
Abstract
Background:
Clinicians frequently encounter patients manifesting with sinonasal symptoms meeting diagnostic criteria for rhinosinusitis, yet demonstrating radiologically-negative sinus computed tomography (CT) findings. These patients typically exhibit poor response to conventional pharmacological therapies. Investigating the pathogenesis of these patients is critically important.
Methods:
This retrospective cohort study characterizes 53 cases of CT-negative symptomatic sinonasal disorders (CTN-SSD) compared with 132 chronic rhinosinusitis without nasal polyps (CRSsNP) controls, utilizing standardized metrics including the following: symptom visual analog scale, Lund-Kennedy endoscopic scores, 22-item Sino-Nasal Outcome Test (SNOT-22), and Lund-Mackay CT scoring.
Results:
The CTN-SSD group demonstrated a greater proportion of female relative to the control group (73.58% vs 63.36%, P < .001). Of the patients with CTN-SSD in the study, 69.81% fulfilled the International Classification of Headache Disorders, third edition diagnostic criteria for migraine. The CTN-SSD cohort showed significantly-higher prevalence of posterior rhinorrhea (P = .028) and headache/facial pain (P < .001), whereas CRSsNP patients predominantly exhibited nasal obstruction, anterior rhinorrhea, and olfactory dysfunction (P < .001). While mucoid secretion rates were comparable between 2 groups (P = .153), purulent discharge exclusively occurred in CRSsNP cases (P < .001). In addition, mucosal swelling was significantly-more prevalent in CRSsNP patients than in patients with CTN-SSD (P < .001). There was no significant difference in SNOT-22 scores between the 2 groups. However, the CRSsNP group scored higher in the nasal subdomain, whereas the CTN-SSD group demonstrated elevated scores in the aural/facial and psychological subdomains (P < .001).
Conclusions:
Patients with symptoms of sinusitis but negative CT finding frequently meet the diagnostic criteria for migraine, and the possibility cannot be excluded that their symptoms are nasal presentations of migraine resembling those of rhinosinusitis, which may result in inappropriate therapies.
Keywords
Introduction
Chronic rhinosinusitis (CRS) is a heterogeneous disease with chronic inflammation involving at least one of the paranasal sinuses. The main clinical manifestations of CRS include anterior or posterior rhinorrhea, and nasal congestion, and the secondary symptoms include headache/facial pain and hyposmia. A diagnosis is made when at least 2 symptoms are present, with at least 1 being a main symptom. 1 The prevalence of CRS in the general population varies from 5% to 12%. 2 It is thought to be one of the most common diseases, interfering with school, work, and social activities, and also causing a substantial economic burden for sufferers. CRS can be grouped into with nasal polyps (CRSwNP) or without nasal polyps (CRSsNP), which is easily recognized by clinicians.
The Lund-Mackay scoring system (LMKS) and computed tomography (CT) imaging are widely-used and generally-reliable tools for diagnosing CRS. 3 However, clinicians increasingly encounter patients presenting with typical symptoms of CRS—including nasal obstruction, purulent discharge, and facial pain—who demonstrate no abnormal findings on paranasal sinus CT scans. Among patients presenting with clinical symptoms meeting the diagnostic criteria for CRS, 44% had negative CT scans. 4
Cranial autonomic symptoms of primary headache disorders (PHDs) such as nasal congestion and rhinorrhea, can mimic the symptoms of chronic sinusitis, leading to misdiagnosis and inappropriate therapies.5,6 It has been realized that autonomic nerve symptoms occur relatively frequently in patients with migraine, which is one of the most common PHDs, ranging from 27% to 73%.7-9 A substantial proportion of patients ultimately diagnosed with migraine had persistently misattributed their symptoms to rhinosinusitis over an extended period and were given inappropriate antibiotics. 10 A definitive diagnosis and appropriate treatment are very important. Therefore, this study aimed to analyze the clinical characteristics of symptomatic patients meeting the diagnostic criteria for CRS despite negative sinus CT findings and explore their relationship with PHDs.
