
Abstract
Purpose:
Objectives were to characterize patients with inducible laryngeal obstruction (ILO), evaluate exercise-induced asthma (EIA) test results, and determine the need for future testing in this population.
Methods:
A retrospective chart review was performed at a tertiary children’s hospital on all pediatric patients seen in the Vocal Cord Dysfunction specialty clinic from February 2018 to February 2020. Demographics, medications, comorbidities, ILO triggers, symptoms, EIA test results, and follow-up otolaryngology and pulmonology appointment information were collected.
Results:
Sixty-eight patients with ILO were identified at a median age of 14.5 (range: 9-18) years. Most were female (n = 50, 73.5%) and white (n = 65, 95.6%). Nearly all (92.6%) patients were triggered by exercise and 72.1% by laryngopharyngeal reflux. Almost all (98.5%) patients described difficulty breathing when triggered, with a third (35.3%) having stridor. Median time from initial symptoms to presentation was 12 months (range: 3 months-10 years) and median episode duration was 5 minutes (range: 30 seconds-3 hours). EIA testing was performed in 82.4%. Most (96.4%) patients did not exhibit an ILO episode during flexible fiberoptic laryngoscopy.
Conclusions:
ILO benefits from a multidisciplinary team approach. Patients were triggered primarily by exertion or reflux, though the underlying behavioral health predispositions have not fully been explored.
Keywords
Introduction
Inducible laryngeal obstruction (ILO), an umbrella term encompassing vocal cord dysfunction (VCD) and other laryngeal disorders such as exercise-induced laryngomalacia, 1 requires diagnosis and treatment with a multidisciplinary approach. There have been many different names over the years, and it continues to be further defined within the context of irritable larynx syndrome. Specifically, paradoxical vocal fold movement involves unintentional vocal fold adduction during inspiration that causes an acute onset of symptoms including difficulty breathing and stridor.2,3 These symptoms are frequently and historically attributed to asthma4,5 or laryngopharyngeal reflux (LPR). 6
Frequently, alternative diagnoses and treatments are considered and implemented prior to the consideration of ILO, the primary diagnosis being asthma or exercised-induced asthma. 7 This may be partly a result of the historical terminology used to describe the disorder throughout the last 5 decades. 8 Due to the multifaceted nature of ILO, patients are often started on a variety of medications and see multiple physicians and specialists before referral to an otolaryngologist for formal diagnosis. Much of the pediatric ILO research in the United States has centered on case reports and small reviews.5,9-12 By assessing 2 years of consecutive ILO patients in a specialty clinic at a large tertiary children’s hospital, we can better describe associated diagnoses and comorbidities in the pediatric population.
At our institution, an exercise-induced asthma (EIA) test is frequently ordered for the same day as the ILO initial consult. The EIA testing includes pre-exercise and postexercise pulmonary function tests. The senior author is the sole otolaryngologist at the specialized VCD clinic at our hospital and works closely with the clinical physiologist and pulmonologist during the EIA. A flexible fiberoptic laryngoscopy (FFL) examination is performed at the point in the pulmonary function test when either (a) the patient reports feeling symptoms associated with ILO or (b) before the postexercise medication challenge and pulmonary function test is performed again. It is important to note that this test is time-consuming, costly, and can be disputed by insurance for necessity.
The objectives of this study were to (1) characterize ILO patients by assessing comorbidities, triggers, and symptoms, (2) evaluate EIA test results.
