
Abstract
Background:
The multidisciplinary tumor board (TB) meeting is a vital aspect of comprehensive cancer care worldwide. Functional flaws in TBs can interfere with maximal performance, leading to several inefficiencies and potentially impacting treatment outcomes.
Objective:
The aim of this study was to analyze the effect of a prospectively-developed list of straightforward patients and their consensus treatment options, also known as a “consensus slate,” on TB efficiency.
Methods:
The consensus slate was developed prior to each weekly TB meeting, and effect of the slate on TB efficiency was analyzed. The main measurement of efficiency was time difference in presentation of those straightforward patients before and after slate implementation.
Results:
Consensus slate implementation resulted in a 78.5% decrease in average discussion time of straightforward patients during TB. An average of 25% of each week’s TB list was presented using the slate.
Conclusion:
This series demonstrates the efficacy of a tool such as the consensus slate in streamlining the TB process. The ultimate result of this streamlining is greater meeting productivity through increased number of patients that can be presented, improved clinician engagement, and increased standardization of patient presentations.
Introduction
Tumor boards (TB) are multidisciplinary team meetings used worldwide for comprehensive care of patients with cancer. In the United States, these meetings are reported to have been used since the 1970s, and they were initially education-centered meetings. 1 Since then, TBs have evolved to be much more care-centered 1 and are associated with improved treatment outcomes and higher quality of care.1-4 This is the reason they have become the gold standard for cancer care today. TBs should include clinicians from the range of specialties involved in cancer care; at a minimum medical oncology, radiation oncology, oncologic surgery, radiology, and pathology,3,4 which allows for a comprehensive discussion of patients/treatment options resulting in a multidisciplinary treatment recommendation. The reported benefits of having care directed by a multidisciplinary TB have included more accurate staging of disease, higher patient survival, higher patient satisfaction, more clinical trial recruitment, greater cost effectiveness, timelier diagnosis and treatment of patients, education opportunities, greater well-being for both patients and providers, better care coordination between specialties, and greater care consistency across patients.1-4
Despite all the potential advantages of TBs, these meetings have been reported to suffer from inefficiencies that may decrease team member engagement and potentially compromise quality of care. Previously-reported inefficiencies include incomplete case information for presentation, unmanageable caseload, redundant presentation, wasted time, incorrect recommendations, and rushed discussions.1,3,5 Although these and other inefficiencies are recognized, there are relatively-few studies that assess potential solutions to address them. In this study, we aimed to propose a change to the structure and presentation of a TB list with the goal of addressing unmanageable caseload, wasted time, and rushed discussions.
The information required for a TB to determine the best treatment currently available for a patient includes the histology of the tumor (many comprehensive cancer centers require internal review of outside pathology), clinical staging, and, often, radiographic staging. National clinical practice guidelines, such as those published by the National Cancer Comprehensive Network (NCCN), serve as a reference algorithm for clinicians to provide consistent, evidence-based care in addition to the team-based decisions made with TB discussions. 6 For this study, when all the required information is reviewed by the treating clinician prior to the TB meeting and the patient falls into an algorithm on the NCCN guidelines, the case is considered a straightforward case, and we believe that team-based discussion is unlikely to add any new or necessary information to treatment recommendations and may therefore be unnecessary. Although other cases can often fall within national treatment algorithms, they may be complicated by unique factors that make panel discussion necessary for well-rounded evaluation and decision of best management, factors such as complex comorbidities, unclear diagnoses, multiple disease sites, or strong patient preferences regarding treatment options. The straightforward cases generally have minimal to no patient history factors that would complicate decision of best management, regardless of staging and demographic information. Other cases that team-based discussion does not add further benefit to and can be considered straightforward are those that are presented for postoperative pathology review and any other cases where the best treatment option for the patient can be decided on clearly by any clinician, without benefit or improved judgement from a panel discussion.
Preparation for TBs is a significant time burden for pathology and radiology. At institutions like ours, for pathology this requires pulling case slides and advance review of the slides, then taking digital photographs of key sections to load into a PowerPoint presentation, which is utilized during the meeting. With multiple pathologists participating, this often meant the pathologist presenting at TB was not the pathologist who signed out the case and therefore took considerable time to review all the slides. Similarly, for radiology, the neuroradiologist prepares by reviewing all scans pertinent to the cases and prepares shortcuts for easy access to PACS during TB discussions. Because we have multiple neuroradiologists, this often meant reviewing scans that had been previously read by one of their partners, as well as outside of films.