Materials and Methods
We retrospectively analyzed 53 CT-negative symptomatic sinonasal disorders (CTN-SSD) adult patients with a disease history of at least 12 weeks from the otorhinolaryngology outpatient clinic of our hospital between May 2023 and August 2024, with 153 consecutively-enrolled CRSsNP patients exhibiting positive sinus CT findings (Lund-MacKay score >5) during the same period serving as the control group. The diagnosis of SSD was based on the presence of at least 2 symptoms consistent with CRS, one of which must be a primary symptom such as anterior or posterior rhinorrhea, and nasal congestion. CRSsNP patients with fungal sinusitis or rhinosinusitis of dental origin were excluded. All these patients had completed symptoms scores, nasal endoscopy scores, CT scan scores, and the 22-item Sino-Nasal Outcome Test (SNOT-22) scores. This study was approved by the Medical Ethics Committee (MEC) of Peking University People’s Hospital (PKUPH). All methods were performed in accordance with the MEC of PKUPH guidelines and regulations. All the patients provided written informed consent.
Assessments
Symptoms Scores
Visual analog scale (VAS) was used to assess the severity of each symptom (congestion, anterior and posterior rhinorrhea, facial pain, and hyposmia). Patients draw a vertical line on a 10 centimeter line to indicate the level of discomfort for each symptom.
Nasal Endoscopy Scores
The nasal endoscopic scores were assessed by the Lund-Kennedy endoscopic scoring system (LKES). 11 The endoscopic score included nasal discharge and mucosal status. Normal nasal discharge, clear secretion, and purulent secretion were scored as 0, 1, 2 points orderly. The mucosa with normal appearance was scored 0, hypertrophy without erythema was scored 1, and hypertrophy with erythema was scored 2.
CT Scans Scores
The LMKS was used to evaluate the CT scans scores. 12 Bilateral maxillary, frontal, anterior, posterior ethmoid, sphenoid sinuses, and ostiomeatal complex were scored. Zero was no opacity, 1 was partially opaque, and 2 was completely opaque. The entire CT scores ranged from 0 to 24 points.
The SNOT-22
Twenty-two individual symptoms were assessed according to the severity of 0 to 5 for each item. The severity was classified according to the following criteria: 0 was “no problem”; 1 was “very mild problem”; 2 was “mild or slight problem”; 3 was “moderate problem”; 4 was “severe problem”; and 5 was “problem as bad as it can be.” The total scores ranged from 0 to 110. The form was categorized into 4 subdomains including nasal (items 1-6, 21-22), aural/facial (items 7-10), sleeping problems (items 11-18), and psychological issues (items 19-20). 13
Statistical Analysis
Data were analyzed using SPSS (ver 17.0; SPSS, Inc, Chicago, IL, USA). Categorical variables were compared with chi-squared tests, and continuous variables with independent t-tests. To complement null hypothesis testing, effect sizes were calculated as follows: Cohen’s w for chi-squared tests (categorical variables) and Cohen’s d for t-tests (continuous variables).
Results
Clinical Characteristics
The study consisted of 132 patients with CRSsNP and 53 with CTN-SSD. All the patients with CTN-SSD were at their first visits to the otolaryngology office due to headaches and nasal symptoms. According to the International Classification of Headache Disorders, third edition criteria, among the patients with negative sinus CT findings, 37 (69.81%) were migraine, 3 (5.66%) diagnosed as tension headache, 5 (9.43%) diagnosed as cluster headache, and 8 (15.09%) diagnosed as others that cannot be grouped (Figure 1). Demographic data comparisons between the 2 groups are listed in Table 1. No significant difference was found in the age and symptom duration of the 2 groups. However, the proportion of females in the patients with CTN- SSD was higher than that in the group of CRSsNP (73.58% vs 63.36%, P < .001).
