
Abstract

Significance Statement
Necrotizing soft tissue infection (NSTI) in the fascial layers of the neck is a feared and complicated pathology that requires prompt diagnosis and action. We present a case of aggressive polymicrobial NSTI secondary to a peritonsillar abscess in a patient with no risk factors and with a low laboratory risk indicator for necrotizing fasciitis. This report highlights the ongoing need for further research into the risk factors, diagnosis, and treatment of cervical necrotizing fasciitis.
Case Report
The patient is an 81-year-old man with a brief medical history of hypertension and cerebrovascular accident who presented to an outside hospital with a 2-day history of sore throat, neck pain/swelling, and difficulty breathing/swallowing. He was intubated at an outside hospital for concern of angioedema with a difficult intubation documented requiring multiple attempts. CT neck showed a large right parapharyngeal/peritonsillar abscess (Figure 1) with a large volume of air surrounding the infrahyoid strap musculature (Figure 2) extending to the thoracic inlet. On exam, anterior neck fullness with crepitus was noted. His lab work showed WBC 6.6 cells/µL, hemoglobin 14.0 g/dL, C-Reactive Protein (CRP) 18.48 mg/L, sodium 138 mEq/L, creatinine 0.9 mg/dL, glucose 129 mg/dL, lactic acid 1.9 mg/dL, and neutrophil to lymphocyte ratio (NLR) of 12.2. He was brought to the operating room (OR) emergently for direct laryngoscopy and neck exploration. Findings intraoperatively included a right peritonsillar/parapharyngeal abscess and extensively necrotic strap musculature with dishwater fluid and purulence throughout levels 2 to 4 bilaterally. Treatment was initiated with Unasyn and Clindamycin. Cultures grew Klebsiella aerogenes, Streptococcus constellatus, and Parvinomonas micra. The patient was brought back to OR 48 hours later for second look and was found to have grossly necrotic esophageal and constrictor musculature with a sizable pharyngeal fistula into the neck, as well as obvious extension into the mediastinum. Discussion was held with the family intraoperatively, and a decision was made to designate the patient comfort measures only. He was terminally extubated 24 hours later.
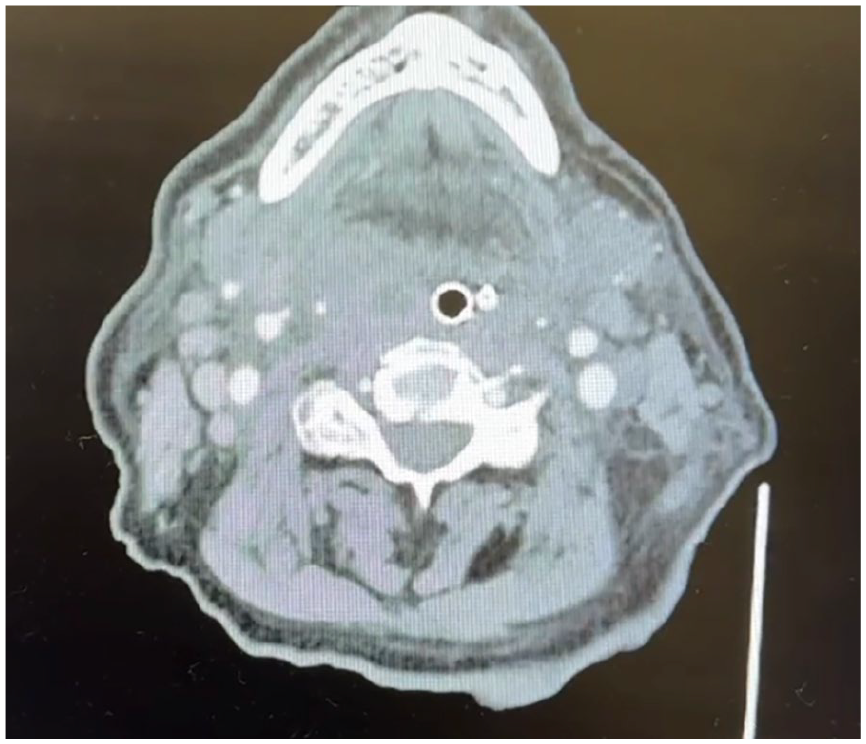
This image is an axial cut of the patient’s CT neck showing a right peritonsillar abscess.
