
Abstract
Adult rhabdomyoma is a rare benign tumor of striated muscle origin, predominantly occurring in the head and neck region of middle-aged males. Herein, we present a unique case of a 78 year-old woman with a 7.3 × 3.8 × 5.4 cm supraglottic rhabdomyoma causing progressive dysphagia, dysphonia, and life-threatening airway obstruction over 5 to 7 years. Despite its benign histology, the tumor’s size and location necessitated emergent airway stabilization and partial resection. This report highlights the tumor’s atypical presentation in an elderly female, its unprecedented dimensions, and the clinical challenges of managing large, obstructive benign neoplasms.
Background
Adult rhabdomyoma is a rare benign mesenchymal tumor of striated muscle origin, classified into 3 subtypes: adult, fetal, and genital. 1 While cardiac rhabdomyomas—strongly associated with tuberous sclerosis complex—are most common in pediatric populations, extracardiac adult rhabdomyomas are exceptionally rare, with fewer than 200 cases reported globally. 2 These tumors arise from striated muscle and are histologically distinct from their malignant counterpart, rhabdomyosarcoma, due to their lack of mitotic activity, necrosis, and infiltrative growth.3,4 While rhabdomyosarcoma predominantly affects children and adolescents, adult rhabdomyoma is most frequently diagnosed in middle-aged males (40-70 years), with a striking male-to-female ratio of 3 to 4:1. 5 Approximately 80% of extracardiac cases occur in the head and neck region, particularly the pharynx, larynx, and oral cavity, where they often present as asymptomatic, slow-growing masses. 1
The indolent nature of adult rhabdomyoma contributes to delayed diagnosis, as patients may remain asymptomatic until the tumor exerts mass effect on critical structures. The average reported size is 1 to 4 cm, with larger tumors (>5 cm) being exceptionally rare. 6 Clinical presentation varies depending on location: Laryngeal tumors may cause dysphonia, dysphagia, or airway compromise, while pharyngeal lesions can lead to obstructive sleep apnea or globus sensation. 7 Histologically, adult rhabdomyoma is often characterized by large polygonal cells with eosinophilic cytoplasm, cytoplasmic vacuoles (“spider cells”), and delicate intervening fibrosis. 2 Immunohistochemistry plays a pivotal role in differentiation from mimics such as granular cell tumors (S100+) and rhabdomyosarcoma (myogenin+, Ki-67+). 8
This case defies established demographic and clinical norms. The patient is an elderly female, a demographic representing fewer than 20% of reported cases. 3 Furthermore, the tumor’s unprecedented size (7.3 cm) and rapid symptomatic progression over 6 months contrast sharply with the indolent behavior typically associated with rhabdomyomas. 5 Such presentations are scarcely documented, with fewer than 10 prior-documented cases describing laryngeal rhabdomyomas exceeding 5 cm. 6 This report underscores the need to recognize rhabdomyoma in atypical populations and settings, particularly when clinical features mimic malignancy.
Case Presentation
A 78 year-old woman with a history of asthma, fibromyalgia, and generalized anxiety disorder presented with a 5 to 7 year history of progressive dysphagia, hoarseness, snoring, and unintentional weight loss. Over 6 months, her symptoms acutely worsened, leading to a 30 pound weight loss, positional airway compromise, and a muffled “hot potato” voice. She denied hematemesis, hemoptysis, or prior radiation exposure.
Initial imaging with Computed Tomography (CT) soft tissue neck on hospital presentation on Day 0 revealed a 7.3 × 3.8 × 5.4 cm heterogeneously-enhancing mass centered in the supraglottic region, causing severe airway narrowing (Figure 1a). Same day, fiberoptic laryngoscopy demonstrated a smooth, mucosa-covered lesion obstructing the supraglottis, with transglottic extension to the right side. Biopsies demonstrated polygonal cells with eosinophilic cytoplasm and “spider cells,” while immunohistochemistry (desmin+, S100−, pankeratin−) confirmed adult rhabdomyoma (Figure 1b-d).