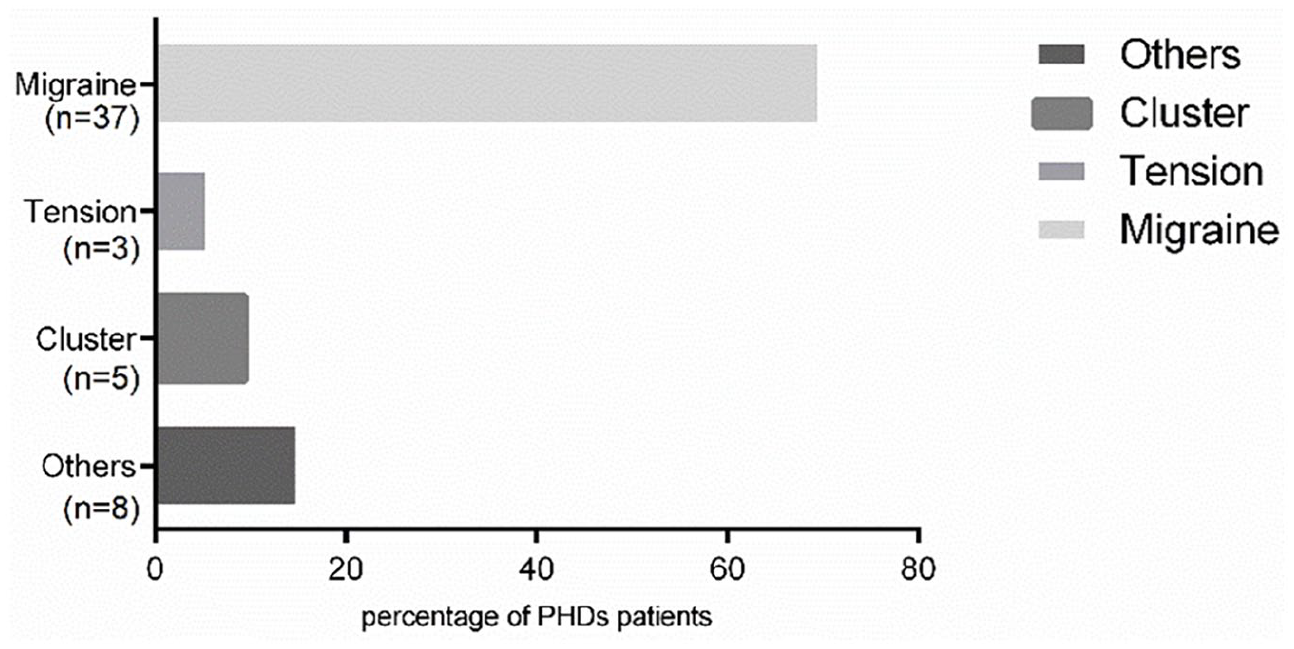
Classification of headache disorders in CTN-SSD group. CTN-SSD, CT-negative symptomatic sinonasal disorders.
Demographic Information of Patients With CTN-SSD and CRSsNP.
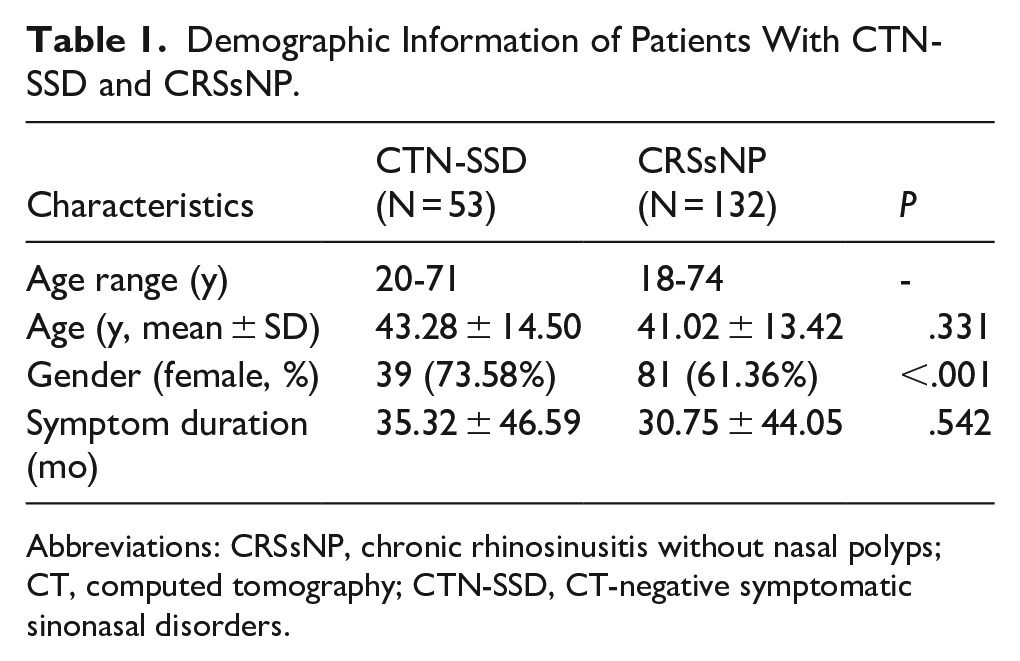
Abbreviations: CRSsNP, chronic rhinosinusitis without nasal polyps; CT, computed tomography; CTN-SSD, CT-negative symptomatic sinonasal disorders.
