
Abstract
Dysphagia and dysphonia are commonly-presenting symptoms to ENT clinic. This case report highlights a case of prior COVID-19 infection and subsequent development of a vocal process granuloma associated with persistent dysphagia and dysphonia symptoms. The approach to management is discussed, highlighting the importance of surgical excision to rule out malignancy, the typical histological findings, and the resulting sustained improvement in symptom burden on the patient.
Introduction
A 53 year-old female presented with a 6 month history of intermittent hoarseness, dysphagia, and globus sensation after COVID-19 infection. Her globus sensation was most pronounced after meals, often progressing to coughing fits not associated with coughing up undigested foods, heartburn, postnasal drip, or difficulty breathing. She began experiencing dysphonia 3 months after her symptom onset. Symptoms did not resolve with a trial of fluconazole, famotidine, antibiotics, nasal budesonide spray, cetirizine, pseudoephedrine, or saline rinses. Her past medical history was significant for environmental allergies. She denied any smoking or drinking history. There was no relevant family history.
In-office flexible laryngoscopy revealed a well-circumscribed, pedunculated lesion of the left arytenoid that did not involve the vocal folds (Figure 1A). The patient underwent direct laryngoscopy under general anesthesia and a soft, pink, 0.9 × 0.9 × 0.4 cm mass was excised at its base (Figure 1B). Pathology revealed acutely inflamed granulation tissue and scant benign squamous mucosa, consistent with a vocal process granuloma (Figure 2). The squamous epithelium was mildly hyperplastic without evidence of dysplasia or carcinoma in situ with evidence of early granulation tissue including plasma cells, scattered lymphocytes, and neutrophils within a loose stroma (Figure 2B and C). Three weeks postoperatively, her voice was clearer, dysphagia and globus sensation had resolved, and arytenoid mucosa had healed without recurrence. Written informed consent and an exemption were obtained from the UCLA IRB.
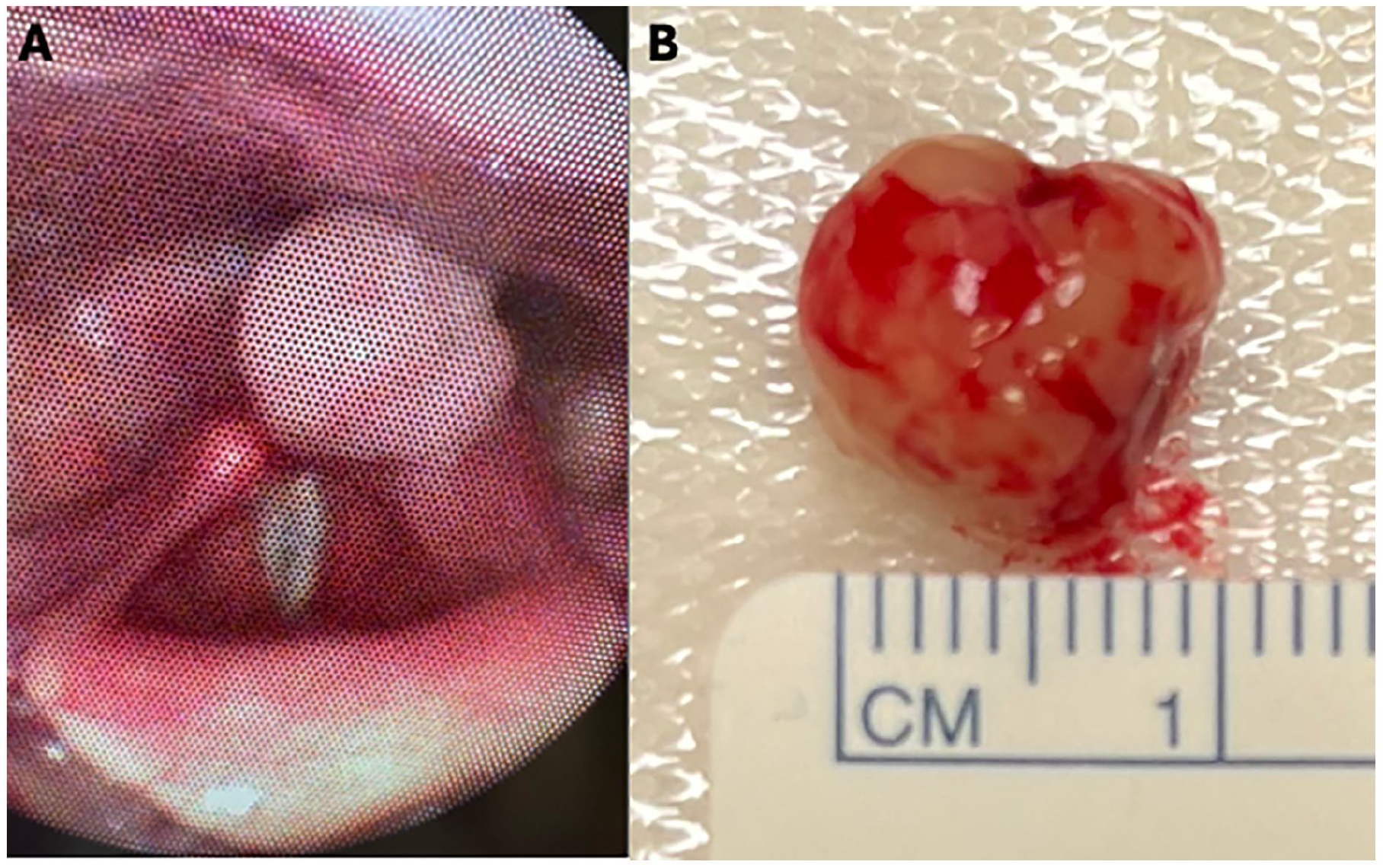
(A) Flexible laryngoscope demonstrating left arytenoid pedunculated mass. (B) Surgically resected mass measuring 0.9 × 0.9 × 0.4 cm.
