
Abstract
Foreign body aspiration is commonly observed in young children. Adults represent about 0.4% of all reported cases. This article reports a unique instance of a 32-year-old gentleman who accidentally aspirated his dental bridge while sleeping. It is rare to see asymptomatic instances exist, as happened in our case. A 32-year-old man presented to the emergency room with complaints of losing his dental bridge when he woke up from sleep. He did not show any other symptoms. Computed tomography scans showed a dental bridge stuck in the left bronchus. The patient underwent a flexible bronchoscopy and then a rigid bronchoscope in a more specialized center to extract the obstacle. The dental bridge was removed successfully. The significance of this case lies in emphasizing the need to consider less conventional sources of airway blockages and the challenges involved in treating such situations.
Introduction
Foreign body aspiration (FBA) is defined as the accidental inhalation of solid or semi-solid material into the lower respiratory tract. 1 While this condition is most frequently reported in young children (particularly aged 1-3 years), it is rarely observed in adults.1,2 Adults account for approximately 0.4% of all tracheobronchial foreign body (TFB) aspiration cases. 3 Risk factors include impaired consciousness due to alcohol intoxication, sedative or hypnotic drug use, neurological disorders (e.g., epilepsy or neurodegenerative diseases), and altered mental status. 4 The most common presenting symptoms are cough and dyspnea. 4 Delayed diagnosis of TFBs may lead to severe complications, including pneumonia, bronchiectasis, or even lung resection. 4 This report describes a unique case of a 32-year-old man who asymptomatically aspirated a dental bridge after waking up from sleep, which was subsequently managed at a tertiary academic medical center.
Case Presentation
A 32-year-old Syrian man presented to the ENT emergency department. The patient reported losing his dental bridge during a coughing episode immediately after waking. He denied symptoms such as dysphagia, shortness of breath, chest pain, hemorrhage, nausea, or fever. His medical, surgical, and family histories were unremarkable, with no regular medications or smoking. Vital signs were within normal limits. Physical examination revealed decreased breath sounds in the left lung field, with no signs of dyspnea. The patient was evaluated and scheduled for intervention on the day of presentation. Chest X-rays (Figure 1) and Computed tomography (CT) imaging (Figure 2) confirmed a dental bridge, comprising several teeth, lodged in the left main bronchus. The diagnosis of dental bridge aspiration was established radiographically; however, the absence of typical symptoms remained unexplained.
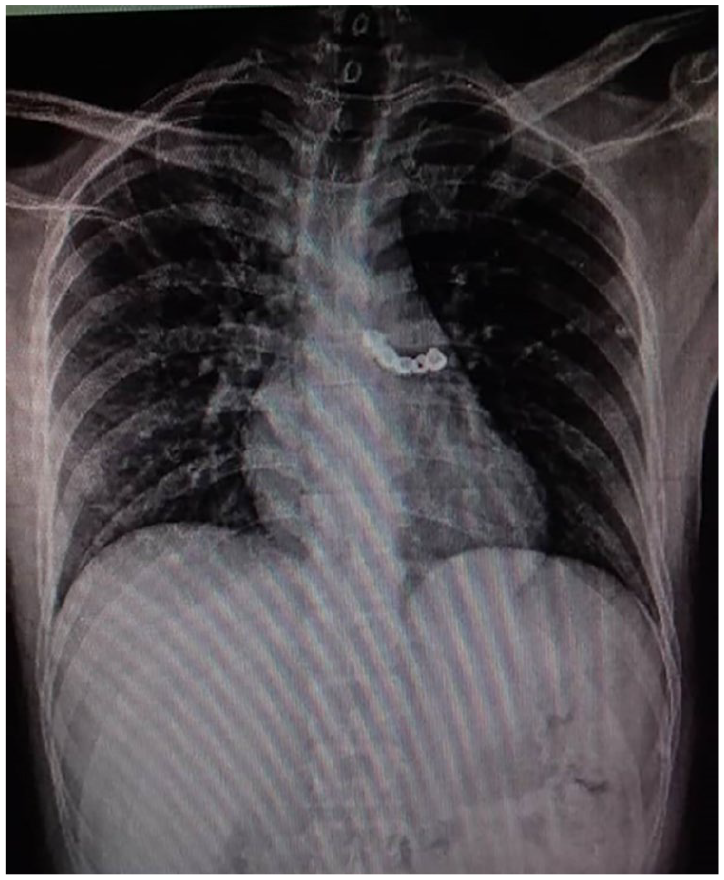
Aspirated dental bridge in left main bronchus. Posteroanterior (PA) chest X-ray demonstrates a radiopaque dental prosthesis lodged in the left main bronchus.