The Incidences of Different Signs and Symptoms in the 2 Groups
The incidences of primary and secondary sinusitis symptoms differed significantly between the 2 groups. Posterior rhinorrhea (49.05% vs 31.81%, P = .028, w = 0.162) and headache/facial pain (100% vs 45.45%, P < .001, w = 0.505) were more common in patients with CTN-SSD, while congestion (54.71% vs 81.81%, P < .001, w = 0.279), anterior rhinorrhea (30.18% vs 59.09%, P < .001, w = 0.261), and hyposmia (11.32% vs 59.09%, P < .001, w = 0.436) were more prevalent in patients with CRSsNP. Nasal mucosal swelling and mucoid secretions were present in both patients with CTN-SSD and CRSsNP. Although there was no significant difference in the presence of mucoid secretions (15.09% vs 12.12%, P = .586, w = 0.039) between the 2 groups, purulent secretions were only present in CRSsNP patients (9.84%, P = .021, w = 0.174). Notably, mucosal swelling was present in a significantly-greater proportion of CRSsNP patients (100%) than of patients with CTN-SSD (79.24%), with a moderate effect size (P < .001, w = 0.394). All these are shown in Table 2.
Incidences of Different Signs and Symptoms in Patients With CTN-SSD and CRSsNP.
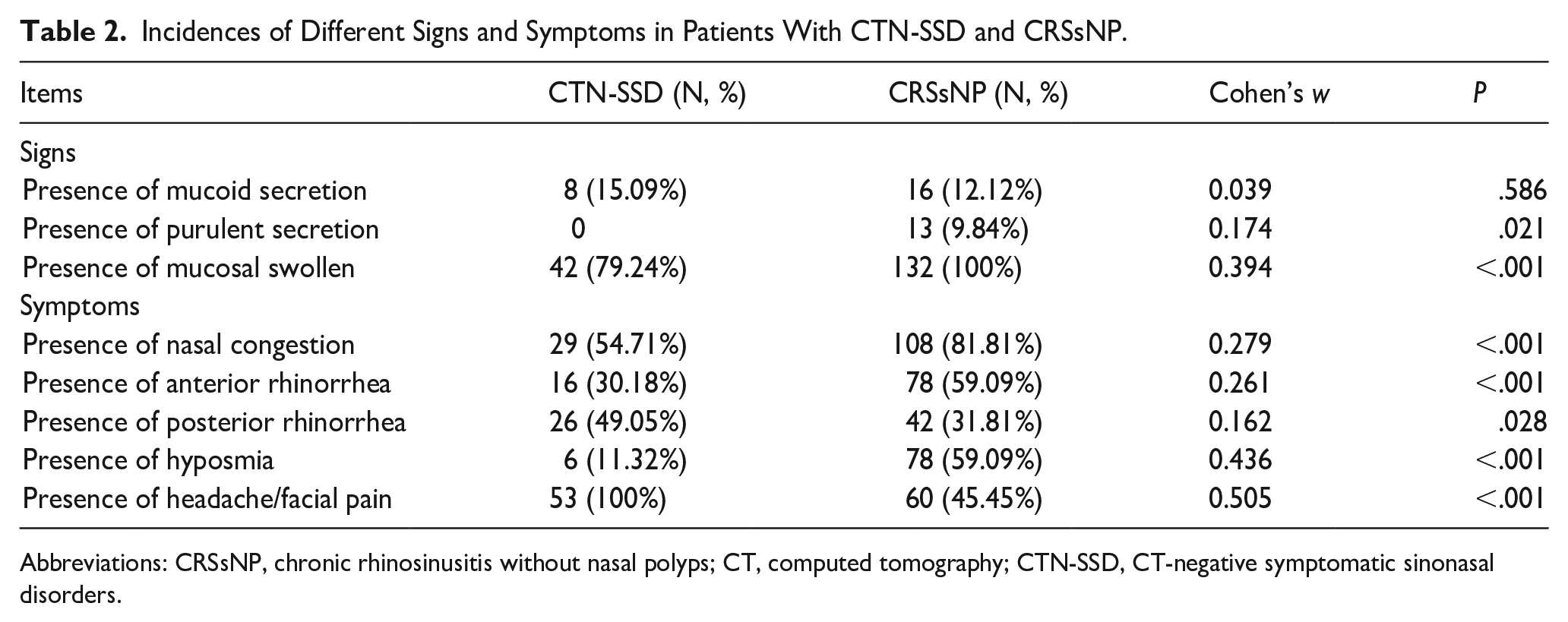
Abbreviations: CRSsNP, chronic rhinosinusitis without nasal polyps; CT, computed tomography; CTN-SSD, CT-negative symptomatic sinonasal disorders.
