
Abstract

Significance Statement
The coexistence of a sphenochoanal polyp and isolated sphenoidal fungal rhinosinusitis is not commonly encountered. While it is not unusual to have superadded fungal infestation in a dark, hypoventilated sinus with chronic inflammation (mucositis, polyp), a primary sphenoidal fungal rhinosinusitis can potentially lead to florid mucosal thickening to produce a polypoid exvagination through the ostium. The disease involution depends upon several factors, like the patient’s comorbidities and immune status, appropriate medical management, and behavior of the primary disease entities. This interesting clinical vignette illustrates this unusual coexistence from endoscopic and radiologic perspectives, discusses its possible etiopathology, and observes how it influences the surgical plan.
Text Proper
A 57-year-old man presented with left-sided nasal blockage, occasional lumpy sensation in the throat, deep-seated headache, and foul breath for 3 years. Temporary symptomatic relief could be achieved through a short-term nasal corticosteroid spray and antibiotics. There was no history of purulent nasal discharge and epistaxis. The patient was non-diabetic and was in good health.
Diagnostic naso-endoscopy revealed a pale polypoid mass almost occluding the left choana, and a thick, greenish blob of crust in the ipsilateral sphenoethmoidal recess. Streaks of purulent discharge emanated from the sinus behind the crusts and trickled down along the posterior pharyngeal wall. The rest of the internal structures in both nasal cavities were unremarkable. An attempt at dislodging the crust led to the expulsion of fungal debris and was associated with bleeding from the surrounding inflamed mucosa and granulation tissue. No further attempt at exploration was made at this time. A non-contrast computed tomography (CT) scan of the nose and paranasal sinuses (Figure 1) done in an outside facility 10 weeks earlier showed almost complete opacity in the left sphenoid sinus that extended as a polypoid mass through the ostium into the nasopharynx, occluding the choana.
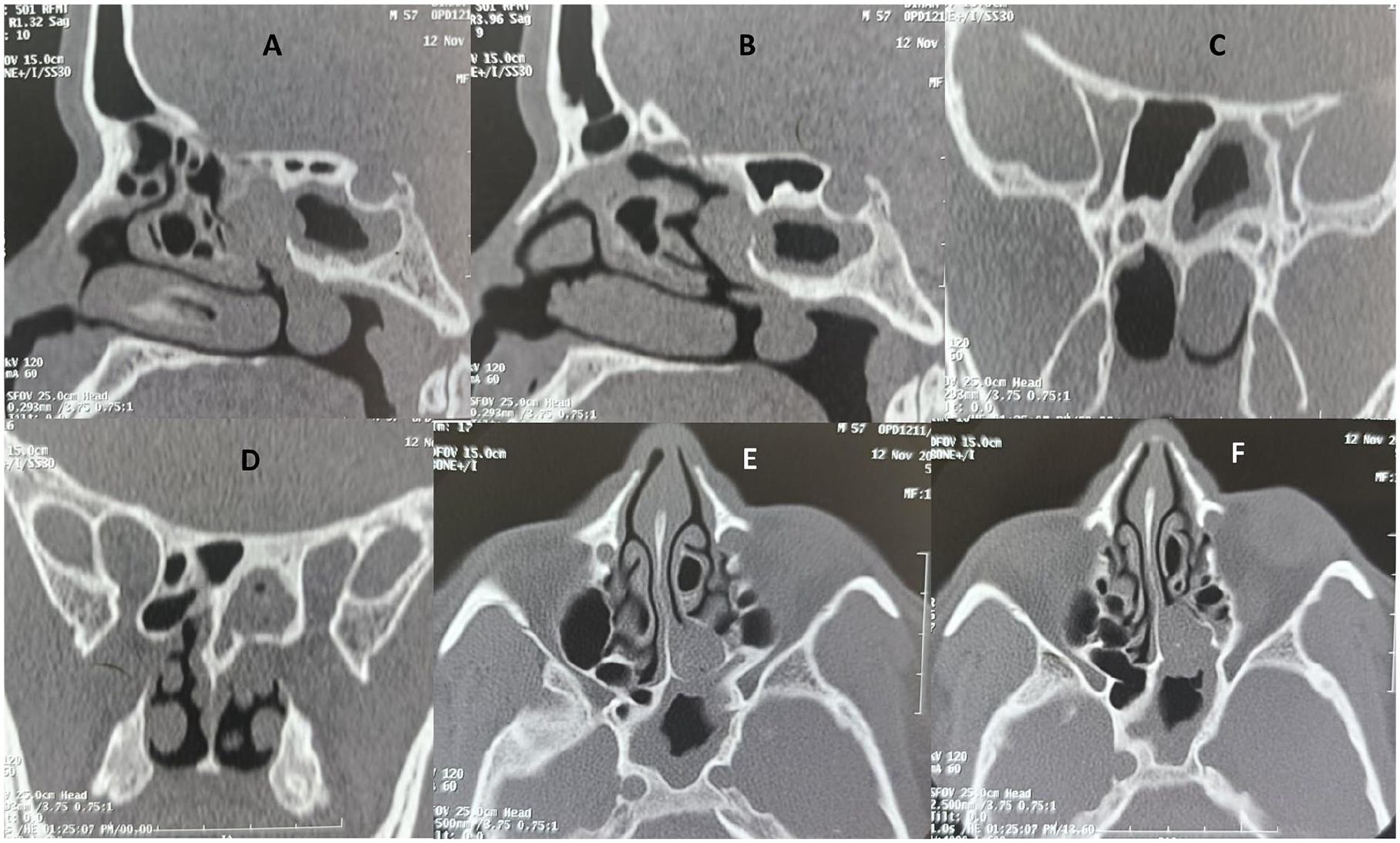
The non-contrast CT scan of the nose and paranasal sinuses done before the appropriate medical management showed the sphenochoanal polyp involving the left (dominant) sphenoid sinus. At that time, there was no evidence of the double density sign characteristic of allergic fungal rhinosinusitis. (A, B) Parasagittal reconstruction cuts; (C, D) coronal cuts; (E, F) axial primary cuts; all are bone windows. CT, computed tomography.
