
Abstract
Objectives:
This review consolidates all reported cases of facial nerve paralysis (FNP) complicating keratosis obturans (KO), a rare disorder characterized by keratin accumulation in the external auditory canal. The study aims to analyze clinical patterns, diagnostic findings, management outcomes, and prognostic factors to enhance understanding and guide evidence-based management of this underrecognized complication.
Methods:
A comprehensive literature search of PubMed, Web of Science, Scopus, and Google Scholar (inception-December 2024) identified English-language case reports and observational studies linking KO to FNP. Two reviewers independently screened titles/abstracts, performed full-text assessments, and extracted data on demographics, clinical features, imaging, interventions, and outcomes.
Results:
Seven cases (mean age: 32.4 years; 57.1% female) were analyzed. All exhibited left-sided FNP, with House-Brackmann grades III to VI at presentation. Hearing loss (71.4%) and keratin debris on otoscopy (71.4%) were common. High-resolution computed tomography (HRCT) revealed bony erosion (28.6%-57.1%) and soft-tissue involvement (57.1%). Surgical intervention (85.7%), primarily debridement or mastoidectomy, resulted in complete/partial FNP recovery in 85.7% of cases, while conservative management (14.3%) also showed improvement. Limitations of this review included the small number of cases, heterogeneity in management approaches, and lack of standardized outcome measures.
Conclusion:
KO-related FNP, though rare, carries significant morbidity. Timely surgical decompression or conservative care may reverse neural injury, emphasizing early diagnosis via clinical-radiological correlation. The predominance of left-sided involvement and favorable outcomes postintervention warrant further investigation. Prospective studies are needed to establish standardized protocols and validate these findings in larger cohorts.
Introduction
Keratosis obturans (KO) is an uncommon disorder characterized by the accumulation of desquamated keratin within the bony external auditory canal (EAC), often presenting with severe otalgia, conductive hearing loss, and circumferential canal widening.1,2 Historically, KO was conflated with external auditory canal cholesteatoma (EACC) due to overlapping clinical features, but seminal work by Piepergerdes et al. (1980) established distinct diagnostic criteria, emphasizing the absence of osteonecrosis in KO compared to the localized bone destruction seen in EACC.2-4 While KO is typically managed conservatively with aural toilet, rare complications such as facial nerve paralysis (FNP) underscores the potential severity of neglected cases.5,6 FNP as a complication of KO remains exceptionally rare, with only isolated case reports documented to date. The pathogenesis of FNP in KO is hypothesized to stem from chronic inflammatory pressure effects or bony erosion of the fallopian canal, though mechanisms distinct from EACC-associated osteonecrosis.4,5 Notably, while EACC tends to invade the mastoid via posterior canal erosion, KO may extend medially, compromising the tympanic membrane and adjacent structures, including the facial nerve.5,7 Despite these insights, the literature lacks a systematic synthesis of clinical patterns, management outcomes, and prognostic factors in KO-related FNP. This review aims to consolidate all reported cases of KO complicated by FNP, analyzing demographics, clinical features, imaging findings, and therapeutic outcomes. By elucidating the natural history and therapeutic challenges of this rare complication, we seek to enhance diagnostic vigilance and inform evidence-based management strategies.
Methods
A comprehensive literature search was conducted using database from PubMed, Web of Science, Scopus, and Google Scholar from inception through December 2024 to identify English-language studies on FNP as a complication of KO. The search was done in the advanced mode using the Boolean operators “OR” and “AND.” The final advanced search builder showed: (“KO”) OR (“keratosis”) AND (“EAC”) OR (“external auditory meatus”) AND (“facial nerve palsy”) OR (“facial paralysis”) OR (“FNP”) AND (“bony erosion”) OR (“complications”). Each database was searched individually, yielding a total of 56 records. Duplicates were removed, and 22 full-text reports were sought for retrieval. After excluding articles that were not retrievable or did not meet the eligibility criteria, a total of 7 studies were included in the final review as shown in the flowchart (Figure 1).
