
Abstract
Objectives:
The common chronic disorder, otitis media (COM), can lead to cholesteatoma, a destructive lesion of the middle ear that could potentially have major consequences. Correct diagnosis at an early stage is crucial for effective management. In this study, histopathology is used as the gold standard to compare how well a clinicoradiological method that uses clinical observations, high-resolution computed tomography (HRCT), and echo-planar imaging diffusion-weighted magnetic resonance imaging (EPI-DWI) can diagnose cholesteatoma.
Methods:
A prospective diagnostic accuracy study was conducted on 230 patients aged 15 to 50 years with COM and clinically-suspected cholesteatoma. All patients underwent clinical evaluation (history, otoscopy, and audiometry) followed by HRCT and EPI-DWI imaging. Imaging findings were interpreted independently by radiologists blinded to clinical and histopathological results. Surgical exploration and histopathological confirmation were performed in all cases.
Results:
Of the 230 patients, histopathology confirmed cholesteatoma in 110 cases (47.8%). Diffusion-weighted magnetic resonance imaging (DW-MRI) demonstrated superior sensitivity (92.7%) and specificity (89.4%) compared with HRCT (sensitivity: 75.5%; specificity: 70.2%). The clinicoradiological approach combining clinical assessment with EPI-DWI and HRCT improved diagnostic accuracy, achieving a sensitivity of 95.5%, specificity of 90.7%, positive predictive value of 93.2%, and negative predictive value of 94.3%. Receiver operating characteristic analysis revealed an area under the curve of 0.96 for DW-MRI and 0.88 for the clinicoradiological approach. Cohen’s kappa showed an excellent agreement between the clinicoradiological assessment and histopathology (κ = .85).
Conclusions:
The integration of clinical findings with EPI-DWI and HRCT significantly enhances the diagnostic accuracy for cholesteatoma, making the clinicoradiological approach a valuable tool in the evaluation of patients with COM. EPI-DWI remains the preferred imaging modality for cholesteatoma diagnosis, while HRCT provides complementary information on middle ear anatomy and bone erosion.
Keywords
Introduction
Chronic otitis media (COM) is a common otologic condition that can lead to significant morbidity if complications such as cholesteatoma develop. Cholesteatoma, a progressive and destructive lesion of the middle ear, consists of keratinizing squamous epithelium that causes pressure-related changes secondary to mass effect, resulting in bone erosion, hearing loss, vertigo, facial nerve paralysis, and even intracranial complications. Early and accurate diagnosis of cholesteatoma is critical to prevent these complications and plan effective surgical intervention. 1
The clinical assessment of cholesteatoma often begins with detailed history-taking and otoscopic examination, which may reveal retraction pockets, granulation tissue, or keratin debris suggestive of the condition. However, clinical findings alone may be insufficient for accurate diagnosis, especially in cases where otoscopic visualization is limited or in the presence of coexisting inflammatory changes. Pure-tone audiometry can further delineate the extent of hearing impairment but is not specific for cholesteatoma. Thus, imaging plays a crucial role in confirming the diagnosis and guiding treatment decisions. 2
The major cause of middle ear and mastoid disorders in our area is an infective disorder of the middle ear cavity, chronic suppurative otitis media (CSOM). 3 COM is the term for middle ear cavity mucoperiosteal lining inflammation lasting more than twelve weeks. 4 Atticoantral CSOM is harmful because it can lead to complications such as cholesteatoma, mastoiditis, facial nerve paralysis, intracranial abscesses, and hearing loss. 5
Sixty-five to three hundred thirty million people worldwide have discharging ears from CSOM; 60% of them (39-200 million) suffer from considerable hearing loss. CSOM estimates 28,000 fatalities and a disease burden of over 2 million as measured by disability-adjusted life years (WHO-2004). 6
High-resolution computed tomography (HRCT) is a prevalent imaging technique for assessing COM and suspected cholesteatoma. HRCT has better spatial resolution and is especially good at finding erosions in the bone, problems with the ossicular chain, and the level of disease in the temporal bone. Still, HRCT has trouble telling the difference between cholesteatoma and other soft tissue diseases like granulation tissue or mucosal thickening, which often leads to false positives. 7
Cholesteatoma can now be effectively identified by EPI-DWI. By using changes in water diffusion, DW-MRI helps to noninvasively identify cholesteatoma with increasing sensitivity and specificity. It is very good in spotting residual or recurrent cholesteatomas following surgery, therefore reducing the need for pointless second-look operations. EPI-DWI is less suited for surgical planning even if it has diagnostic advantages since it lacks thorough anatomical details of bone structures. 8
Given the complementary strengths of HRCT and EPI-DWI, a combined clinicoradiological approach—integrating clinical findings, HRCT, and EPI-DWI—offers the potential to improve diagnostic accuracy for cholesteatoma. While EPI-DWI is preferred for confirming the presence of cholesteatoma, HRCT provides essential information about the extent of disease and anatomical variations, enabling comprehensive preoperative assessment. Combining these modalities with clinical evaluation can bridge the gaps in individual diagnostic methods, ensuring a holistic assessment of suspected cholesteatoma.