Subjective and Objective Scores in the 2 Groups
Compared with CTN-SSD, CRSsNP patients had significantly-higher Lund-Kennedy Endoscopic Scoring System (LKES) scores (P < .001, d = 0.53) and LMKS scores (P < .001, d = 2.47). There was no significant difference in SNOT-22 scores (P = .063, d = −0.30) and total VAS scores of the symptoms (P = .077, d = 0.29). The scores of nasal congestion (P < .001, d = 0.69), anterior rhinorrhea (P < .001, d = 0.88), and hyposmia (P < .001, d = 0.60) in patients with CRSsNP were higher than those in patients with CTN-SSD. However, the scores of posterior rhinorrhea (P = .044, d = −0.31) and headache/facial pain (P < .001, d = −2.00) were higher in the CTN-SSD group.
Patients with CTN-SSD had significantly-higher aural/facial subdomain scores (P < .001, d = −0.92) and psychological subdomain scores (P < .001, d = −6.48) than in CRSsNP patients. The sleep subdomain score of CTN-SSD was higher than in CRSsNP patients, but there was no significance (P = .102, d = −0.14). Moreover, CRSsNP patients had significantly-higher nasal subdomain scores (P < .001, d = 0.94). All these are shown in Table 3.
Subjective and Objective Scores in Patients With CTN-SSD and CRSsNP.
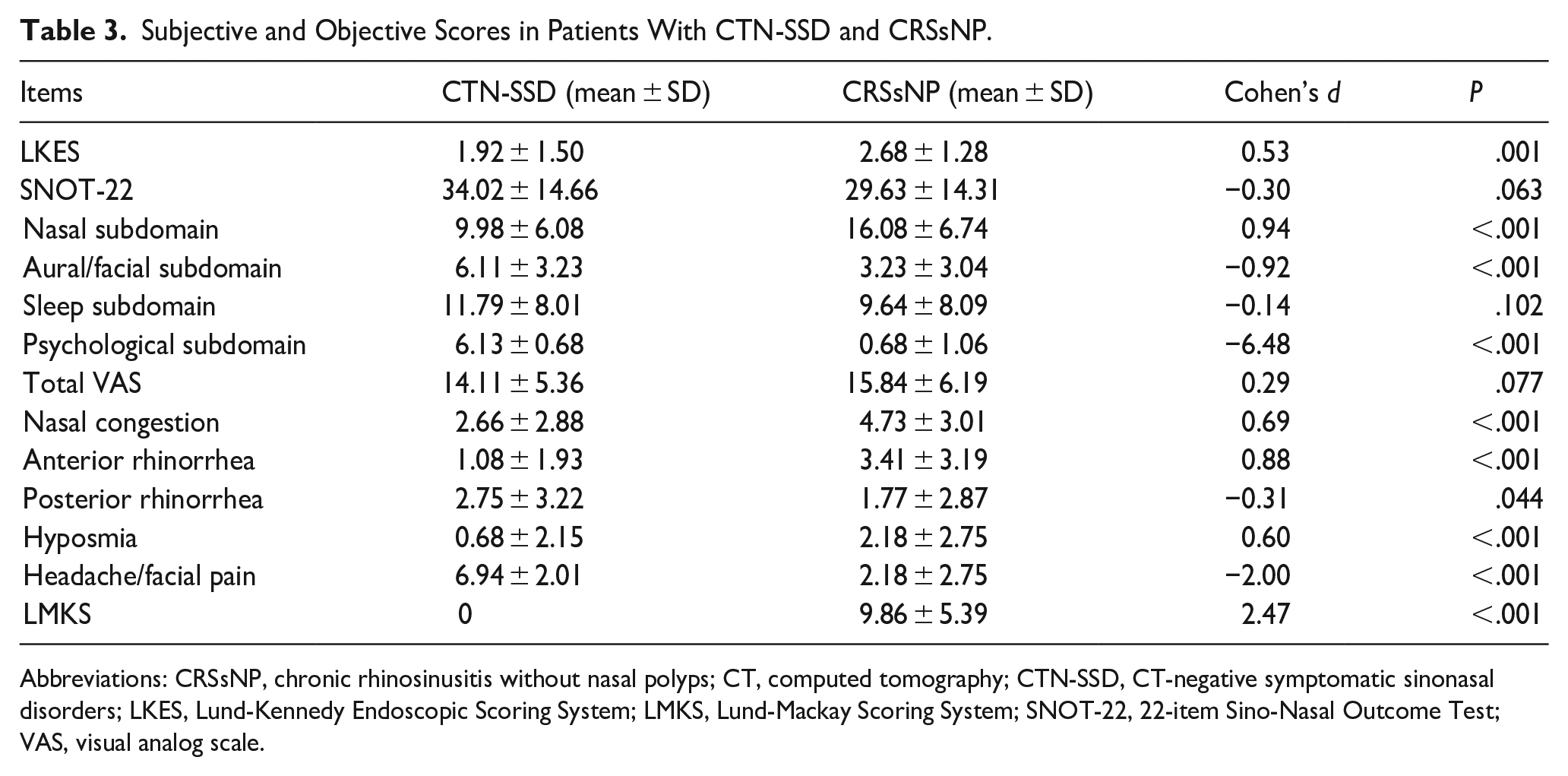
Abbreviations: CRSsNP, chronic rhinosinusitis without nasal polyps; CT, computed tomography; CTN-SSD, CT-negative symptomatic sinonasal disorders; LKES, Lund-Kennedy Endoscopic Scoring System; LMKS, Lund-Mackay Scoring System; SNOT-22, 22-item Sino-Nasal Outcome Test; VAS, visual analog scale.
Discussions
According to European Position Paper on Rhinosinusitis and Nasal polyps (EPOS), CRS is sorted into 2 subtypes, CRSwNP and CRSsNP. It is simple to differentiate the 2 sorts. But for CRSsNP, CT scanning of paranasal sinus is considered to be the gold standard. Many patients do not take CT scans due to the cost factor and radiation exposure. The diagnosis of CRSsNP always relays on symptoms and patients are often given antibiotics before images are available.
Nasal symptoms can present in PHDs and may be misdiagnosed as CRSsNP, resulting in inappropriate medical treatments. As one of the most common subgroup of PHDs, migraine with nasal symptoms has been widely studied. The nasal symptoms of migraine are thought to be the central activation of the parasympathetic tracts caused by neurogenic inflammation. 8 Many patients with migraine reported different nasal symptoms. Eighty-two percent complained of facial pain, 63% complained of nasal obstruction, and 40% complained of rhinorrhea at the first visit to the office. 5 These nasal symptoms are related to anatomy and physiology, consisting of trigeminal autonomic reflexes. Migraineurs with CRS symptoms suggest that 1 or more branches of the trigeminal nerve are chronically upregulated, resulting in cranial autonomic nerve hyperactivity through the trigeminal autonomic reflex, and leading to sinus symptoms such as facial pain, nasal congestion, and rhinorrhea. When both the trigeminal and autonomic nervous systems of the brainstem are activated, a wide variety of symptoms can occur that can easily be misinterpreted as CRS. 14 Therefore, patients with migraine were always mislabeled as having CRS. Misdiagnosis puts these patients at the risk of inappropriate treatments and procedures, and delays proper treatment of their headache. 15