We hypothesize that a TB can be more efficient if straightforward cases and their treatment recommendations can be identified prior to presentation, and discussion of these cases is limited to a simple presentation during the meeting with all the straightforward recommendations simultaneously endorsed as a slate. This study consists of 2 phases—(1) confirmation of the feasibility of identifying straightforward cases for a consensus slate and (2) evaluation of the time efficiency of incorporating a consensus slate for straightforward patients into the Head and Neck Cancer TB at the Stephenson Cancer Center.
Materials and Methods
Preliminary Data Collection
Between August 2022 and March 2023, preliminary data were collected to assess length of discussion time for straightforward cases at the weekly head and neck TB for the Stephenson Cancer Center, a part of the University of Oklahoma in Oklahoma City, Oklahoma. This multidisciplinary TB occurs weekly and prospectively discusses all patients with primary and recurrent head and neck cancer. It typically consists of head and neck surgeons, and representatives from neuroradiology, head and neck pathology, medical and radiation oncology, dermatology, and endocrinology, as well as support staff and trainees. The weekly TB list was assessed by a single experienced clinician to identify straightforward cases, and the discussion of each of these cases was timed during TB without knowledge of the discussing clinicians.
Slate Development
In March 2023, the project was disclosed to members of the TB along with a proposed template for a consensus slate that included disease site, stage, unique patient history, imaging and pathology notes, and recommended treatment option for each case (Figure 1). The treating provider was asked to identify whether a case was eligible for the consensus slate as they were added to the weekly list. The cases on the consensus slate were placed at the top of the circulated TB list, and circulated to participating members in advance per our usual protocol.
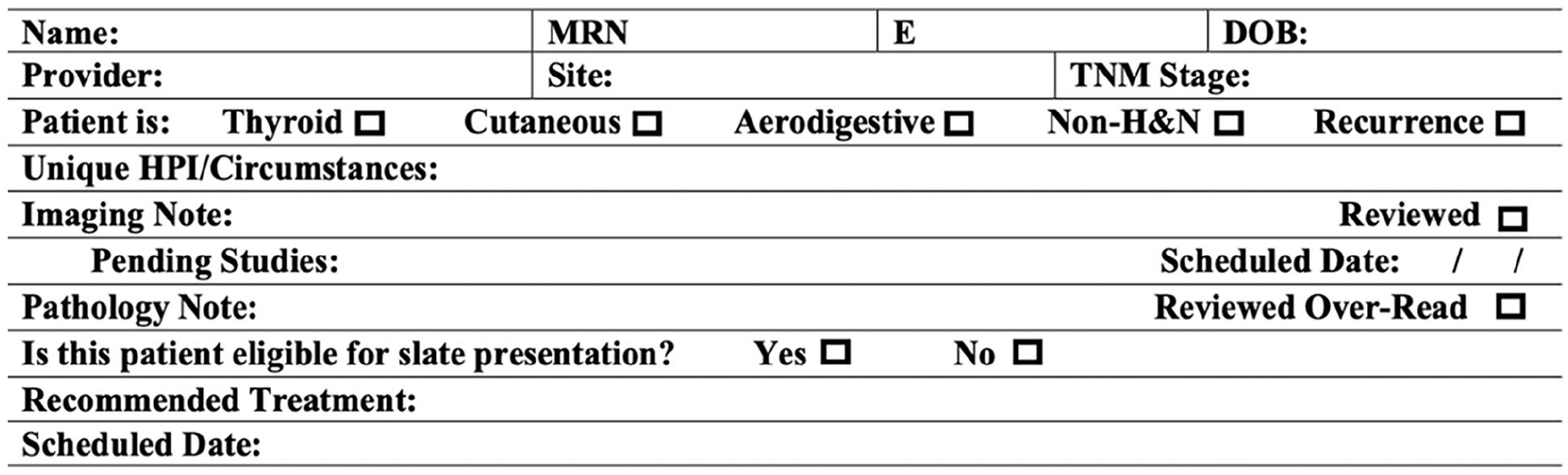
Slate patient template.