Methods
This study was approved by the University of Pittsburgh Human Research Protection Office Institutional Review Board (STUDY20060029). The requirement for informed consent was waived. A retrospective chart review was performed at our tertiary care children’s hospital on all patients seen at the VCD specialty clinic for initial consult appointment from February 2018 to February 2020 by 1 otolaryngology attending. Patients are referred from physicians for symptoms suggestive of ILO. This is a multidisciplinary pediatric clinic for ILO that takes place 1 day a month. Diagnosis of ILO was made through a combination of interview, review of systems, and history of symptomatology. Multidisciplinary evaluation was performed by a laryngologist and a speech-language pathologist (SLP) who specializes in voice and upper airway disorders. Criteria for diagnosis included rapid onset of inspiratory dyspnea that resolved with rest, site of restriction (neck rather than low lungs), and presence of a trigger such as exercise or psychological stressor. Other factors such as lack of response to asthma medications and age 7 or older increased suspicion for ILO. Patients were excluded if reported symptoms were not consistent with ILO or if the initial consult appointment was not during the study period. Data collected included demographics (biological sex and United States Census-designated race), prescribed medications, comorbidities, patient-reported ILO triggers, symptoms when triggered, EIA test results, and follow-up appointments with otolaryngology and pulmonology. Prescribed medications included reflux, asthma, anxiety, and allergy treatments. Comorbidities, triggers, and symptoms variables were not mutually exclusive. All patients were taught breathing exercises by a SLP at the time of the initial evaluation after the EIA testing was complete.
The protocol for EIA testing was as follows: Patients underwent baseline spirometry, electrocardiogram (EKG) leads (12-lead EKG) and pulse oximetry were placed, and exercise was performed on a treadmill with a modified Bruce protocol (gradually increasing intensity with simultaneous spirometry). Exercise stopped when the patient endorsed distress or the end of the protocol was reached, and the patient was seated for laryngoscopy. Laryngoscopy was performed while the patient was panting. Following laryngoscopy, spirometry was repeated at the 1st, 5th, 10th, and 15th minute. The patient was then given albuterol, and testing was repeated. EIA diagnosis was based on a decrease in forced expiratory volume in 1 second of ≥10% after exercise. Methacholine challenge was not performed.
Laryngoscopy was considered normal if there was no obstruction of air flow from the nares to the vocal folds throughout inspiration and expiration. Findings were considered abnormal if there was airway obstruction including and not limited to internal/external nasal valve collapse, deviation of the nasal septum, adenoid hypertrophy with obstruction, turbinate hypertrophy, lateral pharyngeal wall/tonsillar prolapse with Mueller maneuver, paradoxical vocal fold movement with inspiration, or supraglottic laryngeal obstruction with inspiration.
Statistics were performed with SPSS version 27 (IBM, Armonk, NY) with P < .05 denoting significance. Statistical tests included the Mann-Whitney U.
Results
A total of 88 patients were seen at the VCD clinic for the evaluation of possible ILO at a consult appointment. Sixty-eight (77.3%) had clinical symptoms consistent with ILO. The inclusion and exclusion study flow chart is seen in Figure 1. A total of 68 ILO patients were identified at a median age of 14.5 years (range: 9-18 years). A majority were female (n = 50, 73.5%) and white (n = 65, 95.6%). Other races included Asian (n = 1, 1.5%), black or African American (n = 1, 1.5%), and mixed race (n = 1, 1.5%). Over half of patients were taking medication at the consult (n = 42, 61.8%); 16.2% (n = 11) were taking reflux medication(s). Other medications were for asthma (32.4% of patients), anxiety (11.8%), and allergy (35.4%).