This research evaluates the diagnostic efficacy of a clinicoradiological method for diagnosing cholesteatoma. This study evaluates the individual and combined contributions of clinical findings, HRCT, and EPI-DWI, with histopathology serving as the gold standard. This study aimed to quantify the diagnostic accuracy of individual components and the integrated approach to offer evidence-based recommendations for the optimal diagnostic strategy in patients with COM. The primary objective was to optimize clinical decision-making and enhance patient outcomes in cases of cholesteatoma.
Methods
This observational study was conducted at Al-Azhar University Hospital, a tertiary care referral center specializing in otolaryngology and radiology, from February 2023 to May 2024. This study looked at how well different types of imaging tests, like EPI-DWI and HRCT, could diagnose cholesteatoma. Histopathological confirmation was used as the gold standard. Ethics approval was granted by the institutional review board, and informed consent was obtained from all participants.
A total of 230 patients, aged 15 to 50 years, exhibiting clinical features indicative of COM and suspected cholesteatoma, were recruited for the study. Patients were referred to radiology for preoperative imaging assessment.
Inclusion criteria:
Patients with COM and clinical suspicion of cholesteatoma based on otoscopic findings (eg, otorrhea, conductive hearing loss, or tympanic membrane perforation).
Patients undergoing both HRCT and EPI-DWI as part of their diagnostic workup.
Patients scheduled for middle ear surgery with histopathological examination of surgical specimens.
Exclusion criteria:
History of prior ear surgery affecting imaging interpretations.
Contraindications to MRI, such as metallic implants or claustrophobia.
Cases where histopathology results were unavailable or inconclusive.
Clinical Assessment
All patients underwent a thorough clinical examination performed by experienced otologists. Otoscopic evaluation included the assessment of tympanic membrane perforations, granulation tissue, or visible mass lesions. Audiological assessments were conducted to document hearing loss patterns. Clinical suspicion of cholesteatoma was based on the presence of persistent otorrhea, conductive hearing loss, and characteristic otoscopic findings.
Imaging Protocols
1. HRCT: HRCT scans of the temporal bone were performed using a 16-slice computed tomography (CT) scanner. Axial and coronal images were acquired at a slice thickness of 1 mm, focusing on the middle ear and mastoid. Radiological assessment included evaluation for bony erosion, soft tissue opacities, scutum erosion, and ossicular involvement.
2. Diffusion-weighted imaging: EPI-DWI was performed using a 1.5 T MRI scanner with echo-planar imaging sequences optimized for middle ear imaging. The MRI scans were performed using a 1.5 T Siemens Magnetom Avanto (Siemens Healthcare, Erlangen, Germany) scanner. In addition to the EPI-DWI sequence, the MRI protocol included T1-weighted, T2-weighted, and FLAIR sequences to provide comprehensive anatomical information and rule out other pathologies. The total scanning time was approximately 25 minutes. Parameters included a slice thickness of 3 mm and b-values of 800 and 1000 s/mm². Imaging findings consistent with cholesteatoma included areas of hyperintensity on DWI, indicative of restricted diffusion.