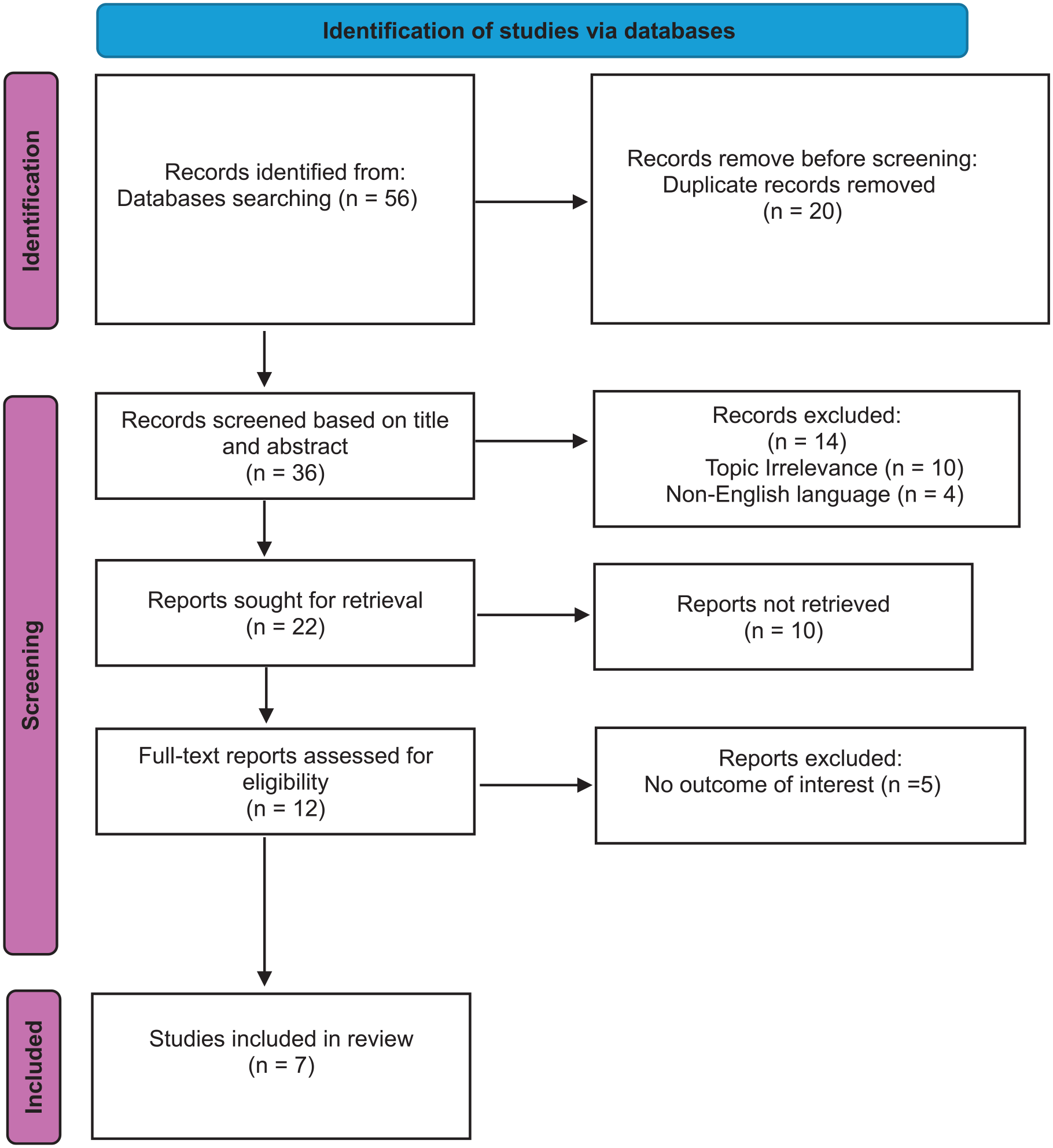
PRISMA flowchart for selection of the articles in the systematic review.
Inclusion criteria encompassed case reports, case series, and observational studies detailing FNP secondary to KO. Exclusion criteria involved non-English articles and studies lacking explicit linkage between KO and FNP. Two reviewers independently screened titles/abstracts, followed by full-text assessment, resolving discrepancies via consensus. The data extraction focused on epidemiology, pathophysiology, comorbidities, diagnostic modalities (e.g., otoscopy, imaging), therapeutic interventions, and outcomes. A Microsoft word sheet was prepared to record the outcomes from the studies included. In addition, the authors followed PRISMA criteria. 8
Results
Our review identified a total of 7 cases of FNP as a complication of KO [4 females (57.1%), 3 males (42.9%), mean age 32.4 years (range: 13-56)]. All cases demonstrated left-sided facial nerve palsy secondary to KO. House-Brackmann grades were reported in 5 cases at presentation [Grade III: 3 cases (42.9%), Grade IV: 1 case (14.3%), Grade VI: 1 case (14.3%)], while grades were unavailable in 2 cases (28.6%) Table 1.
Summarizes Previously Published Case Reports Documenting Facial Nerve Paralysis as a Complication of Keratosis Obliterans.
