
Abstract
Balloon-assisted dilation (BAD) of paranasal sinus ostia is a Food and Drug Administration (FDA)-approved minimally-invasive procedure used to treat medically refractory chronic rhinosinusitis. Several large cohort studies have reported relatively-low complication rates with BAD. Thus, users of this technology may perceive this to be a safer alternative to formal dissection of the frontal and sphenoid sinus and perform these as office-based procedures. Here, we present 2 patients who underwent BAD of the sphenoid sinus and developed cerebrospinal fluid leak (CSF) leaks with pneumocephalus. Both patients had thinning of the planum sphenoidale in generously-pneumatized sphenoid sinuses. Although BAD is considered safe, review of the current literature demonstrates that serious complications can occur. These case reports demonstrate the potential for skull base injury, particularly in hyper-pneumatized sphenoid sinuses with dehiscent bone. Preoperative anatomic evaluation is crucial to identify at-risk patients. During BAD, trauma to critical structures may cause CSF leak and result in pneumocephalus. This knowledge is important for improving surgical decision-making and patient counseling.
Introduction
Introduced into clinical practice in 2006, balloon-assisted dilation (BAD) devices offer the ability to dilate sinus ostia (i.e., balloon sinuplasty) as an in-office procedure performed under local anesthesia. This technology has gained widespread popularity in the United States due to its efficacy and association with low complication rates.1,2 However, adverse events (AEs) such as cerebrospinal fluid leak (CSF), pneumocephalus, orbital complications, and severe bleeding have been reported. 3 As with the adoption of conventional endoscopic sinus surgery (ESS), analysis and reporting of AEs related to BAD are important to document in the literature. We therefore present characteristics and events afflicting 2 patients treated at a tertiary medical center for CSF leak and pneumocephalus following BAD of the sphenoid ostium.
Case Presentation
Case 1
A 51-year-old female was transferred to our hospital for further management of CSF rhinorrhea. She underwent BAD of the bilateral maxillary, frontal, and sphenoid sinuses at an outside facility 10 days prior for sinus disease. The sphenoid body appeared hyper-pneumatized with a very thin planum sphenoidale on the images obtained from before her procedure (Figure 1A). Two days after