Slate Implementation
From April 2023 to November 2023, the consensus slate was incorporated into the TB meetings and its effectiveness evaluated. In preparation for the TB meetings, the presenting pathologist would ensure that all histopathology for the slate cases was signed out by one of our institutional head and neck pathologists, but no slides were pulled for review, and no digital photographs prepared for the TB meeting. Similarly, for radiology, the presenting neuroradiologist for TB checked the site of origin for films and if internal to our institution did not review any images in preparation for TB. If the films were obtained outside of our institution, they reviewed the imaging to verify that the radiographic staging correlated with the staging on the TB list, and if there was disagreement created the shortcut to facilitate discussion. The slate was presented at the beginning of TB by a single team member by reviewing but not discussing individual cases. The data reviewed included patient demographics, unique history, tumor site and stage, and recommended treatment option. Following the review of all the cases on the consensus slate, the TB team was given the opportunity to clarify information on any of the slate cases or to remove a case from the slate if they thought that case required discussion. Following this, the slate recommendations were endorsed as final recommendation, and the TB meeting continued with the regularly-discussed patient list. Length of presentation time of the slate was measured and recorded from beginning of the presentation until final team slate approval along with the number of patients on the slate, total number of TB patients that day, and slate patient disease sites/staging.
Results
In the preliminary data collection period, 550 patients were presented at 24 TB meetings. A total of 125 cases (23%) were identified as straightforward. The average presentation time of each was 2 minutes and 15 seconds, ranging from 16 seconds to 8 minutes and 17 seconds. Disease sites for straightforward cases included the spectrum of head and neck cancers (Figure 2), and clinical staging ranged from carcinoma in situ to advanced tumors with metastatic disease.
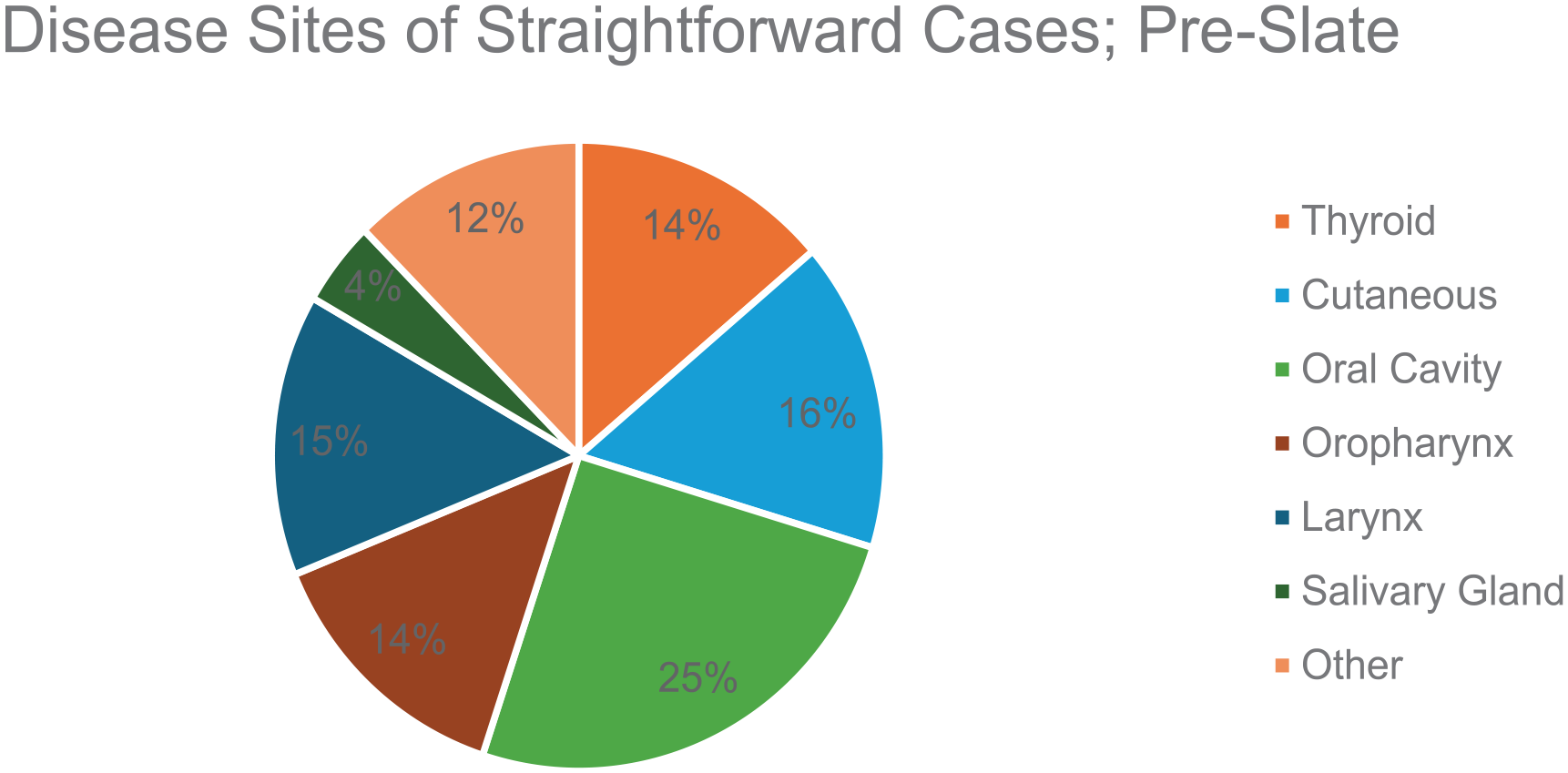
Disease sites of straightforward cases prior to slate implementation.