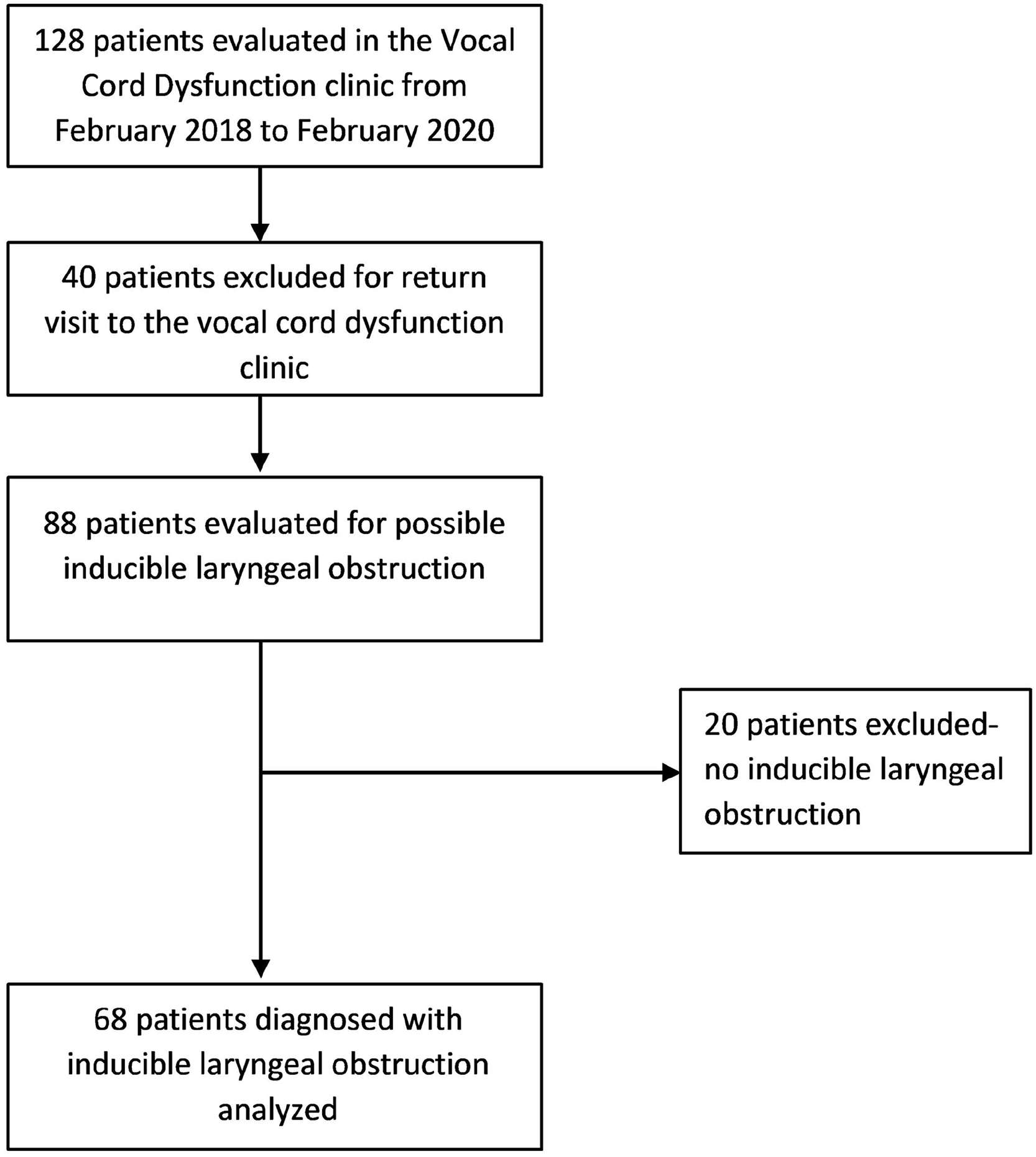
Study inclusion and exclusion flowchart.
Table 1 presents comorbidities. The comorbidity with the highest percentage was environmental allergies; a third of the patients (n = 25, 36.8%) reported environmental allergy symptoms. This cohort exhibited low rates of history of anxiety (17.6%) and depression (2.9%). While 88.4% (n = 61) were athletes, a quarter of the patients were reported to be overall competitive in nature including in academics and/or sports. Most patients were triggered by exercise (n = 63, 92.6%) seen in Figure 2. Of those who were not triggered by exercise (n = 5), 2 were triggered by stress and social change, 1 by cold air and LPR, and 1 patient was triggered by viral illnesses.