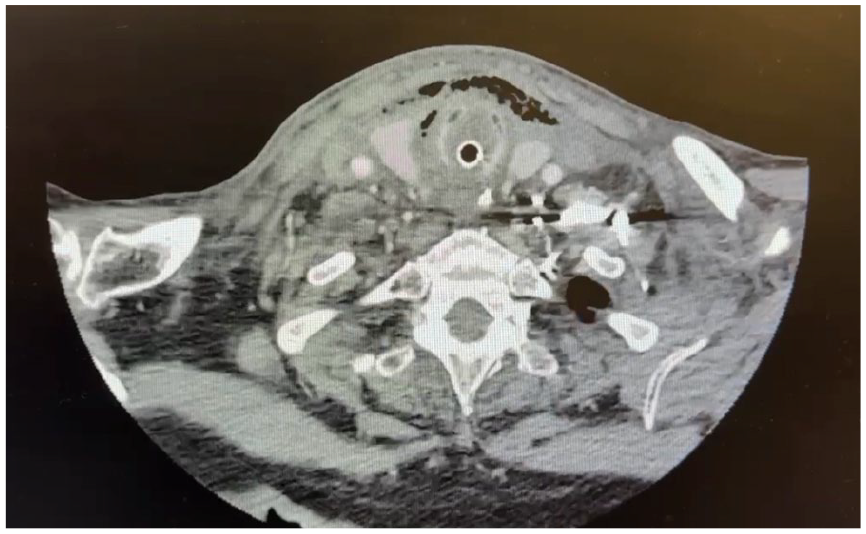
This image is an axial cut of the patient’s CT neck showing subcutaneous emphysema surrounding the thyroid cartilage and strap musculature.
Cervical necrotizing soft tissue infections (NSTIs) are rapidly progressive and potentially fatal infections of the head and neck with an estimated incidence of 2 cases per 1 million individuals, 1 accounting for 1% to 10% of all NSTIs. 2 Diabetes mellitus, renal failure, and obesity are the only comorbidities known to be associated with necrotizing fasciitis-related deaths. 3 Odontogenic etiology (47.04%) is most likely, followed by pharyngolaryngeal (28.34%) or tonsillar/peritonsillar (6.07%) sources. 4 In a sample of 16 patients, necrotizing fasciitis secondary to peritonsillar abscess demonstrated increased mortality compared to odontogenic infections. 5
Necrotizing fasciitis is a challenging diagnosis early in the disease course, as it presents similarly to other soft tissue infections. The laboratory risk indicator for necrotizing fasciitis (LRINEC) is a diagnostic tool based on serum values for CRP, total white count, hemoglobin, sodium, creatinine, and glucose. Wong et al originally proposed this method with a cutoff score over 6 for differentiating NSTI from other infections, demonstrating a positive predictive value of 92.0% and a negative predictive value of 96.0%. 6 Recent studies have reported limitations in the usage of LRINEC in isolation; an 18-year investigation calculated sensitivity of 59% and specificity of 82%, with positive and negative predictive values of 57% and 84%, respectively. 7 The prognostic efficacy of LRINEC is known to vary widely based on the anatomical region of infection,8,9 with mixed assessments in the evaluation of exclusively cervical NSTIs.10-14 Still, LRINEC ≥6 holds the most diagnostic relevance in necrotizing fasciitis of the head and neck with values for sensitivity, specificity, and negative predictive value established at 75%, 85%, and 98%, respectively. 15 Variability across studies suggests that cervical NSTI can be a difficult diagnosis despite screening tools. Our patient’s LRINEC score was calculated at 4 on presentation and 5 on the day of terminal extubation, demonstrating low efficacy as both a screening and prognostic tool in this case.
The NLR is an alternative biomarker related to immune response with prognostic value in necrotizing fasciitis, sepsis, and all-cause mortality.16-18 NLR values over 15 have demonstrated the highest efficacy for differentiating cervical NSTI from other soft tissue infections.19,20 In a sample of 14 oro-cervical necrotizing fasciitis and 217 severe oro-cervical cellulitis cases, NLR ≥15.3 had a sensitivity of 92.9%, with LRINEC ≥6 demonstrating a sensitivity of 71.4%. 20 Additional studies are needed to evaluate NLR against LRINEC; however, this represents another diagnostic adjunct for cervical NSTI. Our patient’s NLR was below 15 at 12.2.
Necrotizing fasciitis is a rare but well-described complication of peritonsillar abscess, with few cases involving immunocompetent individuals. Prompt diagnosis, operative debridement, and initiation of antibiotics are critical for treating necrotizing fasciitis. The threshold should be very low for surgical intervention, including interval debridement until viable, healthy tissue is evident. Delayed intervention and restricted debridement are associated with 9 times greater mortality and over 7 times increased relative risk of death, respectively.21,22 This is crucial in cervical NSTI, where progression to descending mediastinitis is associated with a significantly increased mortality rate. 4 Overall, evidence suggests that LRINEC and NLR can supplement the diagnosis of cervical NSTI in many cases. Further investigations should confirm the cutoff value for NLR. Our case represents a rapidly progressive and fatal infection with atypical response in laboratory markers, emphasizing that clinical judgment remains paramount.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Written informed consent to present and publish this case report was obtained from the patient’s legally authorized representative.
Author Contributions
M.M. contributed by drafting the manuscript and conducting a literature review. T.P. contributed by drafting the manuscript. D.R. assisted in conducting literature review. C.M. conducted literature review and assisted in drafting manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data pertaining to this report is available upon request, so long as it is within HIPAA guidelines.