During the slate implementation period, 739 patients were presented at 30 TB meetings, of whom 198 (27%) cases were identified as straightforward and consequently presented on the consensus slate. This ranged from 10% to 45% of the TB weekly list. Disease sites of consensus slate patients included the spectrum of head and neck cancers (Figure 3), and staging again ranged from carcinoma in situ to advanced tumors with metastatic disease. The time per slate case ranged from 17 to 57 seconds (Figure 4), with an average of 29 seconds. There were 3/198 (1.5%) cases that were removed from the slate to the traditional discussion list due to missing staging information and 19/198 patients (9.6%) had information that was clarified during slate presentation, such as staging information, patient location preferences, and clinical trial qualification.
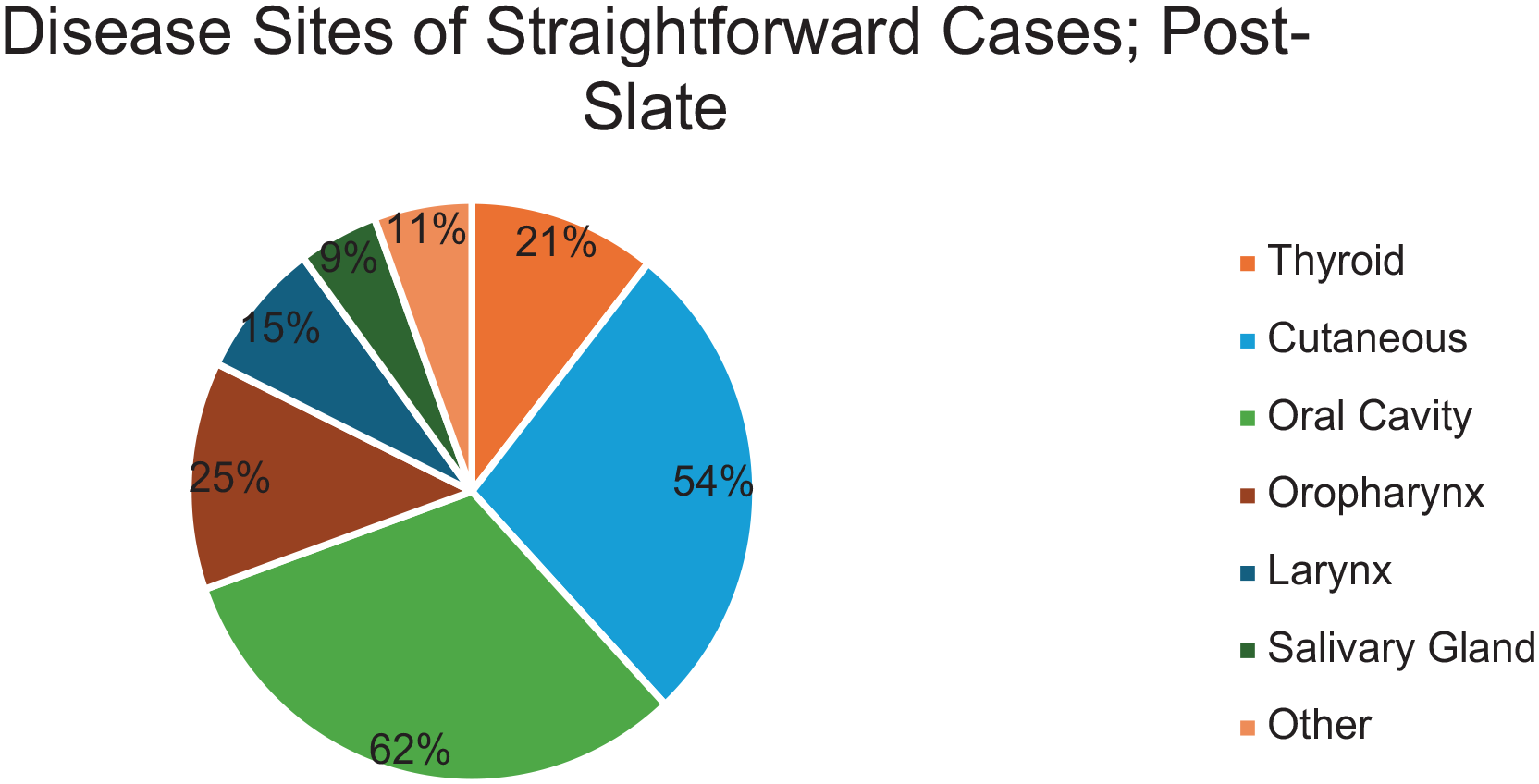
Disease sites of straightforward cases after slate implementation.