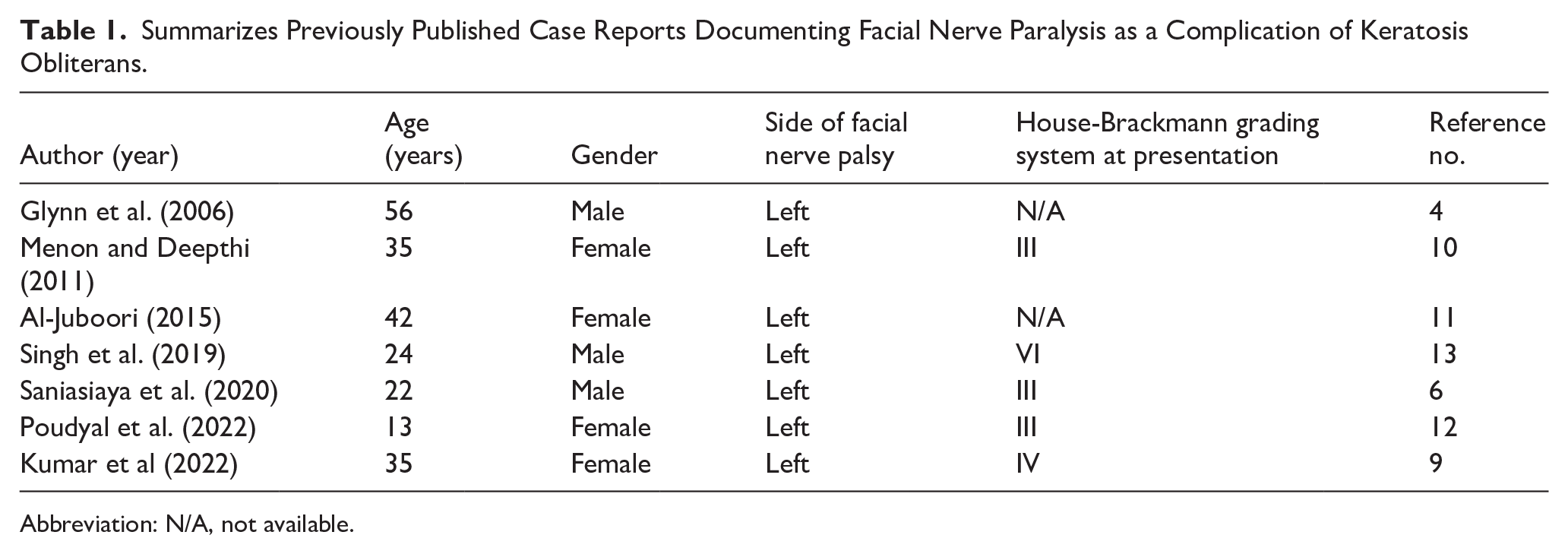
Abbreviation: N/A, not available.
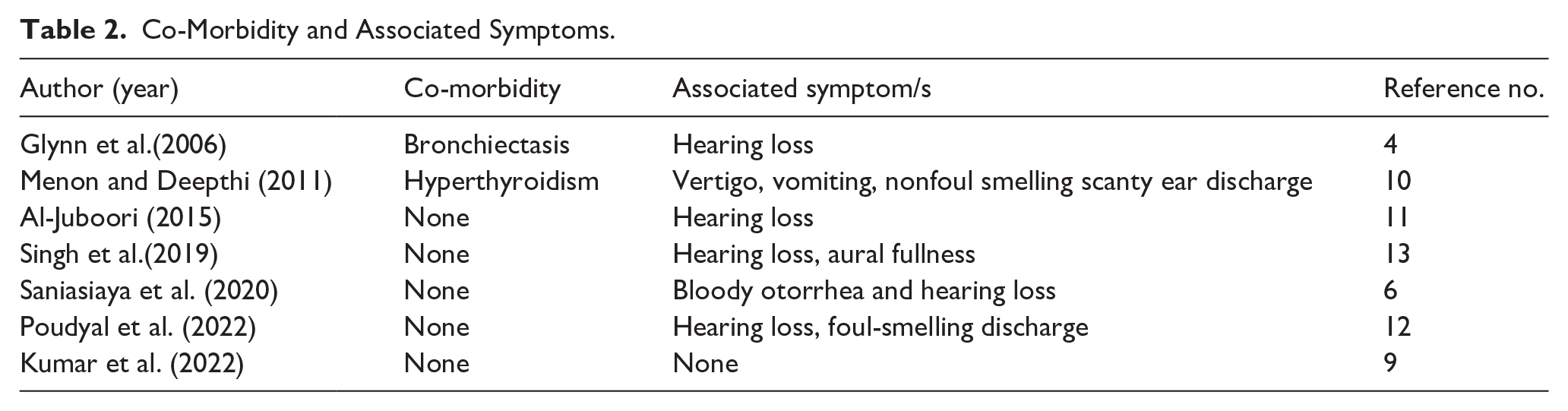
Among the 7 reviewed cases, 2 (28.6%, 2/7) documented co-morbidities: bronchiectasis (14.3%, 1/7) and hyperthyroidism (14.3%, 1/7), while the majority (71.4%, 5/7) reported no co-morbidities. Hearing loss was the most frequent associated symptom, present in 71.4% (5/7) of cases. Other symptoms included vertigo, vomiting, nonfoul-smelling scanty ear discharge, aural fullness, bloody otorrhea, and foul-smelling discharge, each occurring in 14.3% (1/7) of cases. One case (14.3%, 1/7) reported no associated symptoms (Table 2).