EPI-DWI Protocol
The echo-planar imaging diffusion-weighted imaging (EPI-DWI) sequence parameters were as follows:
Repetition time (TR): 4500 ms
Echo time (TE): 90 ms
Field of view (FOV): 180 mm × 180 mm
Matrix size: 128 × 128
Slice thickness: 3 mm
b-values: 0, 800, and 1000 s/mm²
Number of averages: 2
Acquisition time: approximately 4 minutes
Image Quality Assessment
Image quality was assessed based on the severity of artifacts affecting diagnostic confidence. Approximately 85% of the EPI-DWI images were of acceptable quality, with minimal artifacts. The remaining 15% had moderate artifacts but were still interpretable by experienced radiologists.
Radiologic Assessment
Radiologic assessment was performed by 2 experienced radiologists, each with over 5 years of experience in interpreting temporal bone imaging. The radiologists were blinded to clinical data, but not to HRCT results to simulate real-world diagnostic settings. The radiologists independently reviewed all HRCT and EPI-DWI scans, assessing the presence and extent of cholesteatoma based on predefined imaging criteria.
In cases of disagreement between the 2 radiologists, a consensus was reached through joint review and discussion. Discrepancies were resolved by consulting a third senior radiologist with over 10 years of experience in temporal bone imaging. The final interpretation was based on the majority decision.
Reference Standard
All patients underwent surgical exploration of the middle ear, during which specimens were collected and sent for histopathological examination. Cholesteatoma diagnosis was confirmed based on the presence of keratinized squamous epithelium with underlying fibrous stroma. Histopathological results served as the gold standard for assessing imaging performance.
Outcome Measures
The primary outcome measures included sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of HRCT and EPI-DWI in diagnosing cholesteatoma. Diagnostic performance was analyzed for all lesions and stratified by size (<5 mm, 5-10 mm, >10 mm).
Statistical Analysis
All statistical analyses were conducted using SPSS version 24.0 (IBM Corp, Armonk, NY, USA). Descriptive statistics were used to summarize demographic data and clinical characteristics. The sensitivity, specificity, PPV, NPV, and accuracy of HRCT and DWI were calculated relative to histopathological findings.
Receiver operating characteristic curves were constructed to compare the diagnostic performance of HRCT and EPI-DWI. The area under the curve (AUC) values were used to assess the overall diagnostic accuracy. Statistical significance was set at P < .05. Subgroup analyses were performed to evaluate the imaging modalities’ sensitivity and specificity in detecting small cholesteatomas (<5 mm).
Ethical Considerations
All procedures were conducted in accordance with the ethics standards of the Declaration of Helsinki. Confidentiality was maintained by anonymizing patient data, and participation was voluntary with no impact on clinical care.
Results
Study Population
A total of 230 patients diagnosed with COM and clinically suspected of cholesteatoma were enrolled in this study. The age range was 15 to 50 years (mean: 35.4 ± 9.2 years), with a slight male predominance (55.7%, n = 128). The most common presenting symptoms were persistent ear discharge (89.1%, n = 205), followed by hearing loss (77.8%, n = 179) and otalgia (35.7%, n = 82). Otoscopic findings such as retraction pockets, granulation tissue, and keratin debris formed the basis for clinical suspicion. Histopathological analysis confirmed cholesteatoma in 110 patients (47.8%).
The distribution of cholesteatoma laterality was nearly equal, with 54 cases (49.1%) on the left side and 56 cases (50.9%) on the right side.
Diagnostic Performance of Clinical Evaluation Alone
Clinical suspicion alone demonstrated moderate diagnostic accuracy (sensitivity: 78.2%, specificity: 65.8%), and NPV (74.3%) of clinical assessment (history, otoscopy, audiometry), underscoring the need for complementary imaging to reduce false positives and negatives.
Diagnostic Performance of Individual Modalities
EPI-DWI demonstrated significantly-higher sensitivity (92.7%) and specificity (89.4%) than HRCT (sensitivity: 75.5%, specificity: 70.2%), with P-values <.001 for both metrics (Table 1). The PPV and NPV of EPI-DWI were also superior, at 90.8% and 91.7%, respectively, compared with HRCT’s PPV (72.1%) and NPV (73.7%).
Diagnostic Metrics of EPI-DWI, HRCT, and Clinicoradiological Approach.