Not all CRS patients present with nasal discharge. 1 Although different nasal discharge may be present, purulent or mucoid was more common. Usually, the physical examination does not make a substantial contribution in identifying the diagnosis of CRS, because the findings can be quite subtle and nonspecific. 16 Hyperemic and swollen nasal mucosa may be present. 17 Purulent secretions in the middle nasal meatus often indicate bacterial infection of sinuses. 18 Congestion of the nasal mucosa can occur during the onset of headache in patients of PHDs. Endoscopic nasal mucosal edema during migraine attacks was reported. 19 The changes in nasal resistance between onset and non-onset periods in migraine patients were significant. 20 These findings are consistent with the high endoscopic scores and the presence of nasal congestion observed in patients with CTN-SSD in our study, likely representing active episodes due to neurogenic-mediated inflammation. 19 Devyani found that the most common nasal symptom of PHDs was posterior rhinorrhea in addition to nasal obstruction. 21 This observation aligns with our study findings that CT-negative cases predominantly present with posterior rhinorrhea as the cardinal symptom, thereby supporting the hypothesis that CTN-SSD may likely represent the nasal manifestations of PHDs. The nasal symptoms and signs in CRS are thought to be the result of immunologic mechanisms, while these in patients with PHDs are considered to be the central activation of parasympathetic tracts caused by neurogenic inflammation. 19
The SNOT-22 is widely used to evaluate the severity of quality of life in patients with CRS. SNOT-22 is not necessary in the diagnosis of CRS. However, it plays a very important role in the identification of PHDs. Daniel found the SNOT-22 may be used to distinguish PHDs from CRS based on severe aural/facial and sleep subdomains scores. In addition, patients with CRS had more severe nasal subdomain scores. 22 The prevalence rates of sleep disorders, anxiety, and depression in patients with PHDs were higher than those in the general population. 23 Patients with PHDs are more prone to anxiety and other emotional disorders, while those with CRS had more serious nasal symptoms. For patients with CRS, nasal obstruction was significantly associated with poorer sleep quality. 24 Therefore, both PHDs and CRS are associated with sleep disorders. Prior studies had described many audio vestibular symptoms associated with PHDs, including dizziness, aural fullness, and otalgia, which are the items of aural/facial subdomain. 25 Patients with PHDs reported more severe symptoms in the aural/facial and emotional portions of this survey. Meanwhile, patients with CRS reported more severe nasal portion of the SNOT-22 survey. Although SNOT-22 are not routinely used in otolaryngology settings, the possibility of PHDs should be considered when the patient has severe aural/facial and emotional issues. Therefore, before performing a sinus CT scan on a patient, if the aural/facial and psychological subdomain scores of the SNOT-22 are high, there should be a high suspicion of PHDs to avoid inappropriate therapies.