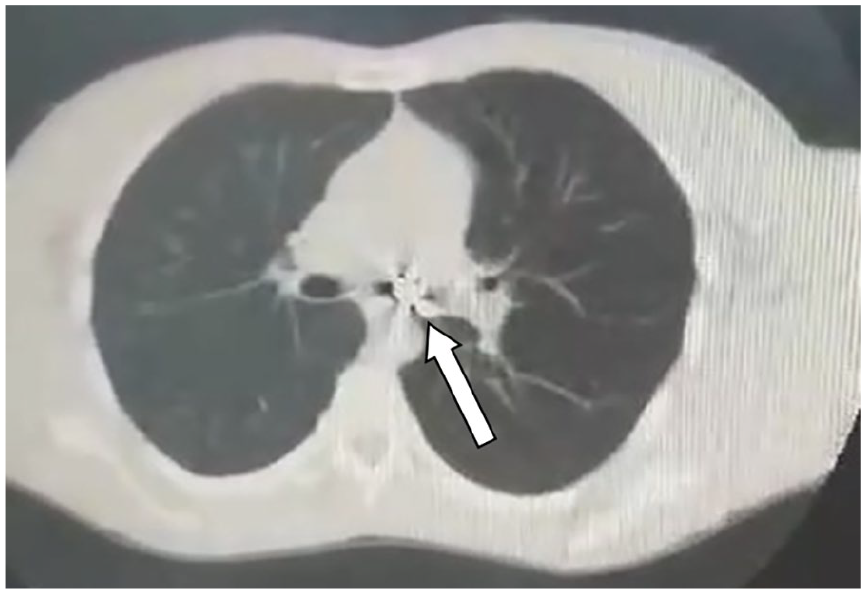
Axial chest CT—impacted dental bridge. Non-contrast axial CT image demonstrates a dental bridge lodged within the lumen of the left main bronchus (arrow). CT, computed tomography.
The patient was prepared for intervention, with no significant pre-procedural considerations required due to his unremarkable medical history and lack of chronic medications. Initially, an attempt was made to remove the dental bridge using a flexible bronchoscope at a nonspecialized facility; however, this was unsuccessful. Consequently, the patient was transferred to a tertiary academic hospital for further management.
Under general anesthesia, a rigid bronchoscopy was performed by an experienced bronchoscopist. The dental bridge was visualized within the left main bronchus, carefully grasped, and extracted through the vocal cords without complications (Figure 3). Standard instruments and techniques were employed throughout the procedure.

Dental prosthesis post-extraction. This image shows the dental prosthesis recovered from the patient’s bronchus using rigid bronchoscopy, demonstrating the object’s structure and size following removal.
Postoperatively, the patient was maintained on a liquid diet for 2 hours and monitored closely. Vital signs remained stable, with no evidence of respiratory distress or oxygen desaturation. He was discharged later that day in stable condition. During a 9-month follow-up period, no complications (e.g., infection, airway injury, or delayed symptoms) were reported.
