
Abstract
Laryngeal abscesses (LA), though rare in the modern antibiotic era, remain potentially life-threatening, especially when associated with airway obstruction. This case report presents a 55-year-old immunocompetent female, a heavy smoker and alcohol user, who developed a spontaneous supraglottic laryngeal abscess masquerading as a malignant pathology. The patient presented with odynophagia, dysphagia, and dysphonia, along with inspiratory stridor. Fiberoptic endoscopy revealed a mass in the left aryepiglottic fold and ipsilateral vocal fold immobility. Imaging studies demonstrated a supraglottic formation with necrotic features and bilateral cervical lymphadenopathy. After 3 days of intravenous antibiotics and corticosteroids, the patient’s symptoms improved, and she was discharged on oral antibiotics. At 14 days, endoscopy confirmed the resolution of the aryepiglottic fold swelling and normal vocal fold mobility. The clinical evolution, including the patient’s response to conservative treatment coupled with the laryngeal status at follow-up, ultimately confirmed the diagnosis of a laryngeal abscess rather than a malignancy. The case underscores the importance of considering laryngeal abscess in the differential diagnosis for patients presenting with persistent symptoms and highlights the need for thorough diagnostic evaluation, including imaging and biopsy when malignancy is suspected. Furthermore, it emphasizes the potential effectiveness of conservative treatment with antibiotics, particularly when airway management and timely intervention are prioritized, thus reducing the need for invasive surgical procedures.
Keywords
Introduction
Laryngeal abscesses (LA), though rare in the modern antibiotic era, remain potentially life-threatening due to the risk of airway compromise. Historically, these infections were more common and carried a nearly universal fatality rate before the advent of antibiotics. 1 Advances in antimicrobial therapy have significantly reduced their incidence and associated mortality.
LA are most frequently reported as a complication of acute supraglottitis. 2 The incidence of epiglottic abscesses in children, primarily caused by Haemophilus influenzae, has significantly decreased since the introduction of the vaccine in the 1980s. 3 Suppuration in the posterior larynx is rare and typically linked to trauma or instrumentation. 2 In adults, the most common type occurs in the epiglottis, typically as a complication of acute supraglottitis, although it may also result from infection of preexisting cysts. 4 Epiglottic abscesses usually form in the lingual portion due to the looser submucosal attachments, while subglottic abscesses are extremely rare. 4