her BAD, she presented to an emergency room (ER) with nausea and headache. She re-presented a day later with persistent symptoms and left-sided clear nasal drainage. Computed tomography (CT) scan of her head revealed significant pneumocephalus. She was admitted for bed rest and conservative management for a presumed CSF leak. Due to continued leak, headaches, and low-grade fever, she was transferred to our care. A non-contrast CT at this time showed a breach in the mid-planum sphenoidale just anterior to the sella turcica (Figure 1B).
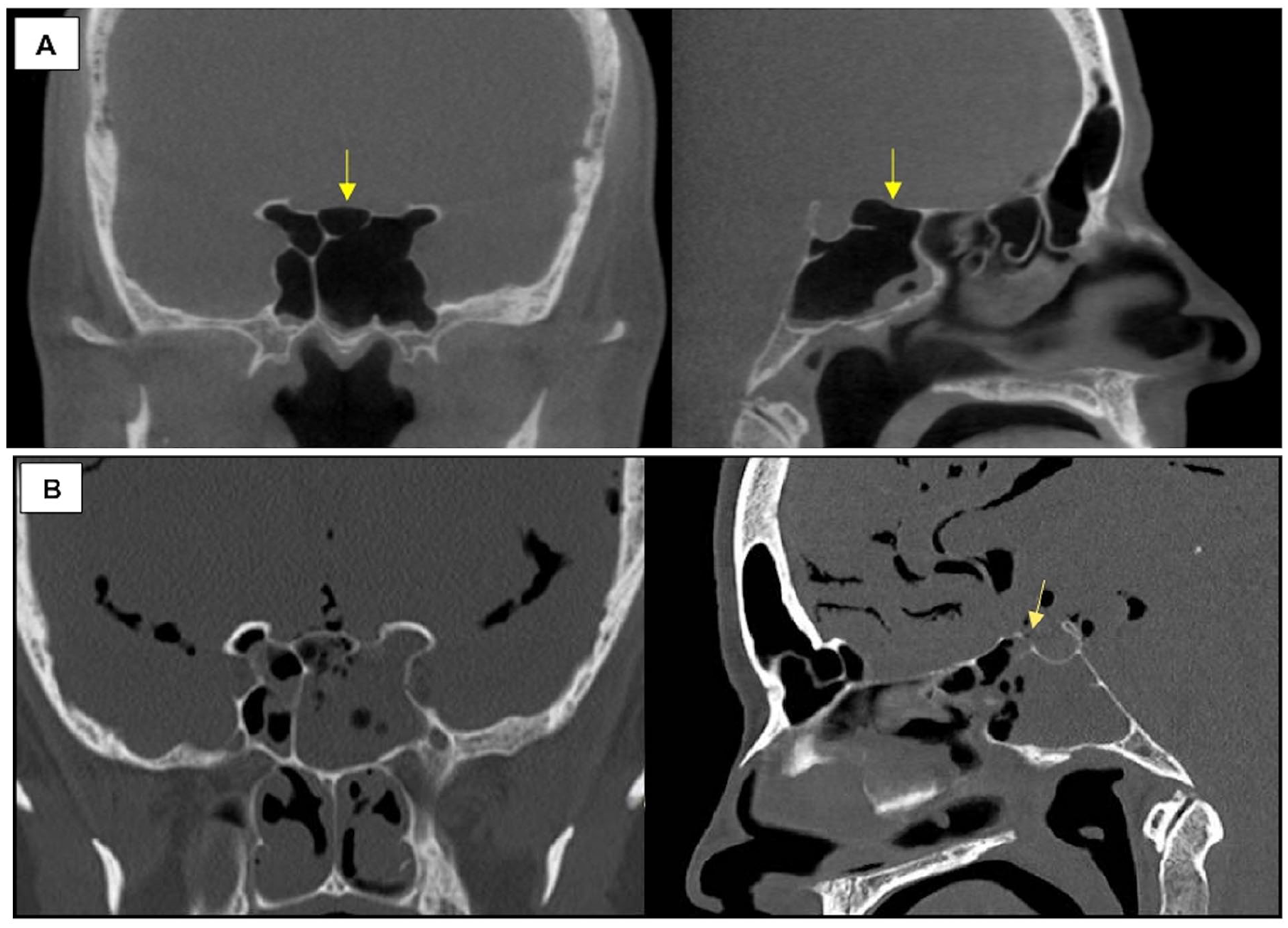
(A) Pre-procedural coronal (left) and sagittal (right) CT scan of the head. The arrow highlights thinning of the planum sphenoidale. (B) Coronal and sagittal CT of sphenoid sinus with suspected location of breach (arrow) and significant associated pneumocephalus. CT, computed tomography.
The patient was taken for urgent surgical repair, where the sphenoid was found to be filled with clear fluid and a high-pressure, high-volume leak from a 2 mm mucosalized fistula likely in communication with a subarachnoid cistern. The surrounding planum bone appeared to be fractured after the mucosa around it was elevated. The site of injury was just inferomedial to and within 5 mm of bilateral dehiscent carotid arteries in the planum sphenoidale. The leak was successfully repaired in a layered fashion using a nasoseptal flap. Lumbar puncture was consistent with bacterial meningitis. She was treated with an anti-meningitic antibiotic protocol for 6 weeks and recovered without neurologic sequela.
Case 2
A 41-year-old female presented to our hospital’s ER with complaints of headaches and difficulty with gait coordination a few hours after undergoing BAD of the right sphenoid sinus at an outside facility. Indications for her procedure are presumed to be related to sphenoidal sinus disease, as demonstrated in her pre-procedural scans (Figure 2A). Upon arrival, non-contrast CT studies revealed moderate pneumocephalus that was most prominent in the right frontal region, as well as a defect in the roof of the right sphenoid sinus with communication into the intracranial space (Figure 2B). As with Case 1, the sphenoid body was hyper-pneumatized with a notably-thin planum sphenoidale. Bony defects were also identified in the cribriform plate and the posterior roof of the right frontal sinus, representing potential areas of dehiscence which may have predisposed the patient to a dural tear.