Comorbidities of the Pediatric Patient Population With Paradoxical Vocal-Fold Movement Disorder.
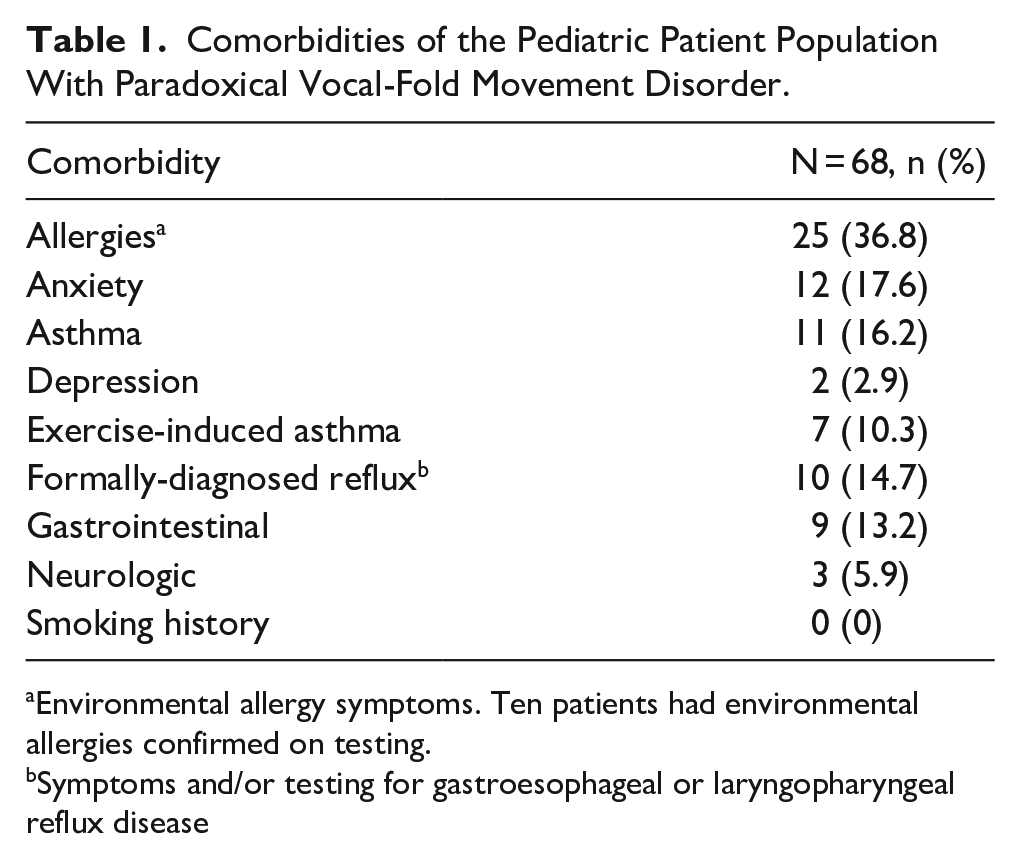
Environmental allergy symptoms. Ten patients had environmental allergies confirmed on testing.
