
Abstract

Significance Statement
Peripheral facial paralysis develops as a result of lower motor neuron damage to the facial nerve. The etiology is often unknown. Peripheral facial paralysis is commonly observed in patients with multiple sclerosis (MS). A rare cause of peripheral facial paralysis is the facial colliculus syndrome. Central nervous system imaging is highly useful for elucidating the etiology in patients with peripheral facial paralysis.
A 12-year-old male patient, without known prior medical conditions, presented complaints of double vision, inability to close the right eyelid, drooping in the corner of the mouth, and facial asymmetry that started 3 days ago. Physical examination revealed peripheral-type facial palsy and diplopia. The patient underwent cerebral magnetic resonance imaging. Multiple hyperintense plaques, located perpendicular to the corpus callosum, were observed in fluid-sensitive and T2-weighted sequences (Figure 1A and B). In the axial fluid-sensitive image at the level of the pons, an increased intensity of the signal was observed in the facial colliculus (Figure 1C). On the diffusion-weighted image, the nuclei and tracts of the abducens and facial nerves were demonstrated (Figure 2A). The same image showed an increase in signal intensity in the facial nerve tract (Figure 2B). In the axial fluid-sensitive image, increased signal intensity was observed in the nuclei of the abducens and facial nerves (Figure 2C). After considering the current findings and imaging, the patient was diagnosed with MS and facial colliculus syndrome.
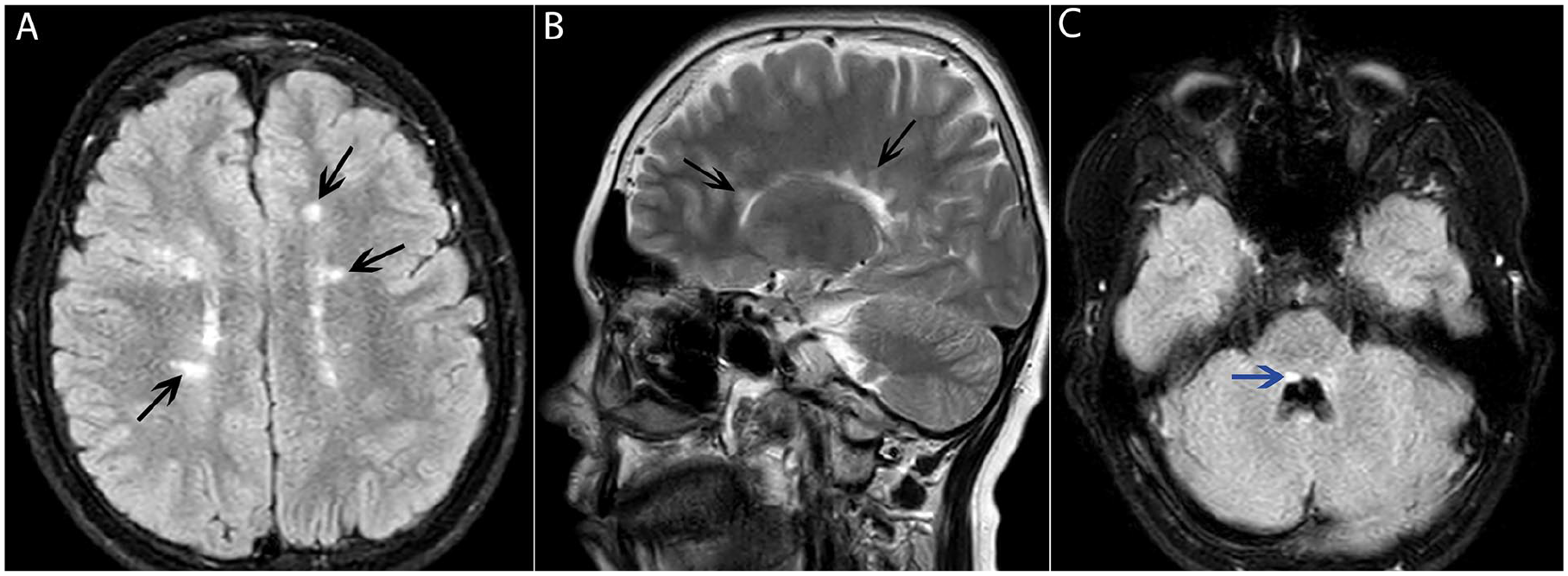
(A) Axial FLAIR image showing multiple hyperintense plaques in white matter (black arrows). (B) Sagittal T2-weighted image showing multiple hyperintense plaques in white matter (black arrows). (C) Axial FLAIR image passing through the pons showing hyperintense signal in the facial colliculus (blue arrow).