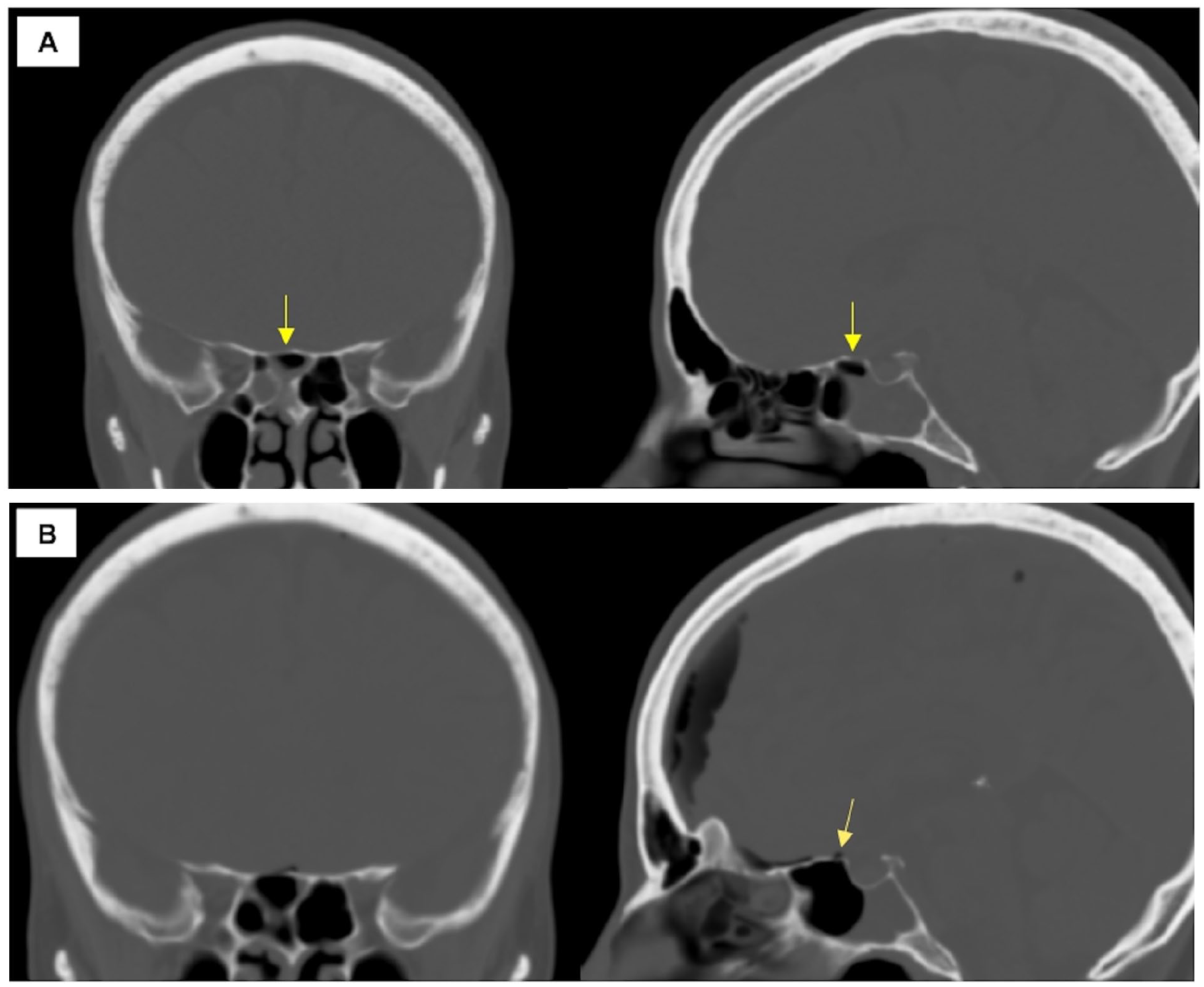
(A) Pre-procedural coronal (left) and sagittal (right) CT showing near complete opacification of the right sphenoid sinus with fluid level. The arrow highlights thinning of the planum sphenoidale. (B) Coronal and sagittal CT demonstrating moderate volume pneumocephalus with suspected location of breach (arrow). CT, computed tomography.
The patient was taken urgently to the operating room. Right sphenoidotomy revealed pooled fluid and debris within the sinus floor. A low-flow CSF leak was identified from a 2 mm defect in the right planum sphenoidale. The defect was repaired using a narrow-based pedicled nasoseptal flap and reinforced with tissue sealants and nasal packing. Postoperative imaging showed near-complete resolution of pneumocephalus at the 24th hour. The patient healed well and had no further complications postoperatively.