Symptoms and/or testing for gastroesophageal or laryngopharyngeal reflux disease
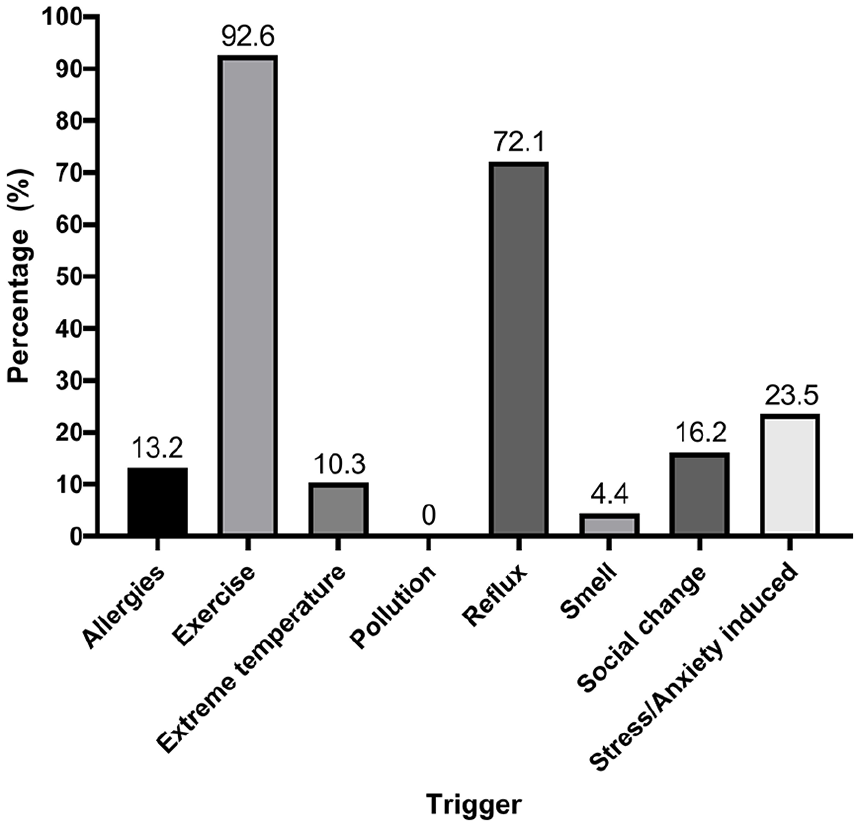
Inducible laryngeal obstruction and patient-reported triggers (N = 68).
ILO symptoms when triggered are seen in Figure 3. The only patient without difficulty breathing described a pain in the throat as well as a cough. Stridor was present in 35.3% of patients (n = 24). There was a median time since initial symptom presentation of 12 months (range: 3 months-10 years) from 57/68 patients. Of those that reported a quantitative duration of symptoms when triggered (n = 42), there was a median duration of 5 minutes (range: 30 seconds-3 hours); however, 4 patients reported symptoms lasting a whole day up to a few days. There were no significant differences between symptom duration in minutes and each of the symptoms (P > .05). About half of the patients (n = 37, 54.4%) tried a bronchodilator breathing treatment for symptoms. Of those with post-breathing treatment follow-up (n = 33/37), 39.4% reported symptom improvement versus 60.6% with no improvement.
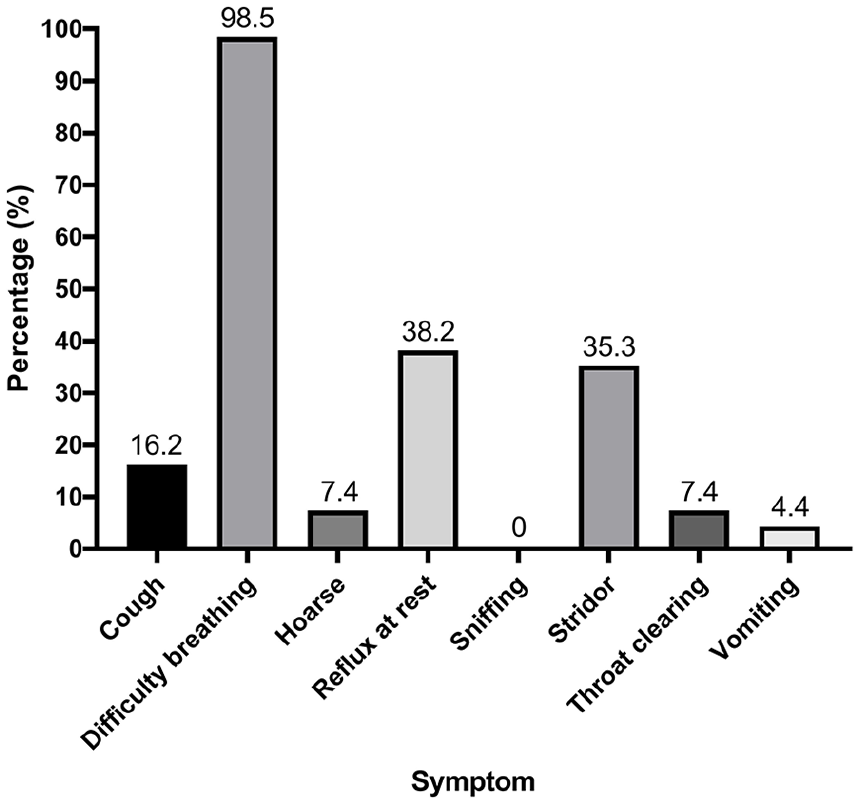
Symptoms when triggered (N = 68).