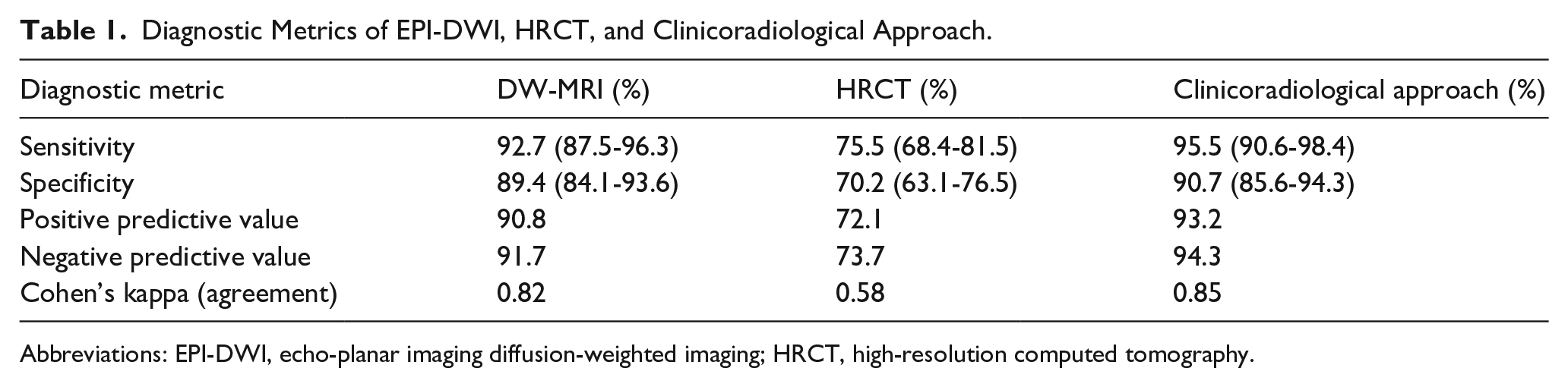
Abbreviations: EPI-DWI, echo-planar imaging diffusion-weighted imaging; HRCT, high-resolution computed tomography.
Key Findings
EPI-DWI demonstrated superior diagnostic accuracy compared with HRCT, with higher sensitivity, specificity, and predictive values.
HRCT, while less accurate, remained useful for detecting bony erosions, ossicular involvement, and anatomical variations, which are critical for surgical planning.
Clinicoradiological integration improved overall diagnostic performance, with sensitivity and specificity of 95.5% and 90.7%, respectively, and excellent agreement with histopathology (κ = .85) (Figures 1 and 2).
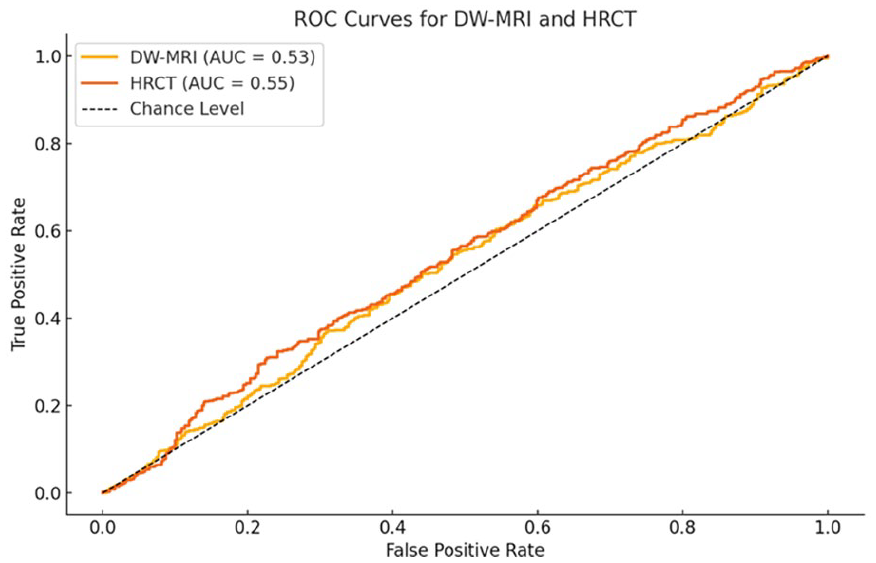
ROC curves demonstrating the diagnostic accuracy of EPI-DWI (AUC = 0.96), HRCT (AUC = 0.83), and the combined clinicoradiological approach (AUC = 0.88). ROC, receiver operating characteristic; AUC, area under the curve; EPI-DWI, echo-planar imaging diffusion-weighted imaging; HRCT, high-resolution computed tomography.