Discussion
FBA occurs when solid or semi-solid material is accidentally inhaled into the lower respiratory tract. While the esophagus and upper respiratory system share a common anatomical pathway, making ingested food particles the primary source of foreign bodies, aspiration into the respiratory tract can occur due to factors such as impaired consciousness, neurological conditions (e.g., seizures), regurgitation, or intentional object misplacement. 1 At our institution, accidental inhalation of foreign bodies is relatively common and carries significant morbidity, particularly in children who aspirate small objects such as seeds or nuts. This case underscores the importance of recognizing unconventional sources of airway obstruction and the challenges in managing such scenarios. For instance, retrieving the smooth-surfaced dental bridge proved difficult with standard instruments, necessitating multiple attempts under specialized care.
Tracheobronchial FBA is most prevalent in children under 5 years of age; however, incidence also rises among older adults and individuals with neurological disorders. 4 The right bronchial tree, particularly its lower lobe and intermediate branches, is the most frequent site of aspiration due to its anatomical verticality. 5 However, as demonstrated in this case, foreign bodies may lodge in the left mainstem bronchus. Commonly aspirated dental materials include teeth, fillings, crowns, bridges, and orthodontic appliances. 6 Symptoms vary widely depending on the object’s size, shape, composition, and location. While acute presentations typically involve coughing, choking, or dyspnea, asymptomatic cases, as seen here, may occur if the foreign body causes partial obstruction or minimal inflammation. 7
The patient’s age may also attenuate symptom severity, contributing to delayed diagnosis. Evaluation of suspected FBA begins with posteroanterior and lateral chest X-rays. For precise localization or characterization of radiolucent objects, CT is often indicated. 8
Management depends on the patient’s clinical stability. In urgent cases, immediate bronchoscopic intervention is warranted. 1 While rigid bronchoscopy remains the primary approach for removing aspirated foreign bodies, flexible fiberoptic bronchoscopy offers an alternative. Its key advantage is the ability to use local anesthesia with sedation. However, limitations include smaller instruments and a higher risk of dislodging the foreign body further into the airway. 9
Bolden et al. 10 describe a case of an 82-year-old male who aspirated a dental bridge into his left mainstem bronchus during dental cleaning, presenting with minimal symptoms. After failed conservative management, flexible bronchoscopy under general anesthesia successfully retrieved the intact bridge via a urology basket, resulting in only minor mucosal edema. This demonstrates flexible bronchoscopy’s efficacy for retrieving select aspirated dental prostheses and highlights the essential need for preventive measures (e.g., rubber dams) during dental procedures.
To minimize the reported risk of S. epidermidis sepsis secondary to mucosal injury during dental prosthesis retrieval, 11 optimal techniques involve utilizing a rigid bronchoscope of maximal diameter and ensuring the foreign body remains contained within its lumen during removal. 9 Failure to remove a foreign body using bronchoscopic techniques necessitates surgical removal by thoracotomy. 12 Post-procedure corticosteroid use to reduce subglottic edema remains controversial and is not routinely recommended. 9 Antibiotics should only be administered if concurrent respiratory infection is evident. 9
Conclusion
FBA is not a rare emergency case, but it is rare in adults and the left bronchus with mild symptoms. In addition, dental bridge is rarely aspirated. There are so many various symptoms, so it is important to evaluate vital signs directly and strictly with a detailed history. Many procedures can be performed for the extraction of the foreign body, but the most important thing is to be done as fast as possible. Usual symptoms sometimes do not exist, so we have to take any complaint seriously and do the required investigations.
Footnotes
Acknowledgements
None.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to Participate
Written informed consent was obtained from the patient for the publication of this case report, including all accompanying medical information and images.
Author Contributions
Hossam Alhraki: Conceptualization, Investigation, Writing – Original Draft, Visualization. Yasser AlGhabra: Data Curation, Formal Analysis, Writing – Review & Editing, Writing (Corresponding Author). Ahmad Kammasha: Project Administration, Validation. Ahmad Alharran: Investigation. Abdulmajeed Yousfan: Supervision.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the author or corresponding author upon reasonable request.