Most patients had an EIA test at the time of the initial evaluation (n = 56, 82.4%). During the exercise portion of the test, most (85.7%) patients reported feeling symptoms that they associate with ILO. Flattened or notched inspiratory loops were observed in 21 (37.5%). A complete FFL was conducted after they stepped off the treadmill and sat on a chair. Of these patients, 54/56 had normal movement of the vocal folds (no VCD) visualized at that time; visual laryngeal examination was within normal limits, and EIA testing was negative for asthma. The remaining 2 patients had a comorbid diagnosis of EIA identified from the test. Follow-up after initial evaluation is not routinely scheduled with either ENT or the pulmonology department unless positive findings from EIA and FFL testing are recorded. Almost half of the patients (n = 29, 42.6%) underwent an evaluation with pulmonology prior to their first visit to our VCD clinic. Respiratory retraining with an SLP occurred the same day. This consisted of 1 session; follow-up with the SLP is scheduled on an as-needed basis regarding breathing techniques.
Discussion
Our study aimed to characterize ILO in the pediatric population at a specialty VCD clinic at a large children’s hospital. For 2 consecutive years, we assessed all patients with initial consult visits. By studying our patients, we were able to delve further into triggers and subsequent symptoms as well as results of testing and benefits to our current evaluation. We were also able to begin to make recommendations regarding standardized reporting.
Adult patients are the focus in most of the literature characterizing ILO.13-16 Morris et al. 17 performed a comprehensive review and found that 70.8% of the patients in the literature were adults. When looking at the pediatric population, Maturo et al.’s 11 cohort had a mean age of 13.6 years and were predominately female (76%). This is comparable to our demographic of female, white, and preadolescents or adolescents with a median age of 14.5 years. In more recent literature, Fujiki et al. 18 described 112 children diagnosed with ILO; 89 (79%) were female, and mean age was 13.8 years. Smith et al. 10 reported 59% (n = 29) of patients were female with an average age at symptom onset of 12 years. Although we did not assess average age at onset, our patients had a median symptom presentation of 12 months before the consult.
Most of our patients (92.6%) had their ILO symptoms triggered by exercise with a majority playing competitive sports. Zalvan et al. 19 reported 79.2% with exercise-induced dyspnea while Doshi and Weinberger 20 reported 59.2%. More recently, Alanazi et al. 21 reported exercise as a trigger 86% of their cohort. Hseu et al. 22 separated their cohort into different categories, formally diagnosing 30% with exercise-induced vocal fold dysfunction and 19% with spontaneous vocal fold dysfunction. Our higher proportion of patients with clinical symptoms consistent with ILO may be understood through the lens of our population comprised of mainly adolescent, female, competitive athletes. Athletes may be more likely to attend an appointment to improve their performance rather than those whose symptoms did not have high stakes consequences such as sitting out for a game.