The patient was put on appropriate medical therapy (2 weeks of co-amoxiclav at 625 mg thrice/day, intranasal corticosteroids, oral prednisolone at 1 mg/kg for 3 weeks in tapering doses, and antihistamine). This time, non-contrast magnetic resonance imaging (MRI) was advised to delineate the mucosal health of the sphenoid sinus and to avoid a second radiation exposure. It revealed a T2 hyperintense polypoid lesion in the left choana, with prominent mucosal thickening of the ipsilateral sphenoid sinus (Figure 2). Much of the left sphenoid was now free; however, areas of heterogeneity were noted on its posterior wall and near its ostium, occluding its opening into the sphenoethmoidal recess. A presumptive diagnosis of sphenochoanal polyp coexisting with isolated sphenoidal fungal rhinosinusitis was rendered, and the patient was prepared for endoscopic sinus surgery.

The non-contrast MRI of the nose and paranasal sinuses (A–D, in craniocaudal order, T2-weighted primary axial cuts) done following the appropriate medical management showed the choanal part of the sphenochoanal polyp (D) with mucosal thickening of the left sphenoid sinus (A–C). The sinus ostium could be seen already dilated (B). Due to the appropriate medical management, much of the intra-sinus component of the sphenochoanal polyp underwent resolution. However, at this point of time, heterogeneous opacities, suggestive of fungal infestation, could be seen in the posterosuperior and inferolateral aspects of the left (dominant) sphenoid sinus, encroaching the ostium (A, C). MRI, magnetic resonance imaging.
At surgery, adequate working space in the left sphenoethmoidal recess was created by lateral partial turbinoplasty of the middle turbinate concha bullosa, allowing its gentle lateralization. The crust in the sphenoethmoidal recess was seen to plug the sphenoid ostium completely; its removal led to expulsion of dense fungal debris from the sinus. The sphenoid ostium was unusually dilated, and the mucosa was grossly edematous and infected, with patches of granulations and pus adhered to its walls, although no allergic mucin was noted. Complete removal of the fungal debris from the sinus was ensured by thorough, repeated normal saline irrigation and, finally, by visualizing its interior with a 70° endoscope. The choanal polyp was free on all sides, and was attached to the inferior edge of the sphenoid ostium and partly to the anterior sphenoid face. A microdebrider was used to detach the polyp, widen the ostium further, and trim its edges by removing the overhanging granulations and edematous mucosa. The details of the diagnostic nasal endoscopy and endoscopic surgery have been well illustrated in Figure 3 and in a short operative Supplemental Video.

The diagnostic nasal endoscopy showed crusts and fungal debris occluding the sphenoid ostium in the left sphenoethmoidal recess (A). A streak of pus could be seen emanating from the sphenoid sinus behind the fungal debris (B), which when followed through the anterior face of the sinus, led to the sphenochoanal polyp (C, D). The fungal crusts plugging the sinus ostium were removed, and the sinus was cleared of dense fungal debris through meticulous suction-irrigation (E, F). The sphenoid ostium was seen unusually wide (presumably due to the sphenochoanal polyp), and the sinus mucosa was edematous, infected, and with granulation tissues (G). The sinus ostium was further widened and its edges smoothened, and the choanal polyp’s attachment on the anterior face of the sinus was debrided (H).