This case is notable for the spontaneous formation of a supraglottic laryngeal abscess in an immunocompetent adult mimicking advanced T-stage supraglottic carcinoma, which resolved with conservative empiric antibiotherapy. It contributes to the scientific literature by emphasizing the potential for non-surgical management in selected cases and by underscoring the diagnostic challenges in distinguishing LA from malignancies as well as the evolving understanding of their etiologies and treatment strategies.
Case Report
An otherwise healthy 55-year-old female, a heavy smoker and alcohol user, presented with a 4-day history of odynophagia, dysphagia, and dysphonia. The patient’s past surgical history was unremarkable. On initial assessment upon admission, she exhibited inspiratory stridor with retractions and was afebrile. Flexible fiberoptic endoscopy, as shown in Supplemental Video 1, revealed a bulging mass of the left aryepiglottic fold with ipsilateral vocal fold immobility in a paramedian position and a yellowish cystic lesion in the left arytenoid area (Figure 1A).
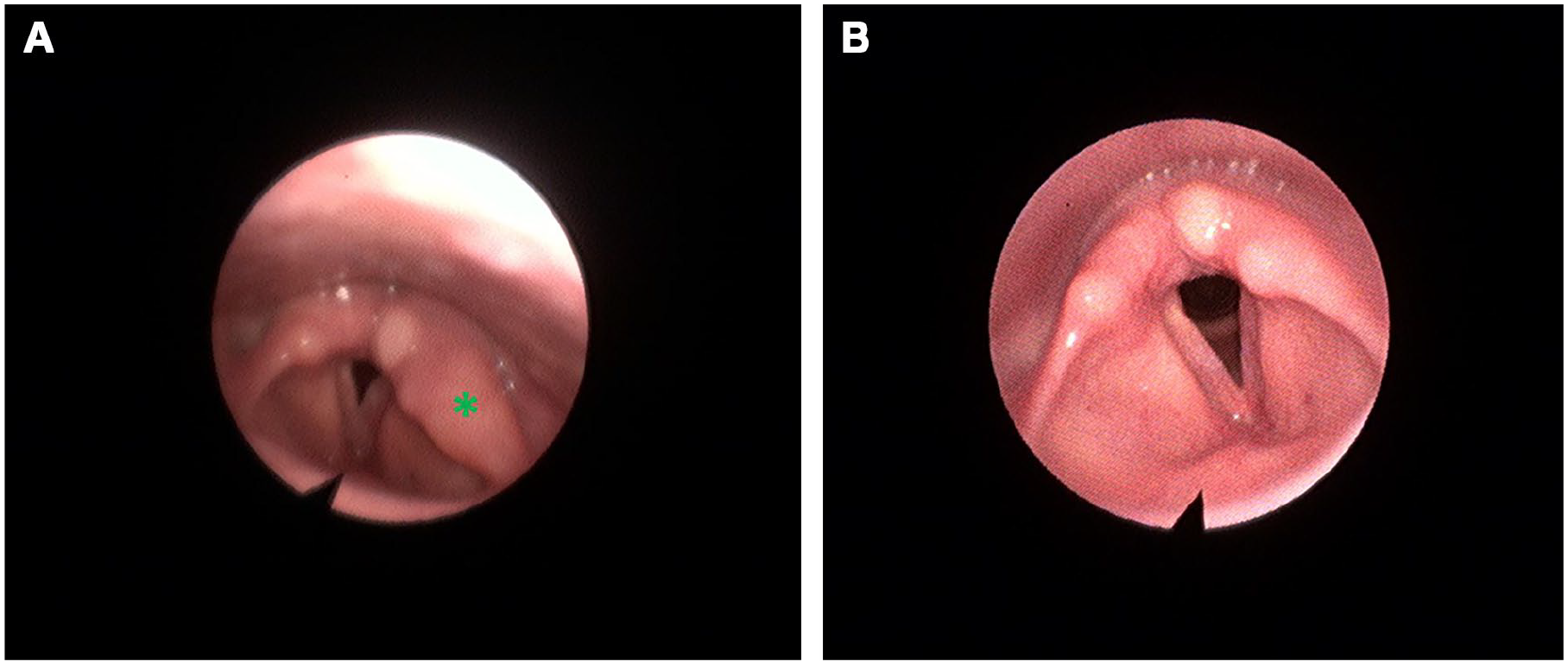
Flexible fiberoptic endoscopic images. (A) Flexible fiberoptic endoscopy image during respiration, at initial presentation, revealing a prominent mass (*) in the left aryepiglottic fold. (B) Follow-up flexible fiberoptic endoscopy image during respiration, at 14 days, showing complete resolution of the mass.
Cervical computed tomography (CT) with contrast (Figure 2A and B) displayed a left supraglottic mass with anterior transglottic and postcricoid extension, accompanied by bilateral cervical lymphadenopathy. The lesion presented a necrotic-appearing component, possibly secondarily infected. A complementary thoracic CT demonstrated no underlying etiology for the unilateral vocal fold immobility. The patient refused diagnostic direct laryngoscopy and was therefore managed conservatively with a 3-day empiric course of intravenous amoxicillin-clavulanic acid and corticosteroids, during which odynophagia subsided and the aryepiglottic fold mass showed a minimal reduction.
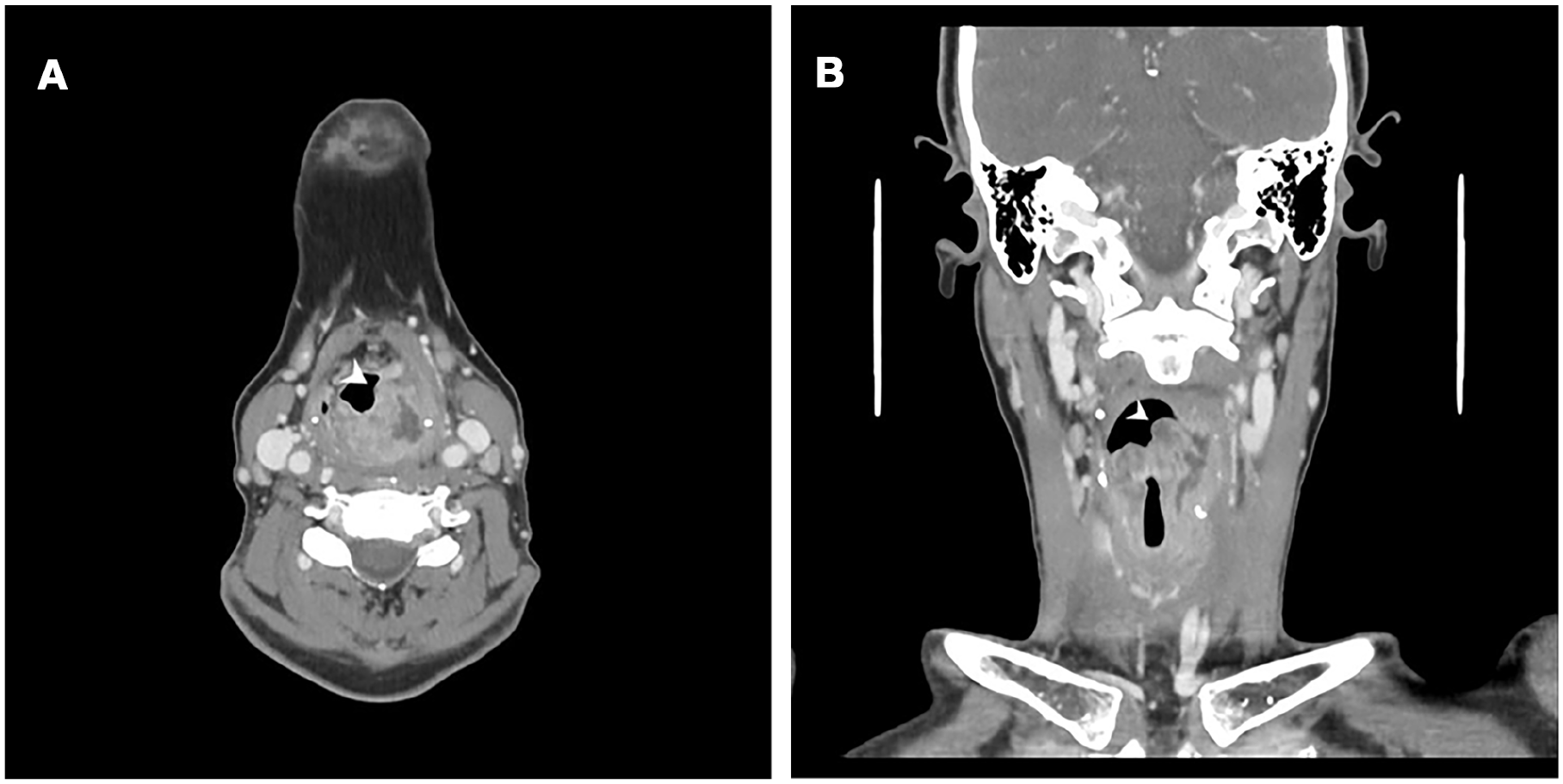
Computed tomography images. Axial slice (A) and coronal reconstruction (B) of the same study, demonstrating a tissue mass in the left aryepiglottic fold (arrowhead), associated with an abscess extending into the supraglottic, glottic, and subglottic spaces.