ILO is agreed upon to have a psychological component, 23 which historically was considered to be the primary cause.24,25 In more recent literature, comorbid psychiatric diagnoses were present in 30% of children in 1 study 11 and 70% in another. 26 Furthermore, parents underestimated their child’s anxiety and depression symptoms in the latter study. 26 In our study, the psychological aspect may have been under-reported due to the nature of the clinic; we do not have formal mental health questionnaires or a psychologist available at this time. However, the attending physician does directly ask the patient and parents if the patient has ever been treated or diagnosed with depression, anxiety, or other mental health concern. Patients and parents were interviewed at the same time, possibly resulting in an environment where some patients would not have been comfortable sharing information regarding anxiety or other psychiatric concerns. Self-report surveys may better evaluate the psychological component in this population.
Interestingly, our cohort had a wide duration of symptoms when triggered, ranging from 30 seconds to 3 hours with 4 patients reporting the symptoms extended throughout the day into multiple days. Although clinical presentation was consistent with ILO, these long-duration symptoms have not been previously described in the literature in a large cohort to our knowledge and should be further investigated with increased documentation. Although 67 of 68 patients in our series experienced dyspnea with exertion, only 35% of our population reported stridor. Although this is consistent with previous reports,7,27 the prevalence of stridor may also be under-reported in our cohort due difficulty reproducing symptoms in the clinic and consequent reliance on patient and parent-report and understanding of terminology.
At our hospital, an EIA test, including pre- and postexercise pulmonary function tests and FFL, can be performed at the time of the appointment. Fifty-six of our cohort had our EIA test protocol and 85.7% of them reported similar symptoms during the treadmill test as they experience at home or during activity when triggered. Flattened inspiratory loops, suggesting extra-thoracic obstruction, were present in only 21 patients who completed EIA tests, which is consistent with previous reports 28 and not surprising since this may not be a sensitive indicator of laryngeal obstruction. 29 During the laryngoscopy, 96.4% did not exhibit paradoxical motion of their vocal cords. Therefore, diagnosis of ILO was typically made based on symptom presentation without observation of vocal-fold adduction. Contributing factors may include stopping of exercise prior to the flexible scope being passed and the patient seated during the FFL. In addition, verbal instructions during the FFL portion include encouraging the patient to “sniff” in through the nose to help pass the scope, which may in turn have been a treating response for the symptoms. A rate of 3.6% had an abnormal test with EIA comorbidly diagnosed. Distinct phenotypes and protocols to distinguish between ILO and other diagnoses have been described previously.20,30-33 Although continuous laryngoscopy during exercise has been described as the gold standard for diagnosis of exercise-induced laryngeal obstruction, 34 in our patient population and lab setup this is not tolerated or possible. Notably, others have highlighted the importance of cardiopulmonary monitoring to confirm the functional consequences of any laryngeal anomalies observed and propose cardiopulmonary testing during exercise and prompt laryngoscopy only in the presence of stridor or decreased flow volumes. 35 Therefore, we use continuous flow volume loop spirometry, direct observation, and postexercise interview of symptomatology along with laryngoscopy. Flow-volume loops were obtained continuously through testing and monitored in real time, but not all participants were able to replicate their symptoms of ILO. Therefore, relying on the observation of a flattened inspiratory loop would also commonly yield false-negative findings.
The FFL portion of EIA testing provides visual examination of nose, nasopharynx, pharynx, and supraglottic structures. This also allows the physician to assess vocal-fold function and mobility and rule out any other sources of obstruction or irritation. Laryngoscopy is also used as biofeedback to the patient either in real time or after the procedure when the patient is shown their laryngoscopy video. We can use this biofeedback to assure the patient of vocal cord mobility, airway patency, and finally to instill confidence of intact laryngeal functioning. This confidence also plays an undefined, but accepted, role in respiratory retraining with the SLP as the correct next step. The biofeedback portion of the evaluation is seldom discussed but is very important in decreasing anxiety surrounding ILO symptoms.