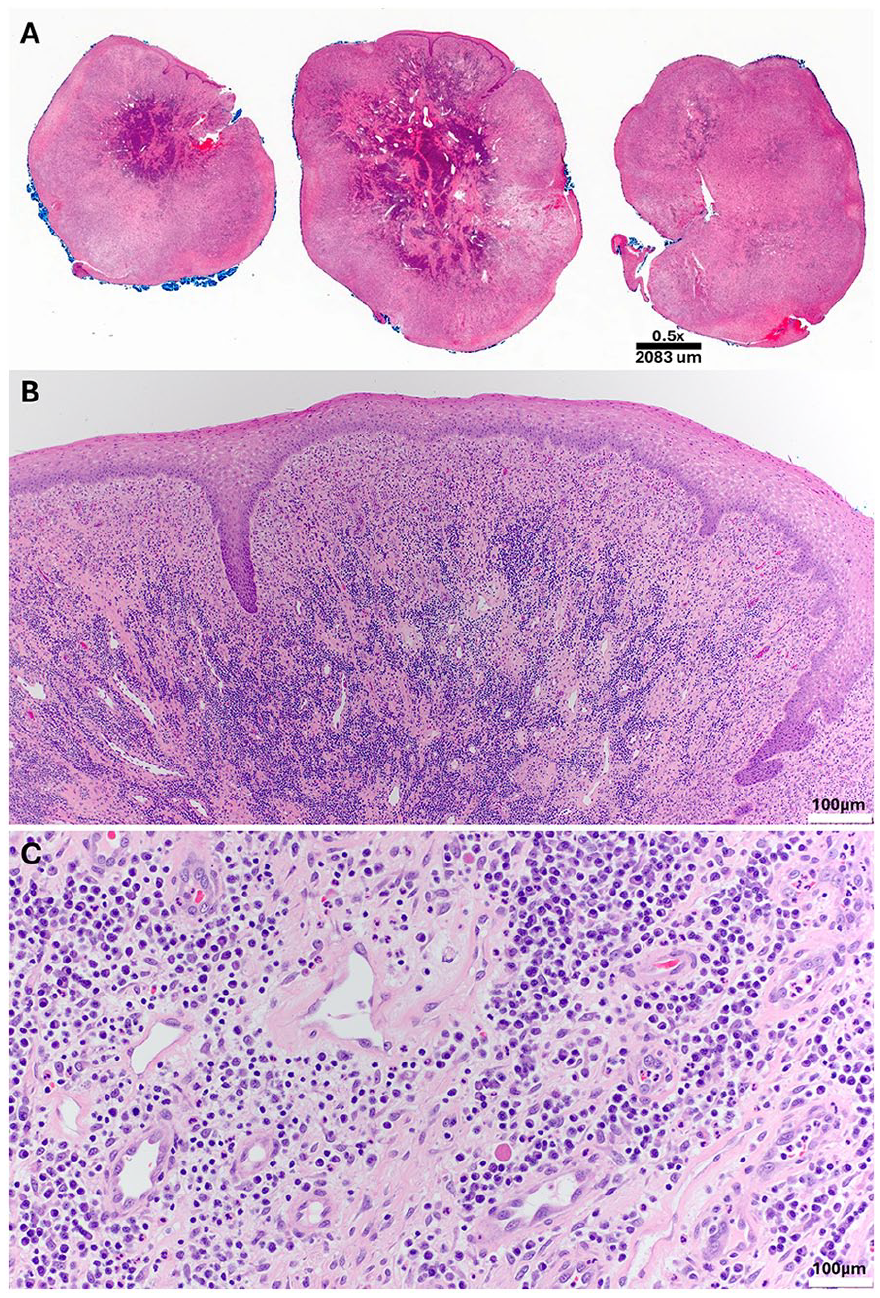
(A) Panoramic view of the trisected lesion showing a nodular growth involving the squamous mucosa. The overlying squamous epithelium is largely eroded and ulcerated. (B) The squamous epithelium is mildly hyperplastic, without evidence of dysplasia or carcinoma in situ. The underlying lamina propria is largely replaced by early granulation tissue, characterized by proliferating capillaries (angiogenesis) and a mixed inflammatory infiltrate (hematoxylin and eosin stain, original magnification ×40). (C) Granulation tissue at higher magnification shows numerous plasma cells, scattered lymphocytes, and neutrophils within a loose fibroblastic stroma containing multiple capillaries (original magnification ×200).