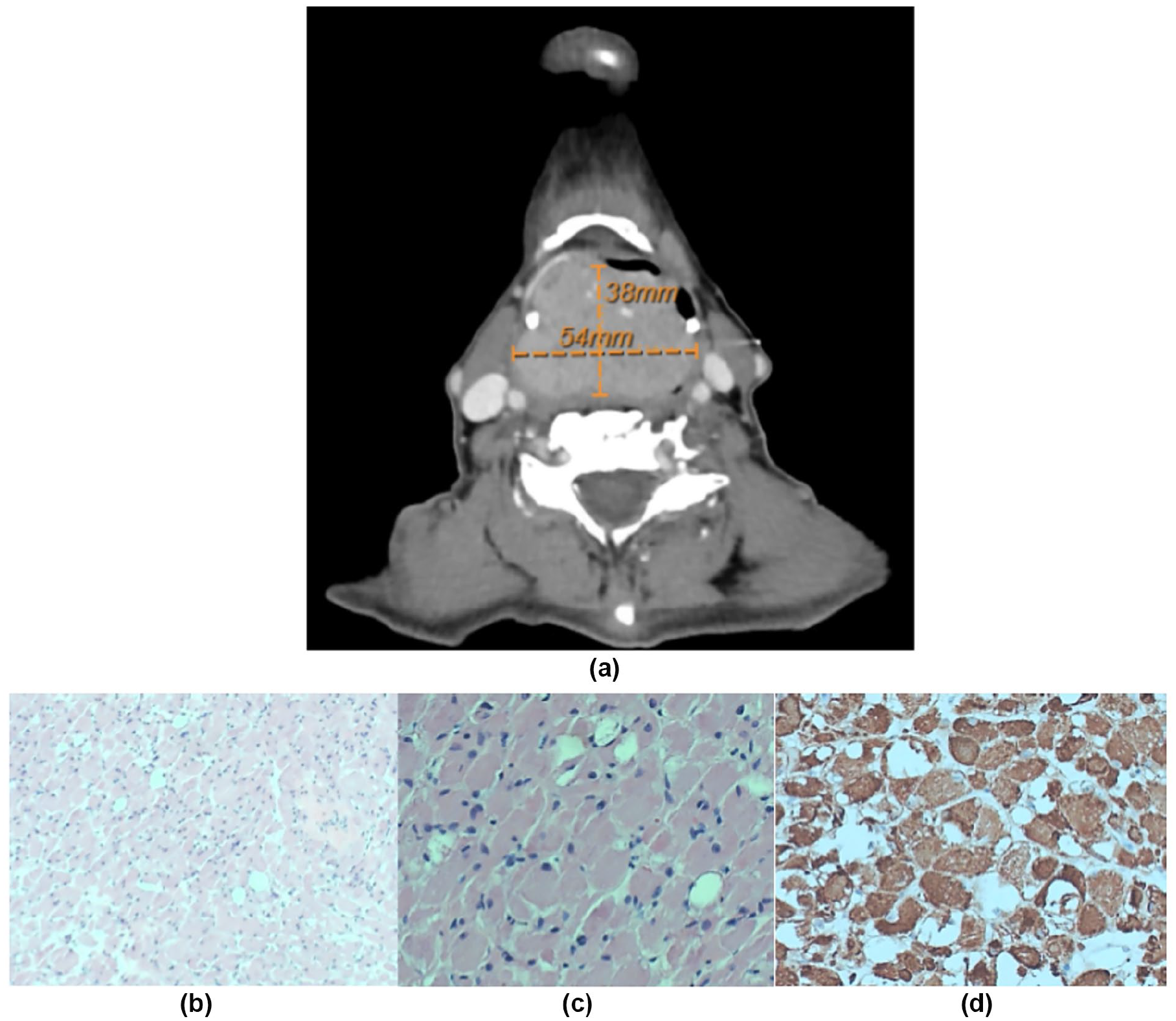
(a) Large, heterogeneously-enhancing supraglottic mass measuring 7.3 × 3.8 × 5.4 cm, causing near-total airway obstruction. The mass extends transglottically to the right, correlating with the patient’s dysphonia and positional stridor. (b) Low-power view (4× magnification) of the patient’s adult rhabdomyoma with polygonal tumor cells. The cells have abundant eosinophilic cytoplasm and are separated by delicate intervening fibrosis, demonstrating the general architecture of the tumor. These “spider cells” exhibit cytoplasmic vacuolization with radiating filaments (best visualized at higher powers), which are pathognomonic for adult rhabdomyoma. (c) A higher power view (10× magnification) focusing on the characteristic “spider cells.” This image provides additional detail on these cells and the delicate intervening fibrosis, emphasizing the diagnostic features at high magnification. (d) Immunohistochemical staining image showing strong desmin positivity (brown coloration) in the tumor cells, confirming skeletal muscle differentiation.
