
Abstract

Keywords
A transgender individual is defined as a person who has completed or is in the process of modifying their physical characteristics through medical interventions to align their body with their gender identity, which differs from their biological sex. 1 Approximately 75% of transgender individuals are biologically male and seek to transition to female (male-to-female, MTF). 2 For MTF individuals, achieving a voice that aligns with their gender identity remains one of the most challenging and socially impactful aspects of gender transition.
While hormone therapy can significantly alter many secondary sex characteristics, it does not effectively raise vocal pitch in those assigned male at birth.3,4 Voice feminization often represents the final step in MTF transition and plays a pivotal role in the individual’s perception and expression of gender identity. 5 A nonfeminine voice may serve as a major barrier to social integration and the ability to function in society as a woman.6,7 As a result, voice feminization surgery becomes an important consideration.
To address this, several surgical techniques have been developed to raise vocal pitch by increasing vocal fold tension, altering vocal fold consistency, and reducing vocal fold mass. 4 Cricothyroid approximation, first described by Isshiki et al., feminizes the voice by tensing the vocal folds through fixation of the cricoid cartilage to the thyroid cartilage. 8 Although widely utilized, the Isshiki technique has demonstrated variable and often inconclusive long-term outcomes.4,5
In contrast, an endoscopic technique described by Wendler has shown more stable and consistent results in voice feminization.8,9 The technique involves anterior glottic web formation through epithelial denudation and suture approximation of the vocal folds. 4 This leads to a permanent increase in pitch with minimal disruption to other vocal parameters. 4 The technique has gained popularity due to its safety profile and relative predictability. 4