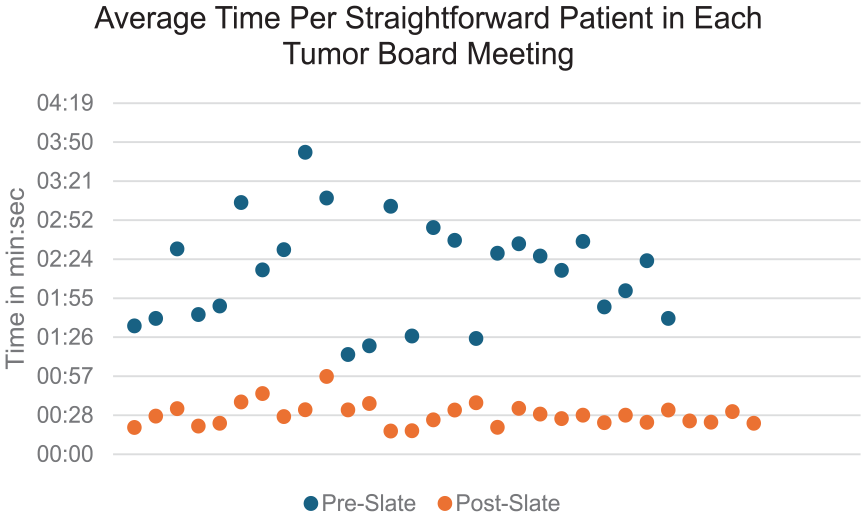
Average time spent on discussion or presentation of straightforward patients in each tumor board meeting.
Discussion
In the initial months of implementation of the consensus slate, the average discussion time of our straightforward patients was reduced by 78.5% from an average of 2 minutes 15 to 29 seconds with only 10% requiring any discussion beyond the data reviewed by the presenter of the slate. This verified our hypothesis that straightforward cases could be identified in advance of the TB meeting. For the average meeting, the consensus slate trimmed 12.5 minutes out of a scheduled 60 minute meeting time for up to a 20% time savings. For the pathologist participating in TB, we did not measure the time impact for preparation, but on the average week, it resulted in pulling slides/preparing photographs for 7 less cases, which should have decreased their preparation time by ~30%. For radiology, we did not include data on the percentage of cases that had outside of films and therefore still required review by the neuroradiologist in preparation for TB. While we cannot quantify the time savings, we can say that all cases of internal imaging did not require re-review, and we believe this resulted in time savings during preparation.
The idea that straightforward cases needlessly use up extra time during multidisciplinary TBs is not novel, and these cases have been proposed as the targets of TB streamlining before.3,7,8 However, few studies exist that test and/or analyze exact methods of streamlining as this study did. When contemplating what to do with straightforward cases, removing them altogether is undesirable due to the concern that cases not discussed in TB may result in suboptimal care recommendations. 3 This was substantiated by our data that showed almost 10% of cases on the consensus slate had some correction/amendment of information when presented. The consensus slate serves as a safety net to ensure that the treatment recommendations for all patients have been reviewed by the multidisciplinary clinician panel and follow clinical practice guidelines.