On Day 13, the patient underwent emergent awake tracheostomy and percutaneous endoscopic gastrostomy (PEG) tube placement for worsening dysphagia and airway compromise. This was followed by open partial laryngeal resection and tumor debulking on Day 15, which alleviated airway obstruction but left gross residual tumor due to the patient’s preference against definitive laryngopharyngectomy. Postoperatively, she developed bilateral pleural effusions, managed successfully with diuretics.
Postoperative Follow-Up and Efficacy of Intervention
Repeat CT imaging on Day 27 demonstrated a significant reduction in tumor size to 4.9 × 3.1 × 2.6 cm (Figure 2), correlating with marked clinical improvement. The patient reported resolution of dysphagia, regained her ability to speak clearly, and had no further episodes of positional airway compromise. By Day 35, she had transitioned to an oral diet without reliance on PEG tube feeds, tolerated tracheostomy decannulation, and was discharged home with home health support.
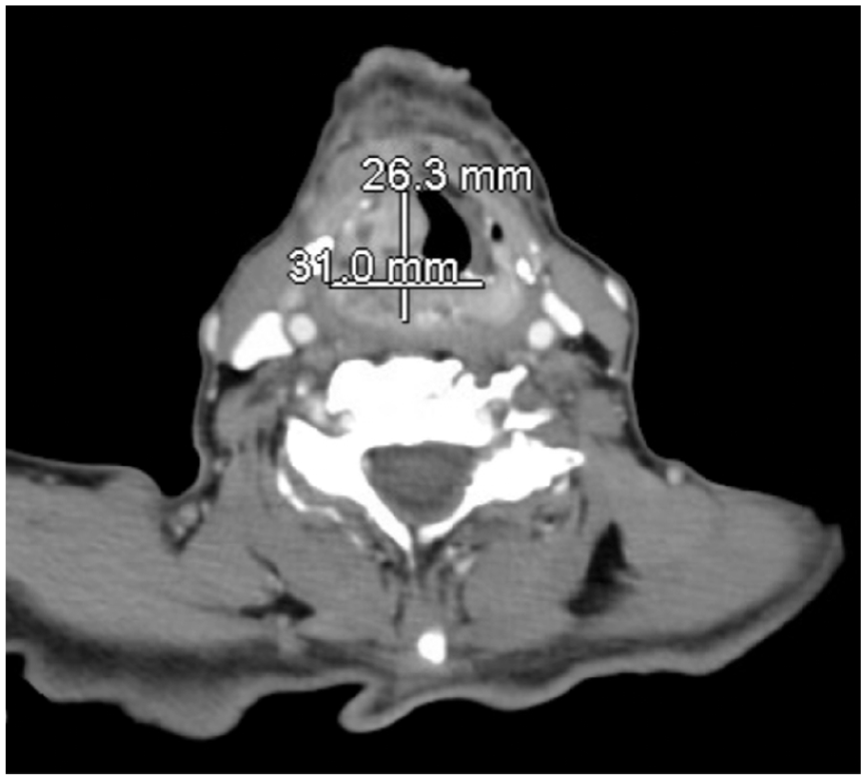
Significant reduction in tumor size to 4.9 × 3.1 × 2.6 cm (arrow) following partial laryngeal resection and debulking. Improved airway patency is evident, consistent with the patient’s postoperative clinical improvement in dysphagia and voice quality.
Repeat fiberoptic laryngoscopy at the 2nd month follow-up confirmed improved airway patency with residual tumor exhibiting stable margins and no evidence of regrowth. These findings not only validated the diagnostic accuracy of adult rhabdomyoma but also underscored the efficacy of debulking in alleviating mass effect and restoring function, consistent with prior reports of surgical management for large benign laryngeal tumors. 6
At follow-up, the patient declined further surgical intervention. Surveillance included plans for repeat fiberoptic laryngoscopy and optional imaging at the 6th month. Residual tumor persists but remains asymptomatic, necessitating ongoing clinical monitoring.