Discussion
Vocal process granulomas are benign growths that occur more commonly in males relative to females and adults relative to children. They predominantly arise unilaterally in the vocal process of the arytenoid but also present along the middle or anterior thirds of the vocal cords. Their appearance varies, ranging from gray to red in coloration, sizing between 2 and 15 mm, and gross texture may be polypoid, nodular, pedunculated, or ulcerated. 1 Clinical presentation most commonly involves hoarseness (91%), followed by globus sensation (47%), dyspnea (18%), cough (12%), and rarely, hemoptysis (6%). 1
The first report of a vocal process granuloma was of a contact ulcer by Chevalier Jackson in 1928 and was theorized to result from abusive phonation. Etiologies of vocal process granulomas are grouped into mechanical (eg, post-intubation, endoscopic procedure, or surgical trauma) or inflammatory (eg, gastroesophageal reflux, infectious, allergic, or idiopathic) causes. Mechanical processes may include repeated contact or irritation such as habitual throat clearing or abusive phonation. 1 Since the COVID-19 pandemic, there are increasing reports of persistent vocal symptoms including dysphonia with varying underlying pathophysiology relating to the viral infection. 2 The case presented here represents a post-COVID vocal process granuloma that was not associated with prolonged intubation.
Vocal process granulomas are not true granulomatous lesions, and they get their name from their gross appearance. Histopathologic examination often demonstrates squamous epithelial hyperplasia with proliferation of granulation tissue and with acute or chronic inflammatory cell infiltration. 1 Treatment depends on etiology. Conservative approaches targeting the underlying cause (eg, acid suppression, voice rest, voice therapy) can be effective (reported to be curative in 41%). 3 When conservative approaches fail, microsurgical resection resolves vocal process granulomas in 78% of cases. 3
The differential diagnosis of vocal process granulomas includes benign recurrent respiratory papillomatosis, fibromas, cysts, and malignancy. Alternative infectious and noninfectious granulomatous diseases should also be considered. 1 Respiratory papillomatosis, most commonly caused by human papillomavirus strains 6 and 11, is estimated to affect 1.8 adults and 4.3 children per 100,000, with risk factors including smoking, number of lifetime sexual partners, and maternal HPV at birth. 4 Endoscopic findings often demonstrate grape-like clusters. Treatment involves surgical excision with growing evidence suggesting an increased role for medical therapy in minimizing recurrence. 4
Other benign vocal fold lesions include cysts, fibromas, nodules, and polyps. Vocal cord cysts can occur in the subepithelial space and ligamentous region of the lamina propria and are often unilateral. They are associated with vocal overuse or can occur after a respiratory infection. These more commonly present in women. Vocal cord cysts can appear yellow in hue due to keratin and are managed with surgical excision. Pathology can differentiate 2 types of cysts: mucous retention or epidermoid. 5
As with any vocal fold lesion, it is important to rule out malignancy. Intraepithelial dysplasia can sometimes be seen and is categorized as low-grade or high-grade based on histopathologic features such as mitoses and rare apoptotic and dyskeratotic cells in the former, with progression to nuclear atypia, pleomorphism, and hyperchromasia in the latter. The most common malignancy in the larynx is squamous cell carcinoma (SCC), with keratinization seen on histopathology. Variants of SCC, including basaloid, papillary, and spindle cell SCCs, as well as adenosquamous and verrucous carcinoma may also be diagnosed on pathology. 6 A biopsy is an important diagnostic step in ruling out possible malignancy.
Footnotes
Ethical Considerations
Our institute does not require ethics approval for reporting individual cases.
Consent to Participate
The participant provided written informed consent prior to participating.
Consent for Publication
The participant provided written informed consent for publication.
Author Contributions
S.L.M.: analysis, drafting, and editing manuscript. S.H.: data collection and analysis, drafting, and editing manuscript. A.E.K.: design, conduct, analysis, and editing manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.