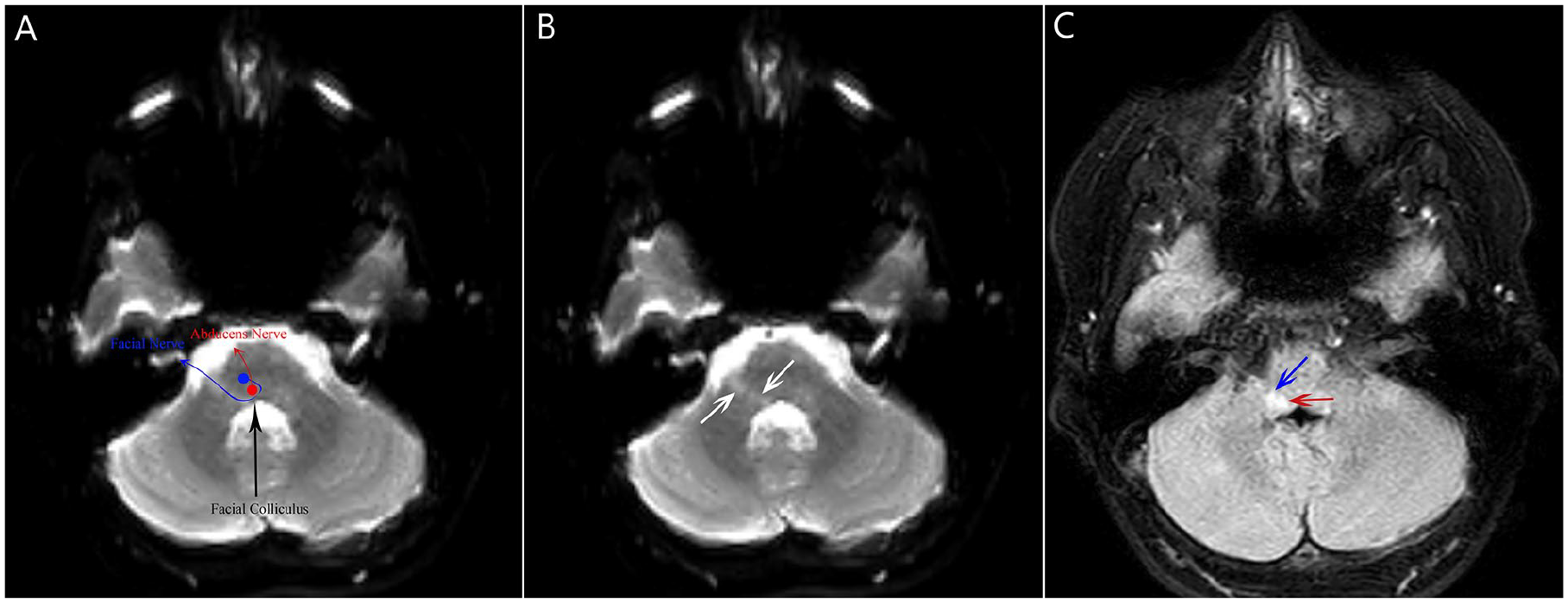
(A) Diffusion-weighted imaging at the pons level demonstrating the nuclei and tracts of the abducent and facial nerves. (B) Diffusion-weighted image showing hyperintense signal along the facial nerve tract (white arrow). (C) Axial FLAIR image showing hyperintense signal in the abducent (red arrow) and facial (blue arrow) nerve nuclei.
Peripheral facial palsy is a common clinical condition seen by otolaryngologists, typically the result of damage to the lower motor neuron of the facial nerve. The etiology is often unknown, but known causes include trauma, malignancy, pregnancy, and autoimmune diseases. 1 MS is a demyelinating, autoimmune, and neurodegenerative disease that affects the central nervous system. 2 In a study by Di Stadio and Bernitsas, the prevalence of facial palsy in MS patients was found to be 7%. 3 Facial palsy can present as the initial symptom in MS patients or develop later during follow-up. In a study by Soltanzadeh et al, 5% of MS patients had facial palsy and 2.1% of these patients presented facial palsy as their initial symptom. 4 In a study by Etemadifar et al, 3.27% of 2260 MS patients had facial palsy. Among these 74 patients, 72 had peripheral facial palsy and 2 had central facial palsy. 5
The facial colliculus is the anatomical term for the bump created by the abducens nerve nucleus and the surrounding facial nerve fibers in the intrapontine area at the base of the fourth ventricle. The clinical signs and symptoms of facial colliculus lesions are primarily the result of damage to the abducens nerve nucleus, the facial nerve fibers surrounding the abducens nucleus, the formation of paramedian pontine reticular formation, and the medial longitudinal fasciculus. Facial colliculus syndrome is characterized by ipsilateral peripheral facial palsy, ipsilateral lateral rectus palsy, and often conjugate gaze palsy due to the involvement of the contralateral medial rectus muscle. 6 The etiology of facial colliculus lesions in young patients includes tumors, viral infections, and demyelinating processes, while ischemic factors are more common in older patients.6,7 We presented a case of an MS case with peripheral facial palsy, a rare cause of which was facial colliculus syndrome.
Footnotes
Author Contributions
Gökhan Polat: writing—review and editing (lead). Muhammet Sefa Acar: writing—review and editing (supporting).
Consent for Publication
We declare that written informed consent for the publication of patient information and images was provided by the patient’s legal representative.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.