Co-Morbidity and Associated Symptoms.
Otoscopic examination revealed the presence of keratinous material/debris in 5 cases (71.4%). Polypoidal masses/tissues were observed in 2 cases (28.6%). Blood-stained discharge was documented in 1 case (14.3%). Otomicroscopy identified EAC widening in 4 cases (57.1%). EAC wall erosion occurred in 2 cases (28.6%). Granulation tissue was noted in 1 case (14.3%). Tympanic membrane perforation was observed in 2 cases (28.6%). Facial nerve involvement was reported in 1 case (14.3%). One case lacked documentation (14.3%; Table 3).
Otoscopic Findings and Otomicroscopy Examination.
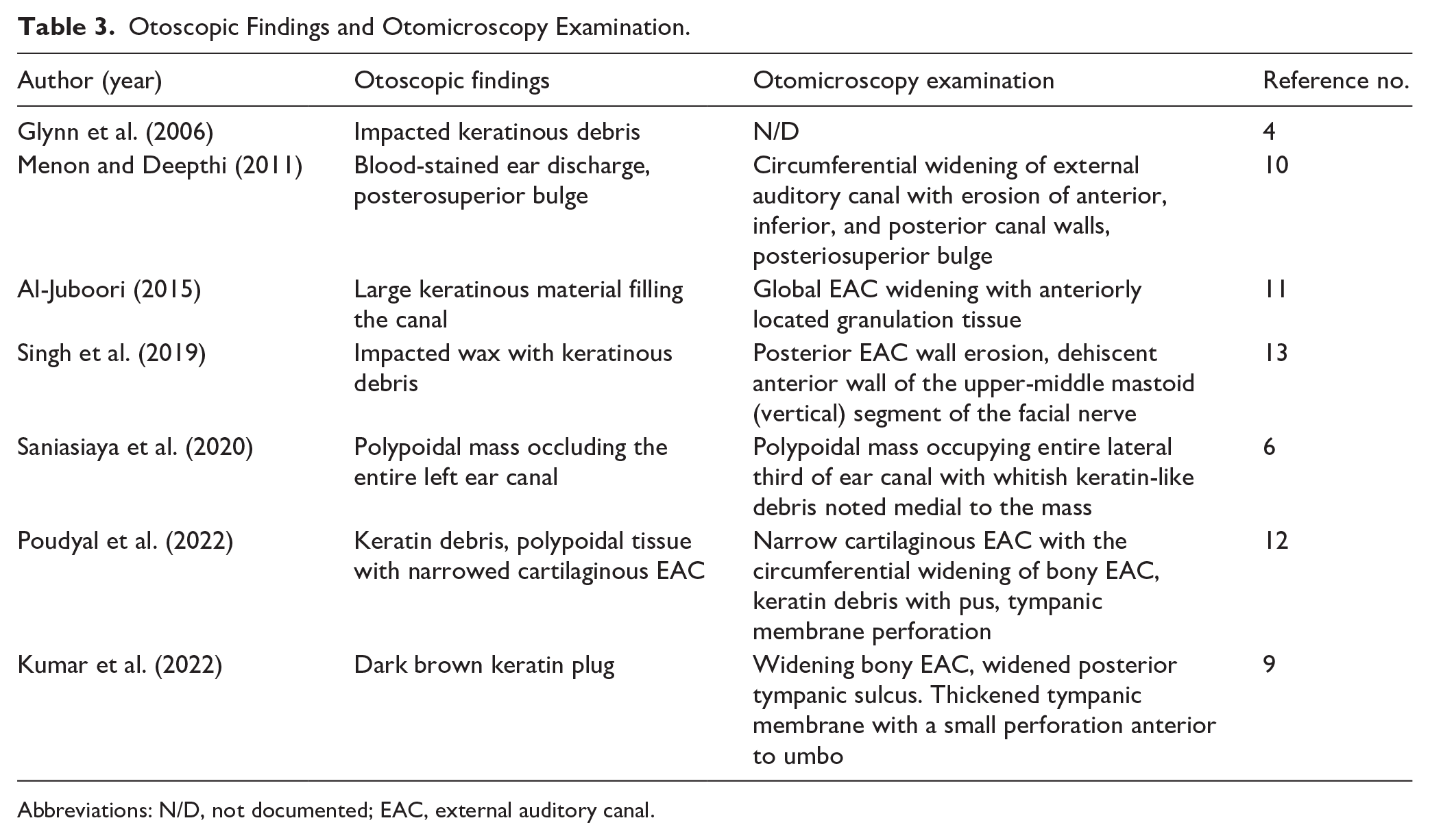
Abbreviations: N/D, not documented; EAC, external auditory canal.