A follow-up was proposed to assess the laryngeal status and, if necessary, to consider microlaryngoscopy with biopsy under general anesthesia for further evaluation. At the fourteen-day follow-up, as shown in Supplemental Video 2, bilateral normal vocal fold mobility was observed, along with the complete resolution of the left aryepiglottic fold swelling (Figure 1B). The patient declined further suspension microlaryngoscopy with excision of the cystic lesion in the left arytenoid area.
Discussion
Traditionally, typhoid fever was the primary etiology of LA, with other systemic infections such as measles, tuberculosis, actinomycosis, syphilis, gonorrhea, and diphtheria also contributing.1,4 During the 1930s, the incidence of typhoid-related cases declined, while foreign body injuries and pharyngotonsillitis emerged as leading causes of laryngeal suppuration. 4 The introduction of penicillin in the mid-1940s significantly reduced the prevalence and severity of these infections, making LA relatively rare. 1 As primary infectious causes diminished, other etiologies, including chronic inflammatory conditions such as histoplasmosis and sarcoidosis, trauma (mechanical or iatrogenic), irradiation, malignancy, airway instrumentation, and ingestion of foreign bodies, became more prominent.1-5
In addition, cases have been described in patients with laryngocele, thymic cyst, bronchogenic cyst, thyroid cyst, branchial arch anomalies, thyroiditis, and even following injection laryngoplasty.1-5 In recent years, cases have been increasingly associated with iatrogenic injuries and immunosuppression.1-3 Posterior LA have been reported following intubation and nasogastric tube placement. 2 Laterally based cricoarytenoid joint abscess has been identified as a complication of chronic rheumatoid arthritis, with successful management documented. 6 Spontaneous LA have also been newly associated with poorly controlled diabetes.1,7 These shifts highlight the evolving etiological landscape of LA over time.
A modern review of LA illustrates a significant shift from historical patterns, with the majority of recent cases occurring in immunocompromised patients. 1 Of the 8 spontaneous cases reviewed, 6 involved immunosuppression, including patients with autoimmune diseases, organ transplant recipients, and those undergoing chemotherapy. 1 The findings underscore the increasing prevalence of immunodeficiency in contemporary laryngeal supuration cases.