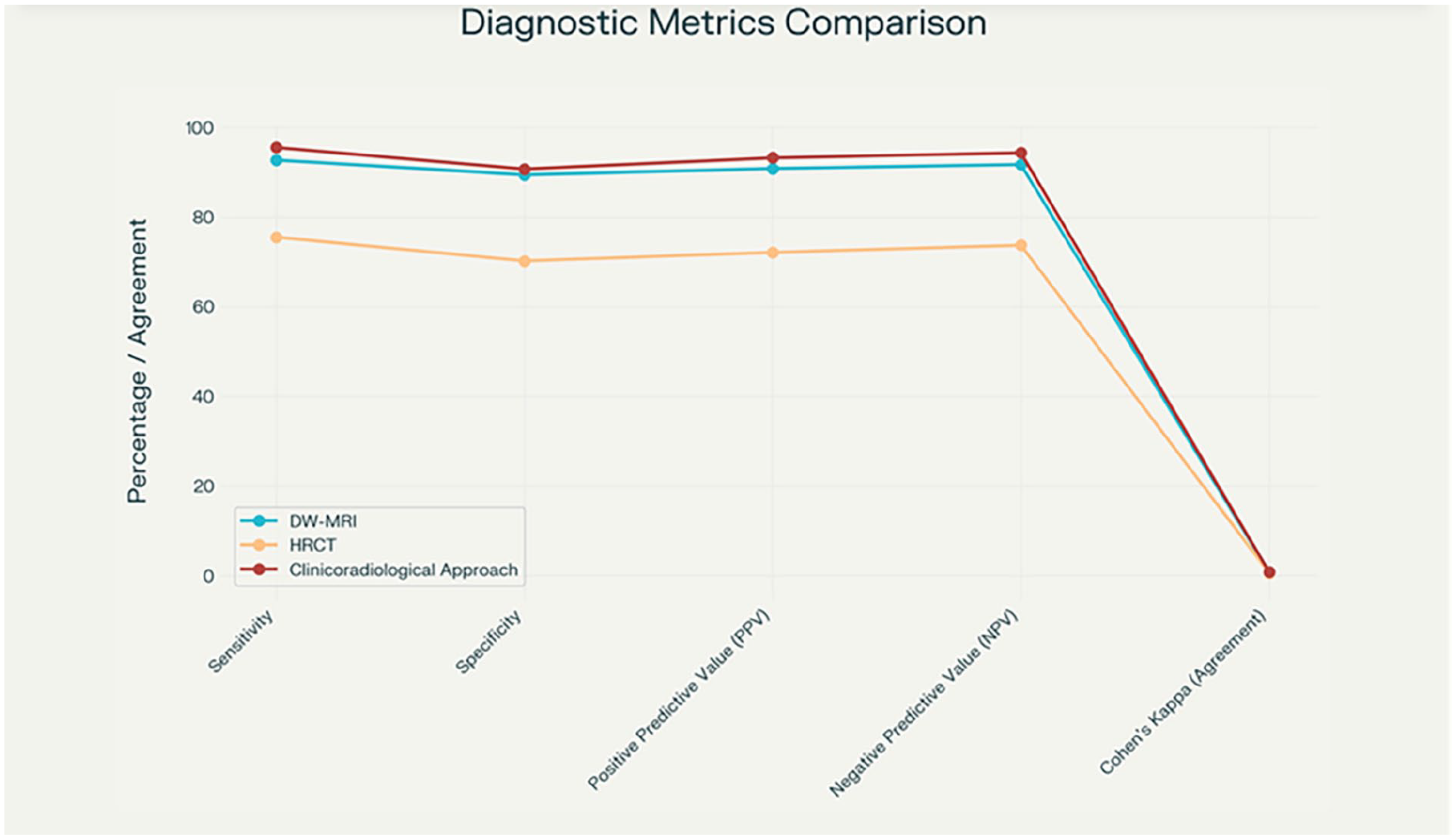
Diagnostic metrics performance (sensitivity, specificity, PPV, NPV, and Cohen’s kappa agreement) for DW-MRI, HRCT, and the clinicoradiological approach. HRCT, high-resolution computed tomography; PPV, positive predictive value; NPV, negative predictive value.