The high-resolution computed tomography (HRCT) findings revealed posterior EAC wall erosion. In 1 case (14.3%), scutum erosion in 2 cases (28.6%), annulus erosion in 1 case (14.3%), and temporal bone erosion in 1 case (14.3%). Soft-tissue density was observed in 4 cases (57.1%), ballooned EAC in 3 cases (42.9%), and thickening of the EAC in 1 case (14.3%). Mastoid involvement was noted in 2 cases (28.6%), while facial canal dehiscence/pressure was identified in 2 cases (28.6%). Additionally, dural plate dehiscence was documented in 1 case (14.3%), and attic involvement was observed in 2 cases (28.6%; Table 4).
HRCT Findings.
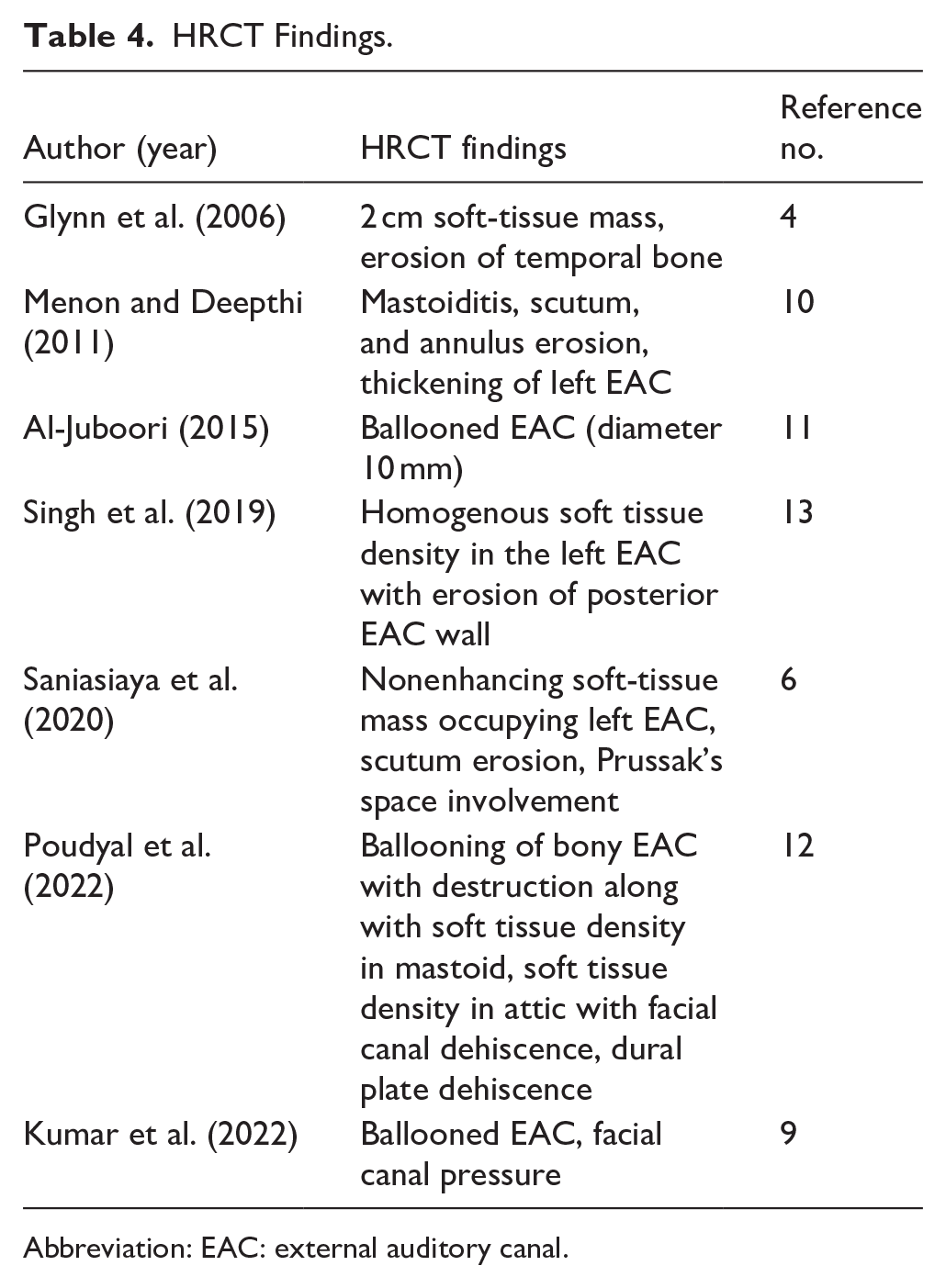
Abbreviation: EAC: external auditory canal.