This patient presented with an unusual co-existence of isolated sphenoidal fungal rhinosinusitis and ipsilateral sphenochoanal polyp. Both are established clinical entities and well documented in the literature, although a sphenochoanal polyp is relatively uncommon compared to an antrochoanal polyp and is sparsely reported.1,2 However, the intriguing point to discuss here is whether the coexistence is merely coincidental or can be explained through a cause-effect relationship. The most consistent chief complaint of the patient was indeed unilateral nasal obstruction; however, its duration and onset did not differ significantly from those of the other less bothersome symptoms. So, the clinical history was of limited help in determining the primary lesion between the 2.
A sphenochoanal polyp originates from an infected sphenoid sinus with grossly edematous mucosa popping out through the sinus ostium, widening it in the process. These features were prominent on imaging in this patient and were also noticed at surgery. It is not unusual to have superadded fungal colonization as a fungal ball in a poorly ventilated, infected sphenoid sinus. 3
By contrast, a primary fungal rhinosinusitis involving the sphenoid sinus can occlude the ostium, leading to secondary mucosal changes within the sinus (edema and granulations) and polypoid outpouching as a choanal polyp. The intra-sinus mucosal changes noticed in this patient were characteristic of a long-standing fungal infestation. Also, primary fungal rhinosinusitis is mostly encountered in older patients who have poor mucociliary transport.2,4 However, since the patient was non-diabetic and had no evidence of immunosuppression, it is difficult to explain the chronicity of a florid, primary fungal infestation in an otherwise virgin sinus environment, leading to intermittent symptoms. Also, the CT scan done prior to the appropriate medical management did not show the double density sign that characterizes allergic fungal rhinosinusitis, nor was any allergic mucin found at surgery. In fact, the imaging (both CT and MRI) showed the left sphenoid ostium already dilated, suggesting a choanal polyp. Interestingly, the isolated fungal rhinosinusitis in this patient involved the dominant sphenoid sinus, which contradicts the observation by Meerwein et al. 2 Thus, it is less likely that the primary pathology could be a fungal sinusitis. The possible impaired mucociliary transport due to the infected intra-sinus component of the sphenochoanal polyp, and the resultant mucus trapping, congestion, and edema noted at endoscopy, produced an environment conducive for superadded fungal infestation.
This dilemma seems logical because the sinus component of the sphenochoanal polyp was characteristically not evident at surgery, and the entire sinus was filled with fungal debris and associated mucosal changes (edema, granulations, purulence). Possibly, the appropriate medical therapy reduced the volume of the intra-sinus polyp, which was evident on comparing the mucosal health of the left (dominant) sphenoid sinus through images before and after the medical therapy (CT and MRI scans, respectively). Besides prominent mucosal thickening, blobs of heterogeneity suggesting fungal debris were noted in the post-medication MRI, within the depth of the left sphenoid sinus, on its posterior and anterior walls, partially occluding the ostium. However, with the absence of the characteristic CT features of fungal rhinosinusitis, and visualization of extensive fungal debris on diagnostic nasal endoscopy 7 weeks later, and subsequently in the MRI following further 3 weeks of medical management, it seems logical that the sphenochoanal polyp was indeed the primary lesion. The fungal component was a superadded colonization rather than representing primary allergic rhinosinusitis; it occupied a poorly ventilated, dark sinus (albeit the dominant one) only later, almost replacing the sinus component of the sphenochoanal polyp.
The coexistence of a sphenochoanal polyp and ipsilateral, isolated sphenoidal fungal rhinosinusitis is not routinely encountered. The clinical presentation may be misleading and may not contribute to the diagnosis. The imaging too should be interpreted with caution as it is subject to extrinsic disease-modulating factors (medical therapy) and the unpredictable involution of the disease with time. Superadded fungal infection may affect a hypoventilated (generally non-dominant) diseased sinus irrespective of any comorbidities and can alter the surgical plan. 2
The unusual coexistence in this patient was helpful to the endoscopic surgeons on 1 aspect—the need for creating a wider sinus opening for fungal rhinosinusitis was partly served by the natural ostium-widening property of the sphenochoanal polyp!
This manuscript contains a short surgical video for review, uploaded with the manuscript submission system as a supplementary file. To accommodate the limited capacity of uploading content, the video is in low resolution (720p). The higher resolution (1080p) video file is available with the Communicating Author and can be produced on demand.
Footnotes
Ethical Considerations
The clinical and surgical principles adopted for the management of his condition complied with the ethical standards of relevant national and institutional guidelines on human experimentation, as laid down in the Declaration of Helsinki, 1975, as revised in 2013, at Fortaleza, Brazil.
Consent for Publication
Written informed consent has been obtained from the patient to publish this clinical document.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The clinical data of the patient illustrated in this article are available from the authors and can be reproduced on request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.