One significant value of TB presentation is the complex patient whose care requires meticulous review/discussion that can take 8 to 10 minutes to do well. Maximizing time for discussing these cases requires efficiency and with a consensus slate, there is a decreased caseload for full discussion and therefore greater meeting productivity. Prior to the slate, we would anecdotally often notice time pressure during presentation and discussion of the TB list that led to a rushed discussion of cases as we got closer to our meeting adjournment, an issue similar to what has been reported by others.1,9 Thus, any amount of time saved could allow for a more comfortable, extensive discussion that is required of the complex cases. Other benefits of the slate that we noted but did not specifically analyze are more consistent completion of the meeting within allotted time, more standardized patient presentations, increased panel engagement, and more time for educational points during TB.
One of the problems encountered with implementation of the slate was a delay in use of the slate by some of the head and neck surgeons on our TB panel. This likely resulted by the “surprise” nature in which we initiated it, the significant change, lack of familiarity, and lack of remembering when a patient could be eligible for the slate. Although not documented, there were a handful of times when clinicians would comment that a patient discussed in the regular TB list “could have been on the slate,” indicating an underrepresentation of potential slate patients during our trial period. This idea is supported by the general upward trend of percentage of total TB patients on the slate (Figure 5). Our initial data suggested 23% of cases would be eligible, but this was based on the review of a list by a single observer who often had not seen the patient. The reason for having a single reviewer initially was to keep the preliminary data collection phase blinded to as many of the TB panel members as possible, even if it did lead to an underrepresentation of slate-eligible patients during the preliminary phase. For that reason, it was expected that use of the slate by the whole group in the post-implementation phase would result in an increased number of patients on the slate. Our implementation period showed 27% of our cases were identified as slate-eligible; 2% were removed from the slate, so 25% of cases were ultimately included in slate endorsement of provider recommendations. We believe that with time, this number could potentially reach 40% when the treating providers make the recommendation for inclusion in the slate and those providers become more comfortable with the concept and process.
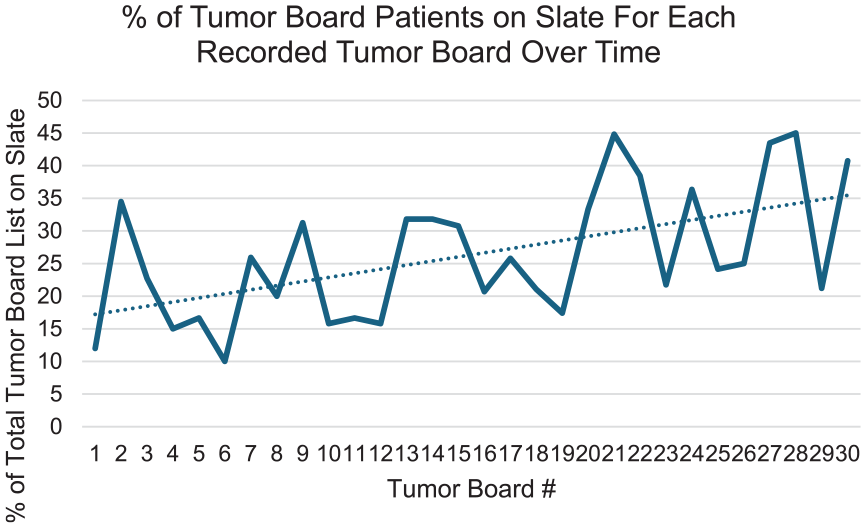
Percentage of each week’s tumor board list patients that were on the slate.
An interesting future study would be analysis of the characteristics of all cases that qualified for the slate over time. Although identification of these characteristics is not necessary for weekly identification of slate patients due to the variety of cases that could qualify as straightforward (a range of patient demographics, disease sites, and disease stages), it would be interesting to assess whether any trends exist in cases that qualified for slate presentation more than others or whether there are cases with certain characteristics that consistently do or do not qualify for the slate.
Conclusion
TBs are widely used across specialties and institutions, and efforts to ensure maximal efficiency and quality benefit patients and providers. When all pertinent information is available prior to a TB meeting, consolidating presentation of straightforward cases into a consensus slate eliminated superfluous discussion while ensuring guidelines were followed with a roughly 20% reduction in meeting time. We believe that with long-term implementation, these results will lead to higher satisfaction with TB by participants, further solidifying its role as the gold standard method for comprehensive cancer care.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.