Discussion
Although widely adopted, there is a paucity in the literature on complication rates associated with balloon-assisted sinus procedures. Given wider adoption of the technology, there is a need to report such AEs in the literature, outside of mandated FDA reporting. Tomazic et al. 4 in 2010 published the earliest report of an ethmoid skull base leak after a patient underwent BAD of the frontal ostium. 5 Medial orbital wall fracture and orbital hematoma during maxillary sinus ostia balloon dilation have been reported.6,7 There has also been an incident of cardiac arrest secondary to oculocardiac reflex following BAD of the frontal recess. 8 Alam et al. 9 in their case series describe 3 patients who experienced pneumocephalus and 2 with orbital complications. Similar to our cases, another report of CSF leak following BAD resulted in a tension pneumocephalus. 10
There have been several database studies evaluating complications as well. A review querying the openFDA database revealed 114 reported AEs, including 4 deaths. 11 Seventeen cases of skull base injury with 15 CSF leaks were noted in this study. Orbital injury was the most common complication, with 13 patients requiring lateral canthotomy and 3 needing medial orbital wall decompression. CSF leak was significantly associated with dilation of the frontal and sphenoid sinus, while orbital injury was associated with maxillary sinus dilation. Severe epistaxis was observed more often with sphenoid sinus dilation, presumably because of the proximity of the sphenopalatine artery to the native sphenoid sinus ostia. A separate openFDA database study analyzing cases from 2015 to 2018 found 78 AEs involving BAD procedures. 12 Of these, there were 19 reports of skull base injury with CSF leaks and 1 case of pneumocephalus. Hur et al. 13 in a study of the Manufacturer and User Facility Device Experience found 211 AEs occurring from 2008 to 2018. Forty-eight percent of the AEs were classified as patient-related, with CSF leak (36%), eye swelling (29%), and epistaxis (12%) being the most common. As with the other database studies, CSF leaks were significantly associated with frontal and sphenoid sinus surgery, underscoring the increased risk of skull base injury when performing sphenoidal BAD. These findings are consistent with our series. While hyper-pneumatization and a thin planum sphenoidale have not been specifically identified in the literature as risk factors, it would seem plausible that these factors increase the risk profile in a locale already prone to injury. Altogether, these studies highlight the possibility of a serious complication and stress the importance of careful patient selection, reviewing individual patient anatomy, and timely recognition of complication.
Patients who have undergone BAD should have similar work-up and management of complications as patients undergoing conventional ESS. Given the anatomic complexity and limited access of the sphenoid sinus, BAD may be suboptimal in cases of isolated sphenoid disease, where direct visualization and potential tissue removal through ESS could provide greater diagnostic and therapeutic precision. The use of BAD may have limited the ability to adequately address underlying pathology, particularly as the indications for intervention in Case 1 were questionable from the outset. When an iatrogenic CSF leak is encountered, it is best managed by urgent repair rather than by conservative management, which may increase the risk of meningitis, pneumocephalus, intracranial infections, and permanent neurologic sequelae. In contrast to post-traumatic leaks, bed rest for iatrogenic CSF leak is not appropriate due to low risk of spontaneous healing. When a delayed leak is repaired, a formal fistula may form and require excision.
Overall, balloon-assisted devices appear to be relatively safe with low complication rates, though major AEs can occur from this sinus dilation technique. Future research should address specific characteristics and treatment factors that predispose patients to AEs.
Conclusion
Herein, we present 2 cases of skull base injuries resulting in CSF leaks with pneumocephalus following BAD of the sphenoid sinus. Otolaryngologists should be aware that serious complications can occur with balloon technology. Given the location of the trauma, the dehiscence over the carotid artery and optic nerve canals, and the blind nature of instrumentation, these case reports should raise concern for injury to critical structures—particularly in patients with hyper-pneumatized sphenoid sinuses and thinned bone. These unique factors should be accounted for in the preoperative decision-making process, and patients should be counseled accordingly. Ultimately, this series provides meaningful information to surgeons as they engage with patients and optimize their treatment plans.
Footnotes
Acknowledgements
None.
Ethical Considerations
Our institution does not require ethics approval for reporting individual cases or case series.
Consent for Publication
Both patients provided written informed consent according to CARE guidelines and in accordance with the principles of the Declaration of Helsinki. This case series was not considered human subjects research and was thus exempt from IRB approval.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.