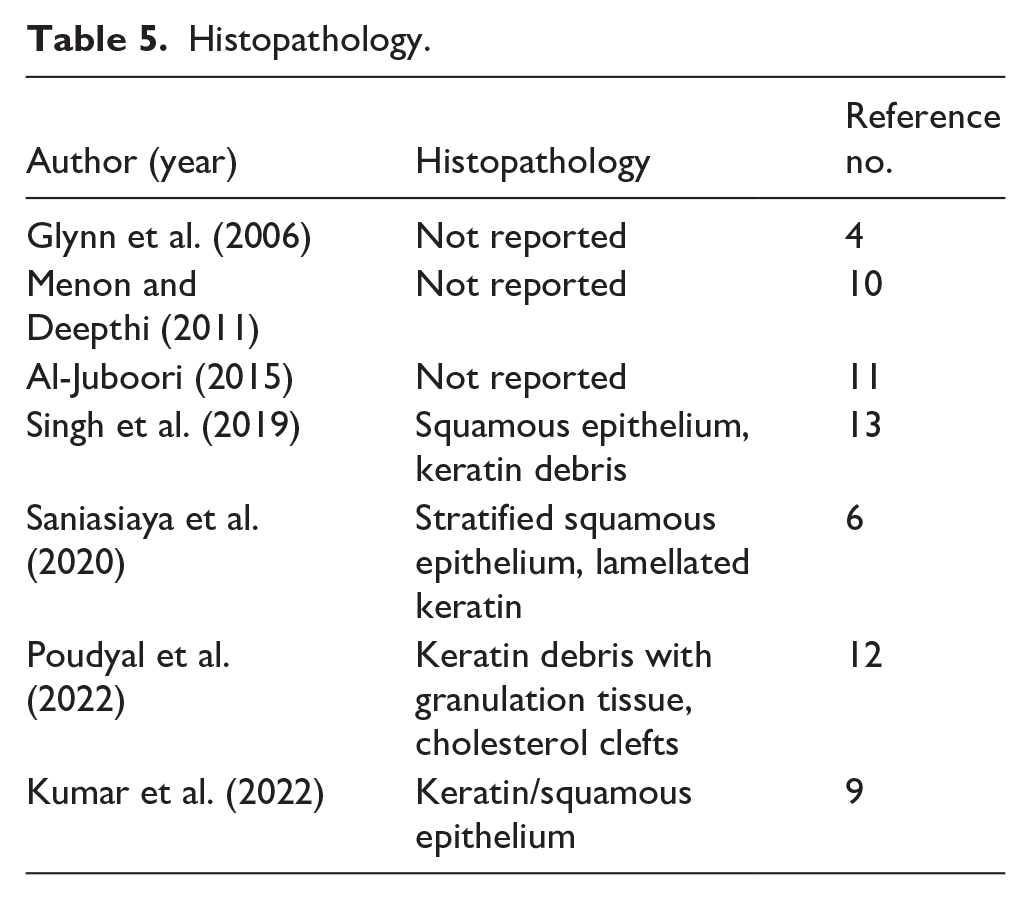
Regarding histological diagnosis, 4 cases (57.1%) reported it, while 3 cases (42.9%) did not report undergoing the histological examination (Table 5).
Histopathology.
Regarding management strategies, surgical management was performed in 6 cases (85.7%), while conservative management was adopted in 1 case (14.3%). As for outcomes, 3 cases (42.9%) reported complete recovery of the facial nerve injury, 3 cases (42.9%) reported partial improvement of the injury, and 1 case did not report on this aspect. Additionally, no cases reported worsening of the facial nerve injury following treatment (Table 6).
Management Strategies and Outcomes.
