the patient’s age and the parents’ concern about cosmetic outcomes, we opted for a minimally invasive treatment using continuous negative pressure aspiration (CNPS).
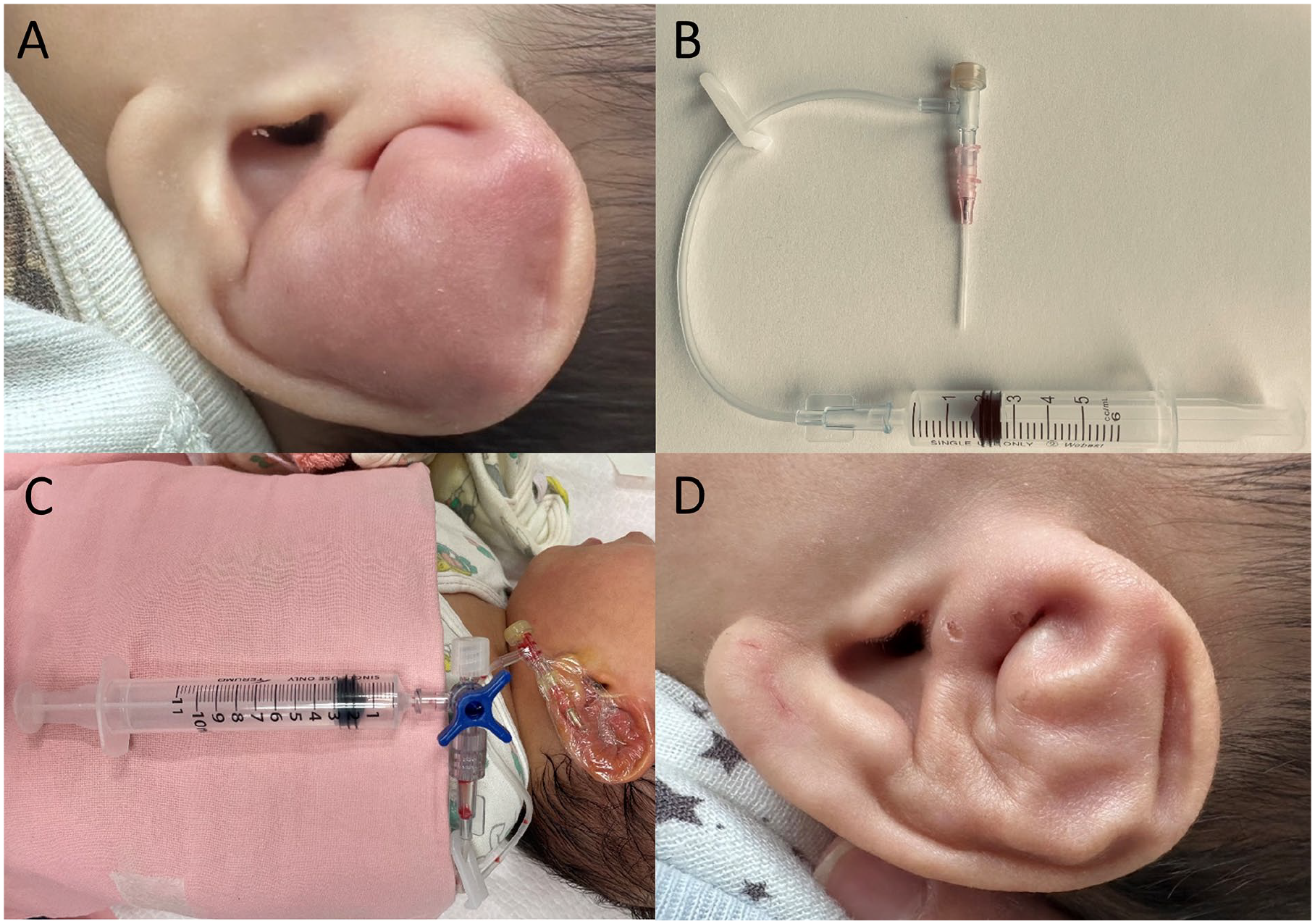
(A) Auricular pseudocyst prior to negative pressure drainage. (B) Negative pressure drainage device assembled using a Tegaderm dressing, an intravenous infusion needle, a drainage tube, and a 10 ml syringe. (C) Clinical appearance of the infant during treatment with the drainage system in place. (D) Appearance of the auricle at 6 month follow-up.
First, needle aspiration 6.5 ml of AS was obtained, which is clear, straw-colored fluid, and cytological analysis revealed lymphocytes and macrophages without neutrophils. Bacterial cultures were negative. Then, intravenous indwelling needle was inserted into pseudocyst space, and connected to a sterile drainage tube and a sealed syringe (Figure 1B and C). No local anesthesia or sedation was required. The sealed syringe was first drawn to 2 mL, which is gradually increased to 6 ml, which created a near-complete vacuum pressure in the absence of air, ~−1033 cm H2O.
Empiric antibiotics of amoxicillin-clavulanate was also given for 7 days to prevent auricular perichondritis. The device remained in place with daily monitoring and adjustment of the reservoir to maintain adequate drainage. The swelling gradually resolved without signs of infection. The drainage volume on day 7 was 0, so the drainage tube was removed. At 6 month follow-up, no recurrence was noted and the auricle maintained its shape and symmetry (Figure 1D).
AS is an asymptomatic, noninflammatory cystic swelling caused by fluid accumulation within an unlined intracartilaginous cavity. 1 Lesions are typically located on the anterior auricle, most often in the scaphoid or triangular fossa, and primarily affect young males, with rare occurrence in children or the elderly. 2 The pathogenesis remains unclear, though proposed mechanisms include embryologic potential spaces or trauma-induced cartilage degeneration.3,4
Conventional treatments for AS such as aspiration or pressure dressing alone have high recurrence rates. 5 Deroofing surgery with anterior cartilage resection followed by pressure dressing is considered effective in adults but may not be ideal for infants due to anesthetic concerns. 5
Dong et al first described CNPS in 2021, showed no recurrence in 32 adult patients with AS over a 3 month follow-up. 6 This method provides uniform pressure to promote closure of the cavity, is simple to perform bedside, avoids surgery and anesthesia, preserves normal tissue, and offers better cosmetic outcomes. Treatment duration can be adjusted based on drainage volume.
This case highlights CNPS as a safe, simple, effective, and minimally invasive treatment option for infantile AS or for patients unsuitable for surgery. In our case, no recurrence was observed, and the auricle retained its shape and symmetry; however, the potential for future auricular deformity cannot be excluded. Long-term follow-up in additional cases is needed to confirm efficacy and monitor for delayed adverse outcomes.
Footnotes
Ethical Considerations
Ethical approval to report this case was obtained from Chang Gung Medical Foundation Institutional Review Board (IRB: 202500238B0).
Consent to Participate
Written informed consent to participate in this study was provided by the patient’s legal guardians.
Consent for Publication
Written informed consent was obtained from the patient’s legal guardians for the publication of anonymized clinical images or data included in this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.