Based on the senior author’s experience, we offer a perspective on a modified version of the Wendler technique and its subjective outcomes in transgender women. Between 2015 and 2018, 20 patients underwent glottoplasty using this modified technique. The Transgender Self-Evaluation Questionnaire (TSEQ) was distributed to all patients at least 6 months postoperatively. The TSEQ includes one global item assessing gender congruence of the voice, followed by 30 statements evaluating daily vocal experience, each rated on a 5-point Likert scale.
Fourteen patients returned completed questionnaires. The mean patient age was 43 years (range 28–61), and the average time from surgery to survey completion was 18.2 months. Half of the patients were smokers, and 71.4% were on hormone therapy (Table 1). When asked to describe their current voice, 64.3% of participants rated it as “very” or “somewhat female.” However, 85.7% reported a desire for a “very female” voice, indicating a partial gap between expectations and outcome.
Patient Demographics.
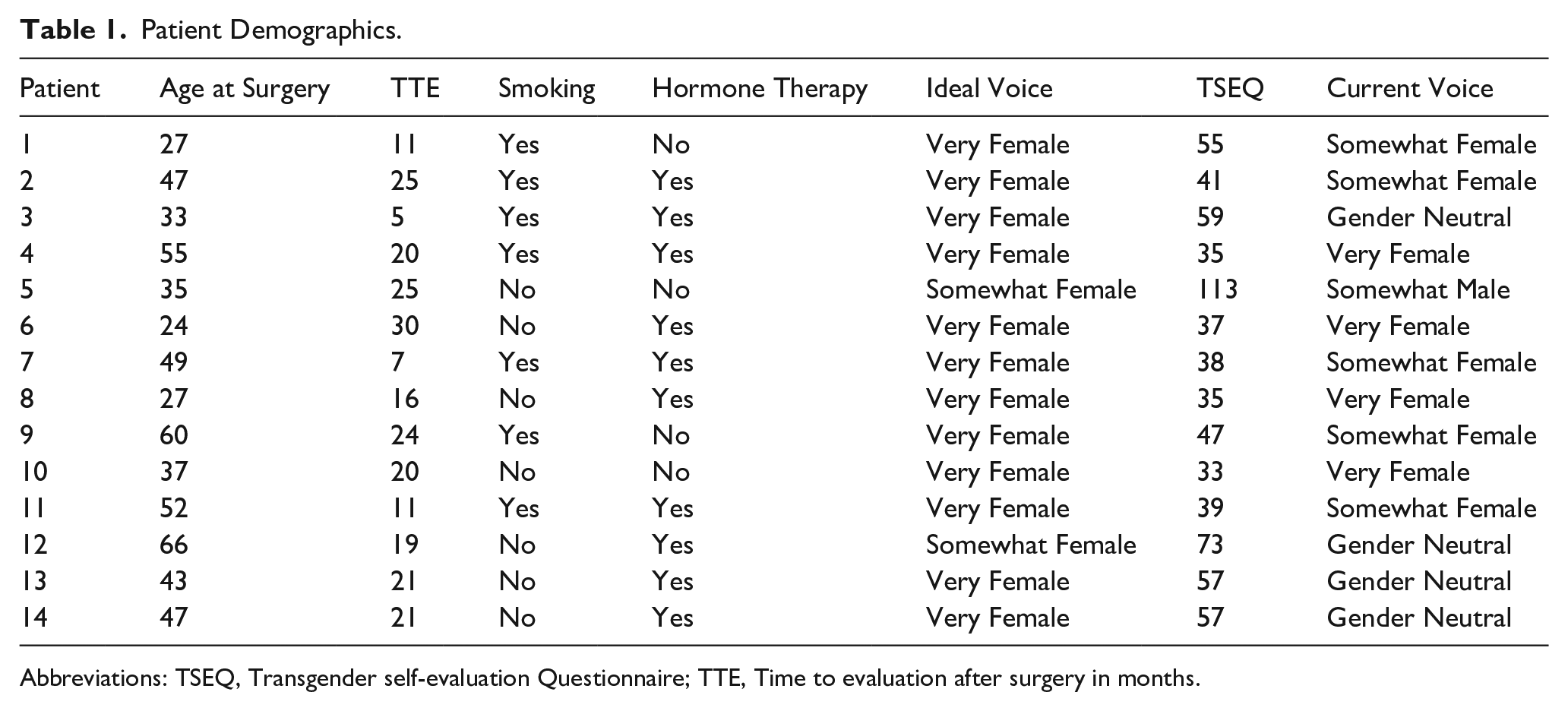
Abbreviations: TSEQ, Transgender self-evaluation Questionnaire; TTE, Time to evaluation after surgery in months.
The average TSEQ score was 51.3 out of a possible 120. Although most participants experienced improved vocal gender congruence, the overall satisfaction level was moderate. Using the median TSEQ score (44) to define the presence of voice-related handicap, we performed subgroup comparisons based on age, smoking status, hormone use, and time since surgery (Table 2). No statistically significant differences were identified across these variables, suggesting that perceived satisfaction is influenced more by individual factors than by medical history or hormonal status.
Association Between Patient Characteristics and Postoperative TSEQ Scores (Fisher’s Exact Test).
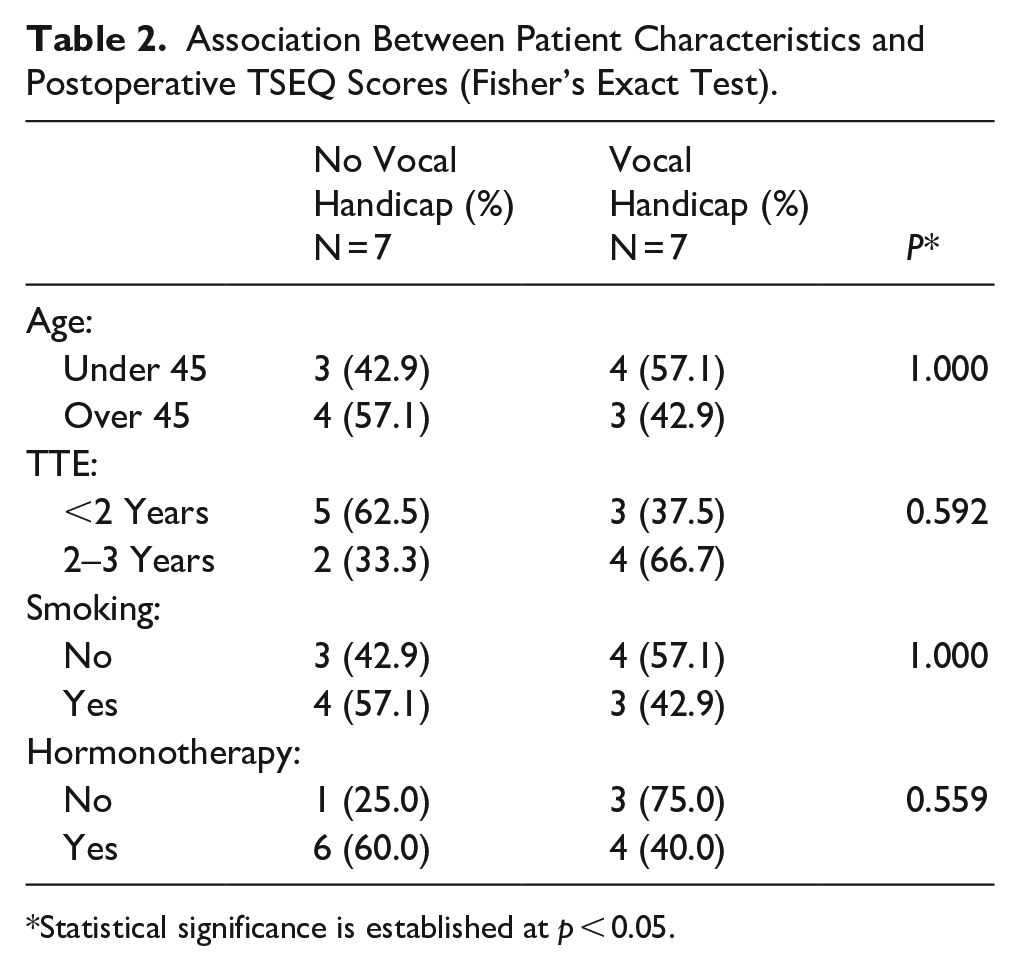
Statistical significance is established at p < 0.05.
Several factors may explain this variability. First, individual differences in vocal fold anatomy, healing response, and postsurgical voice use can influence outcomes. Second, the timing of postoperative assessment may affect patient perception—those surveyed earlier may still be adjusting, while later assessments may reflect habituated expectations. Additionally, subjective satisfaction is multifactorial, shaped not only by pitch but also by resonance, loudness, and voice-related confidence in social contexts.