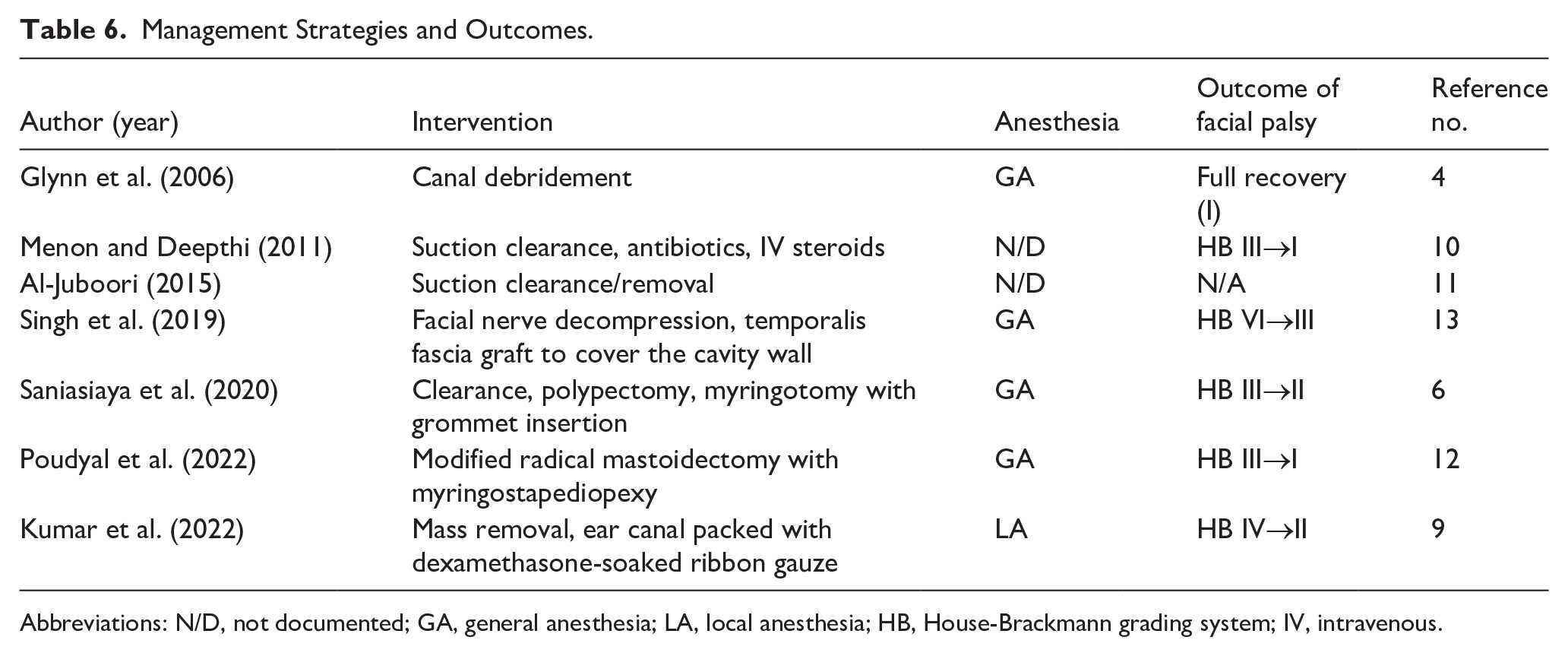
Abbreviations: N/D, not documented; GA, general anesthesia; LA, local anesthesia; HB, House-Brackmann grading system; IV, intravenous.
Discussion
FNP as a complication of KO represents an exceptionally rare clinical entity, with only 7 documented cases to date. This review consolidates the existing evidence to elucidate clinical patterns, therapeutic outcomes, and potential pathophysiological mechanisms underlying this complication. The findings highlight critical insights into the interplay between KO progression and facial nerve integrity, while underscoring the challenges in managing such cases due to their rarity and heterogeneous presentations.
Clinical Characteristics
The predilection for left-sided FNP across all cases is notable, though the small sample size precludes definitive conclusions regarding anatomical or pathophysiological laterality. This observation may reflect coincidental reporting bias rather than a true biological propensity. The mean age of presentation (32.4 years) aligns with prior descriptions of KO as a condition predominantly affecting younger adults, likely due to cumulative keratin accumulation over time. The absence of significant comorbidities in most cases (71.4%) suggests that KO-related FNP arises primarily from local mechanical or inflammatory effects rather than systemic predispositions. However, the association with bronchiectasis and hyperthyroidism in 2 cases warrants further exploration into potential shared pathways, such as chronic inflammation or immune dysregulation.