Moving forward, further standardized reporting is necessary in this population, as well as prospective study for symptom change and improvement. Individuals for whom the ILO diagnosis remains uncertain after thorough case history and symptom gathering would benefit from FFL and EIA. Additionally, formal screening of behavioral health appears to be an essential and under-evaluated aspect to explore. Our current practice at the evaluation is the recommendation to meet with a SLP for introduction of breathing strategies. These strategies are to be used proactively for symptom prevention and/or management once symptoms are triggered. Reflux medication is prescribed only if symptoms were also present outside of exercise as well as diet modifications. Discussion of postnasal drip and allergy symptoms is included with emphasis on the structure and function of our nose for filtration, humidification, and warming of the air prior to passing through the vocal cords.
A multidisciplinary approach to the management of ILO provides assurance of accurate diagnosis. Notably, 32.4% of patients were on asthma medications at the time of evaluation, while only 16.2% had an asthma diagnosis. This discrepancy between asthma prescriptions and diagnosis has been previously reported. 21 Prescriptions for bronchodilators were not given at the VCD clinic visit. These prescriptions were placed by other providers such as the primary care physician who may have treated the patient empirically prior to formal asthma diagnosis or from the referring pulmonologist. This highlights the need for evaluation in a specialized clinic to correctly attribute symptoms. In addition, the identification of any contributing diagnoses such as EIA, LPR, allergic rhinitis, and other behavioral disorders such as stress and anxiety provides the opportunity for concurrent treatment with ILO. Lastly, the ability to initiate therapy in the form of respiratory retraining strategies the same day allows for the best and most efficient patient care and satisfaction. Limitations exist with the nature of a retrospective cohort study. Few patients returned to the otolaryngology department after the initial consult. We do not have data regarding efficacy of reflux or allergy medication as well as patient-reported response to breathing strategies employed by the SLP. It is most likely that the psychologic component of ILO was underrepresented also due the retrospective design. We plan to perform a long-term prospective survey study in this population with surveys given at the consult and at a follow-up appointment if scheduled or by mail or e-mail. This follow-up data would be especially important because positive responses to SLP treatments may increase the confidence in diagnosis when laryngoscopy is negative. In addition, these data would provide opportunity for comparison with improvement in other studies. 20 Another limitation was, due to the rarity of the disorder, our patient sample was limited in number. Comprehensive standardized patient reporting at the appointment was limited and is necessary in this population. In addition, a detailed description of the results of pulmonary function testing, specifically flattening of the inspiratory loop, would help to more fully characterize this population in future studies.
Conclusion
Diagnosing ILO requires eliciting a specific case history and symptomatology. If there is potential for multiple etiologies, FFL and EIA testing may be considered to direct the treatment plan. Consideration should always be given to time, cost, and how the treatment plan is affected by the information gathered. It is through a thorough evaluation that includes a multidisciplinary approach that you can affect the best patient outcomes. While almost all of our patients had identified triggers of exertion or reflux, psychological factors should not be discounted. It is well accepted that psychological comorbidities can be a trigger for ILO. Prospective pre-and-post survey design study is needed to standardize reporting in these patients and could include dyspnea indexes 36 before and after respiratory retraining therapy and biofeedback such as that provided during laryngoscopy.
Footnotes
Acknowledgements
None.
Author Note
Previous Presentations: This project was virtually presented by Jennifer L. McCoy, as an e-poster at the American Society of Pediatric Otolaryngology (ASPO) annual meeting from April 9 to 11, 2021.
Ethical Considerations
This study was approved by the University of Pittsburgh Human Research Protection Office Institutional Review Board (STUDY20060029).
Consent to Participate
The requirement for informed consent for this chart review study was waived by the University of Pittsburgh Institutional Review Board.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
De-identified data will be made available upon reasonable, written request to the corresponding author and execution of any institution-mandated data sharing agreements.