A study has shown that 35% to 50% of CRSsNP patients had normal sinuses. 26 Headache/facial pain symptoms are generally not strongly associated with positive CT findings, whereas nasal obstruction and purulent nasal discharge are often correlated with positive CT results. 27 A study found that by removing facial pain, it was able to increase specificity without a concordant loss in sensitivity in the diagnosis of CRS. 28 Traditionally, patients presenting with sinus symptoms have primarily received empirical antibiotic therapy. The radiation exposure and economic considerations of CT scans make them less practical. Another strategy involves performing an initial CT screening for these patients. This diagnostic approach may ultimately reduce health care costs, avoid unnecessary antibiotic prescriptions, and facilitate timely referral of patients to more appropriate specialties, such as neurology, and/or pain management. For ENT specialists, when traditional treatments fail or sinus CT scans are negative, it is important to consider the possibility of PHDs and promptly refer the patient for further evaluation.
Patients with PHDs always had severe facial pain as the predominant symptoms. CRSsNP patients had more severe nasal subdomain scores of SNOT-22 and worse endoscopic and CT appearances. 22 Patients with PHDs reported more severe symptoms in the aural/facial and emotional portions of the survey. Our research suggests that when patients’ primary symptoms are headaches/facial pain and/or postnasal drip rather than nasal congestion and purulent nasal discharge, timely CT scans should be considered to rule out the possibility of misdiagnosis, especially when the aural/facial and emotional sections of the SNOT-22 show higher scores. In addition to sinus symptoms, patients with PHDs such as migraine often have other typical features, such as throbbing headache and sensitivity to sound. 29 These are helpful to rule out the diagnosis of CRSsNP. A critical limitation is that patients with CTN-SSD in this cohort may in fact have cephalic disorders mimicking sinonasal inflammation. Our protocol did not include a therapeutic trial of triptans or neuromodulators to test this hypothesis.
Conclusions
Patients with CTN-SSD often meet migraine criteria, predominantly female, presenting with postnasal drip and headache/facial pain. In contrast, patients with CRS exhibit anterior rhinorrhea, nasal obstruction, and olfactory dysfunction. This distinction emphasizes the need to differentiate migraine-related nasal symptoms from CRS, particularly in females without sinus abnormalities on CT imaging, to optimize diagnostic accuracy and treatment strategies.
Footnotes
Ethical Considerations
Ethics approval was obtained from the Medical Ethics Committee of Peking University People’s Hospital.
Author Contributions
Zhimin Xing designed the study. Yan Liu analyzed the data and wrote the manuscript. Xiaohong Peng, Xiaopei Yuan, Congli Geng, and Min Wang collected the data.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this article.