Pathophysiology
The pathogenesis of FNP in KO remains speculative but likely involves direct pressure effects from keratin debris, chronic inflammation, or bony erosion of the fallopian canal. Unlike EACC, which erodes bone via osteoclastic activity, KO-associated FNP may result from gradual mechanical compression or reactive osteitis.2,5 Regarding radiological imaging, HRCT findings in this review support this hypothesis, with posterior EAC wall erosion (14.3%), scutum involvement (28.6%), and facial canal dehiscence (28.6%) implicating structural compromise as a key contributor. The extension of KO medially toward the tympanic membrane and adjacent structures may further exacerbate neural injury, particularly in neglected cases. Notably, the absence of osteonecrosis in KO, a hallmark distinction from EACC, underscores the need for tailored diagnostic and therapeutic apprClinic. 5
Diagnostic Challenges
Otoscopic and otomicroscopic findings, such as keratinous debris (71.4%), EAC widening (57.1%), and granulation tissue (14.3%), reinforce the importance of meticulous clinical evaluation in suspected cases. HRCT emerged as a critical tool for identifying bony erosion and soft-tissue involvement, though its utility was underreported in earlier cases. Histopathological examination of KO was inconsistently pursued (57.1%), reflecting either diagnostic confidence based on clinical-radiological correlation or resource limitations. This variability underscores the need for standardized protocols to ensure accurate differentiation from EACC and other mimics.
Management
Surgical intervention, predominantly canal debridement or mastoidectomy (85.7%), achieved complete or partial FNP recovery in 85.7% of cases, suggesting that timely mechanical relief of neural compression is pivotal. Conservative management (14.3%), while less common, also yielded improvement, highlighting the potential role of inflammation reduction in milder presentations.
In addition, the favorable outcomes observed across interventions emphasize the importance of individualized treatment plans guided by disease extent and neural integrity.
Follow-Up Outcomes
The House-Brackmann grading at presentation correlated loosely with outcomes, as even severe initial deficits (eg, Grade VI) showed improvement postintervention. This suggests that neural injury in KO may be partially reversible with timely decompression, contrasting with irreversible damage seen in EACC-associated osteonecrosis. The rapid recovery of HB grades postsurgery (eg, Grade III to I within weeks) suggests that FNP in KO is often neuropraxic rather than axonotmetic. However, delayed presentations (>6 months) correlate with incomplete recovery, emphasizing the critical window for intervention. Serial electroneuronography could stratify patients needing early decompression versus conservative management. This review is inherently constrained by its reliance on case reports, which introduce publication bias and variability in data reporting. The absence of controlled studies precludes causal inferences, and the predominance of surgical outcomes may overestimate intervention efficacy. While KO-related FNP is rare, its potential for severe morbidity necessitates heightened clinical vigilance. Early recognition through combined clinical, radiological, and histopathological assessment, coupled with tailored surgical or medical intervention, appears critical for optimizing outcomes. This review underscores the need for collaborative research to establish evidence-based guidelines and improve prognostication in this understudied complication.
Limitations
Limitations of this review include the small number of reported cases, which restricts the generalizability of finding and precludes conducting statistical analysis. The heterogeneity in management strategies especially in surgical techniques—ranging from polypectomy to facial nerve decompression—reflects the lack of consensus on optimal management. Additionally, the lack of uniform outcome measures, such as consistent use of House-Brackmann scale or long-term follow-up protocols, limits the ability to assess and compare treatment efficacy across cases. Prospective multicenter registries could address these limitations by standardizing data collection and enabling longitudinal follow-up. Investigations into molecular mediators of inflammation in KO may clarify its progression to FNP and identify targets for adjunctive therapies. Additionally, comparative studies between KO and EACC could refine diagnostic criteria and management algorithms.
Conclusion
This review consolidates the limited evidence on FNP as a complication of KO, a rare condition with only 7 reported cases. Given the small sample size, the predominance of left-sided FNP and high recovery rates should be interpreted cautiously, as these findings may not be generalizable and could be influenced by publication bias. Additionally, inconsistent reporting of histopathological findings across cases limits definitive insights into the pathology involved. Future case reports should prioritize obtaining histologic confirmation to differentiate KO from entities such as EACC, which will improve diagnostic clarity and our understanding of disease mechanisms. Surgical intervention, primarily canal debridement, led to complete or partial recovery in most cases, highlighting the potential reversibility of neural injury with timely treatment. Nevertheless, the reliance on case reports and lack of long-term data underscores the need for prospective studies to validate these findings and establish evidence-based guidelines. In summary, this review highlights the rarity of FNP in KO and the critical role of early diagnosis and intervention in optimizing outcomes. Continued research is essential to enhance our understanding and management of this uncommon complication.
Footnotes
Ethical Considerations
This study is a systematic review based on already published data, where no human participants are involved; therefore, ethical approval not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statements
Data are embedded in the manuscript as it’s secondary research.