Our findings must be interpreted within the context of several limitations. The sample size is small, and the response rate was 70%. The TSEQ, while comprehensive, is not a validated instrument, and our study lacked preoperative data or acoustic analysis to objectively measure pitch elevation. Additionally, the lack of a standardized postoperative follow-up schedule may have introduced variability in patient experiences.
Despite these limitations, our experience supports the safety and effectiveness of modified Wendler glottoplasty as a safe and generally effective surgical option for voice feminization in MTF individuals. The technique was well tolerated, and most patients reported increased alignment between their voice and gender identity. Importantly, surgical voice feminization should not be viewed in isolation but rather as one component of a holistic, patient-centered approach that includes counseling, voice therapy, and realistic expectation management.
We recommend that future studies incorporate both objective acoustic measures and validated patient-reported outcomes such as the Voice Handicap Index or the Voice-Related Quality of Life (V-RQOL) scale. A prospective design with pre- and postsurgical data would better clarify the true efficacy of glottoplasty and guide patient selection.
In summary, voice feminization via modified Wendler glottoplasty provides a meaningful improvement in gender congruence for many transgender women. However, surgical outcomes are complex and multifactorial. Our experience highlights the need for holistic, individualized care, informed consent, and realistic preoperative counseling to optimize satisfaction in this unique and growing patient population.
Footnotes
Ethical Considerations
The study was approved by the Institutional Review Board (IRB) of Centre Hospitalier du Luxembourg. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Consent to Participate
Written informed consent was obtained from participants included in the report.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.