Discussion
This case exemplifies 3 critical aspects of adult rhabdomyoma that challenge conventional understanding: demographic rarity, unprecedented tumor size, and clinical urgency despite benign histology.
Demographic rarity: Adult rhabdomyoma is overwhelmingly a disease of middle-aged males, with only 20% of cases occurring in women. 3 Laryngeal involvement in elderly females is exceptionally rare, with fewer than 10 cases reported in patients over 70 years of age. 9 The reasons for this sex and age disparity remain unclear, although hormonal or genetic factors have been hypothesized. 4 This case adds to a limited body of literature documenting rhabdomyoma in elderly women, emphasizing the need to consider this entity even in atypical populations.
Unprecedented tumor size: The tumor’s dimensions (7.3 cm) exceed most-previously-reported rhabdomyomas. 6 Most adult rhabdomyomas measure 1 to 4 cm and are detected incidentally or during evaluation for mild symptoms. 6 The rapid progression of dysphagia and airway obstruction in this case suggests either delayed diagnosis due to the attribution of symptoms to aging or comorbid conditions (eg, fibromyalgia) or an unusual biologic behavior permitting accelerated growth. Notably, the tumor’s transglottic extension and near-total airway obstruction are features more commonly associated with malignancies, highlighting the diagnostic dilemma posed by large benign lesions. 7
Clinical urgency despite benignity: While adult rhabdomyoma is histologically benign, its mass effect can mimic aggressive malignancies both radiologically and clinically. 10 In this patient, the tumor caused life-threatening airway narrowing, necessitating an emergent tracheostomy—an intervention rarely required for smaller rhabdomyomas. This aligns with Ernst and Feller’s review of benign laryngeal tumors, which found that lesions exceeding 4 cm are significantly more likely to cause critical airway compromise. 11 The decision to pursue debulking rather than complete resection reflects the delicate balance between curative intent and functional preservation in elderly patients with comorbidities. 6
Diagnostic Challenges: The initial clinical and radiographic suspicion favored malignancy, given the tumor’s size, airway compromise, and transglottic spread. However, the absence of constitutional symptoms (eg, fever, night sweats) and the smooth mucosal surface on laryngoscopy raised suspicion for a benign entity. Histologic evaluation revealed classic features of rhabdomyoma, including polygonal cells with eosinophilic cytoplasm and “spider cells,” while immunohistochemistry (desmin+, S100−, pankeratin−) excluded mimics such as granular cell tumor and carcinoma. 8
Management Considerations: The patient’s refusal of definitive laryngopharyngectomy underscores the importance of individualized treatment plans in geriatric populations. While complete resection is curative, partial debulking may suffice for symptom relief in patients prioritizing quality of life over radical surgery. 6 Long-term surveillance is critical, as residual tumor carries a theoretical risk of recurrence, although malignant transformation has never been reported. 4
Conclusion
This report expands the clinical spectrum of adult rhabdomyoma, illustrating its potential for atypical presentation in elderly females and life-threatening obstruction despite benign histology. The case highlights the importance of early recognition in patients with prolonged upper aerodigestive symptoms and reinforces the need for multidisciplinary collaboration in managing large obstructive tumors. Future research should explore molecular mechanisms underlying tumor growth and sex-based disparities in incidence to refine diagnostic and therapeutic approaches.3,4
Footnotes
Acknowledgements
This research was supported by scholarly support from the University of Illinois College of Medicine. We would also like to acknowledge the guidance and mentorship of the Department of Internal Medicine, Department of Otolaryngology, and Department of General Surgery at the University of Illinois College of Medicine.
Ethical Considerations
Our institution does not require ethics approval for reporting individual cases or case series.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Since this is a case study/clinical case study write-up, no research funds were used. In the event of publication, the publication fee will be paid by the scholarly-activity funding belonging to Dr Sidney Stewart, MD, in her role as faculty within the Department of Medicine at UICOMP.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No datasets were generated or analyzed during the current study.