Veiga-Alonso et al. 8 conducted a comprehensive 34-year review of laryngeal abscess cases, identifying 13 patients, with epiglottitis being the most prevalent etiology (61%). Notably, 23% of these patients were immunosuppressed, and a significant proportion required urgent airway interventions, including tracheostomy and cricothyrotomy, due to severe airway obstruction. All cases underwent transoral drainage under general anesthesia, and while there were no fatalities, 2 patients experienced severe complications, emphasizing the potential severity of LA. 8
The clinical presentation and imaging findings in the present case suggest a superimposed infection of the arytenoid cyst, which likely precipitated the development of the supraglottic laryngeal abscess formation. This case presented a diagnostic challenge due to clinical and radiologic features suggestive of malignancy, including a bulging aryepiglottic fold mass with ipsilateral vocal fold immobility and necrotic lymphadenopathy, in the context of heavy tobacco and alcohol use. Differential diagnoses included advanced carcinoma of the laryngeal ventricle, benign neoplasms (e.g., schwannoma and neurofibroma), granulomatous diseases (e.g., tuberculosis and sarcoidosis), and post-traumatic lesions. However, the resolution of symptoms and vocal fold mobility following empiric antibiotic therapy confirmed the diagnosis of a spontaneous laryngeal abscess, highlighting the importance of conservative management and close clinical follow-up in selected cases.
Its incidence varies between 2% and 29%, but it remains an exceptionally rare diagnosis, particularly in immunocompetent individuals.1,2 The microbiology of contemporary LA differs significantly from historical patterns. While past cases were often linked to tuberculosis and typhoid, modern abscesses involve a diverse range of pathogens, including Pseudomonas aeruginosa, Actinomyces, Staphylococcus aureus, and Group B Streptococcus. 1 This variability suggests the opportunistic nature of severe laryngeal infections today.
LA typically present with pain, hoarseness, odynophagia, and dyspnea, and are often associated with impaired vocal fold mobility, leading to stridor, and potential airway compromise. Progression to asphyxia can occur rapidly, with patients potentially suffocating without warning. 9 This was especially common in cases of typhoid fever. 9 Examination may reveal edema, erythema, and glottic narrowing, with vocal fold immobility due to cricoarytenoid joint involvement. Reduced vocal cord mobility can result from soft-tissue edema or joint inflammation, with posterior infections more likely to affect the cricoarytenoid joint. Approximately half of the patients with a laryngeal suppuration may not exhibit acute upper airway obstruction. 2
Prior to the advent of antibiotics, LA were associated with a near 100% mortality rate. 4 With the recognition of the importance of early intervention, mortality rates have significantly decreased due to advancements such as early tracheostomy and prompt incision and drainage. 4 Diagnosis of LA requires direct laryngoscopy and CT imaging. Direct laryngoscopy enables a thorough examination of the inflamed larynx, including regions not visible through indirect methods, and helps identify cartilaginous sequestra or pus accumulation. The current approach of performing careful endoscopic evaluation in all suspected cases has significantly reduced the incidence of these abscesses.
LA represent a potentially life-threatening condition that may require urgent intervention, including tracheostomy, translaryngoscopic incision and drainage, and high-dose intravenous antibiotics. Airway management is critical, with many patients requiring tracheostomy for advanced airway compromise, to relieve pressure on the larynx and facilitate tracheal aspiration. Surgical intervention is essential, alongside culture-directed antimicrobial therapy. Soft-tissue abscesses can be drained via direct laryngoscopy under general anesthesia, while necrotic cartilage requires external drainage and removal of nonviable fragments to prevent further infection. In severe cases, laryngectomy may be necessary due to persistent infection and laryngeal dysfunction.2,4 In less severe cases, both endoscopic and transcutaneous drainage are effective. Medical management with antibiotics alone has been shown to be an effective treatment for a 1.3-cm paraglottic abscess. 2
Major complications of LA include aspiration pneumonia, mediastinitis, and vocal cord fixation, with the most concerning outcome being the destruction of the cartilaginous framework, leading to laryngeal stenosis, a well-known complication in historical cases.4,5
Conclusion
This case highlights several key considerations in clinical practice. LA should be considered in the differential diagnosis of unilateral vocal fold immobility, particularly when associated with supraglottic swelling or posterior infection. It emphasizes the necessity of maintaining a high index of suspicion for spontaneous laryngeal suppuration, even in immunocompetent individuals without prior surgical history, to avoid misdiagnosis and ensure timely intervention. In addition, it illustrates how LA can closely mimic malignancy, particularly in patients with risk factors such as heavy tobacco and alcohol use, underscoring the importance of thorough diagnostic evaluation, including endoscopy, imaging, and biopsy when indicated, to rule out neoplastic processes. Finally, it illustrates that conservative management with antibiotics and vigilant follow-up can be an effective therapeutic approach to LA in selected patients, potentially obviating the need for invasive procedures.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Consent to Participate
Written informed consent was obtained from participants included in the report.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.