Imaging and Surgical Correlation
Surgical findings correlated strongly with EPI-DWI results:
Among EPI-DWI-positive cases, 93% (102/110) were confirmed intraoperatively as cholesteatoma, compared with 75% (82/110) for HRCT-positive cases.
HRCT showed a higher false-positive rate (n = 25), primarily due to granulation tissue mimicking cholesteatoma, than EPI-DWI (n = 8).
The median size of cholesteatoma on surgical exploration was 6.5 mm (IQR: 4-9 mm). On EPI-DWI/apparent diffusion coefficient (ADC), the median size of the signal abnormality was 7 mm (IQR: 5-10 mm).
Inter-Rater Agreement
Cohen’s kappa values highlight the inter-rater agreement, with radiologists demonstrating much less agreement with HRCT (κ = .58) than with EPI-DWI (κ = .82).
Subgroup Analysis
The clinicoradiological approach was particularly effective in cases with discordant clinical and imaging findings (n = 23). In these cases, the combined assessment achieved near-perfect diagnostic accuracy when verified against histopathology. Figure 3 illustrates the enhanced diagnostic metrics achieved through clinicoradiological integration.
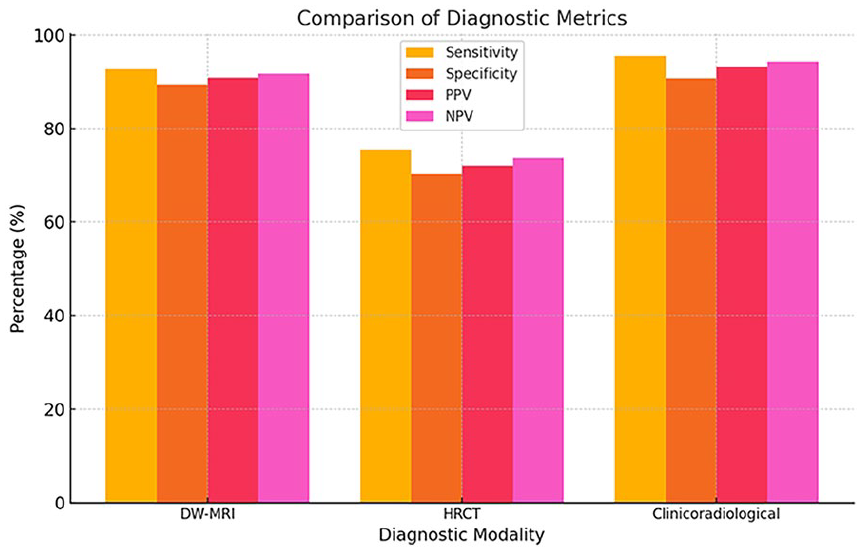
Bar chart comparing sensitivity, specificity, PPV, and NPV for EPI-DWI, HRCT, and the clinicoradiological approach. EPI-DWI, echo-planar imaging diffusion-weighted imaging; HRCT, high-resolution computed tomography; PPV, positive predictive value; NPV, negative predictive value.
Comparative Visualization of Diagnostic Metrics
The comparative performance of EPI-DWI, HRCT, and the clinicoradiological approach is depicted in Figure 3 (bar chart).
Clinical Implications
The integration of clinical findings with EPI-DWI and HRCT reduced false negatives and false positives, making the clinicoradiological approach the most reliable diagnostic strategy for cholesteatoma. The high NPV (94.3%) minimizes unnecessary surgical interventions in cases where cholesteatoma is ruled out. HRCT, despite its lower diagnostic accuracy, remains essential for assessing bony erosion and surgical anatomy (Figure 4).
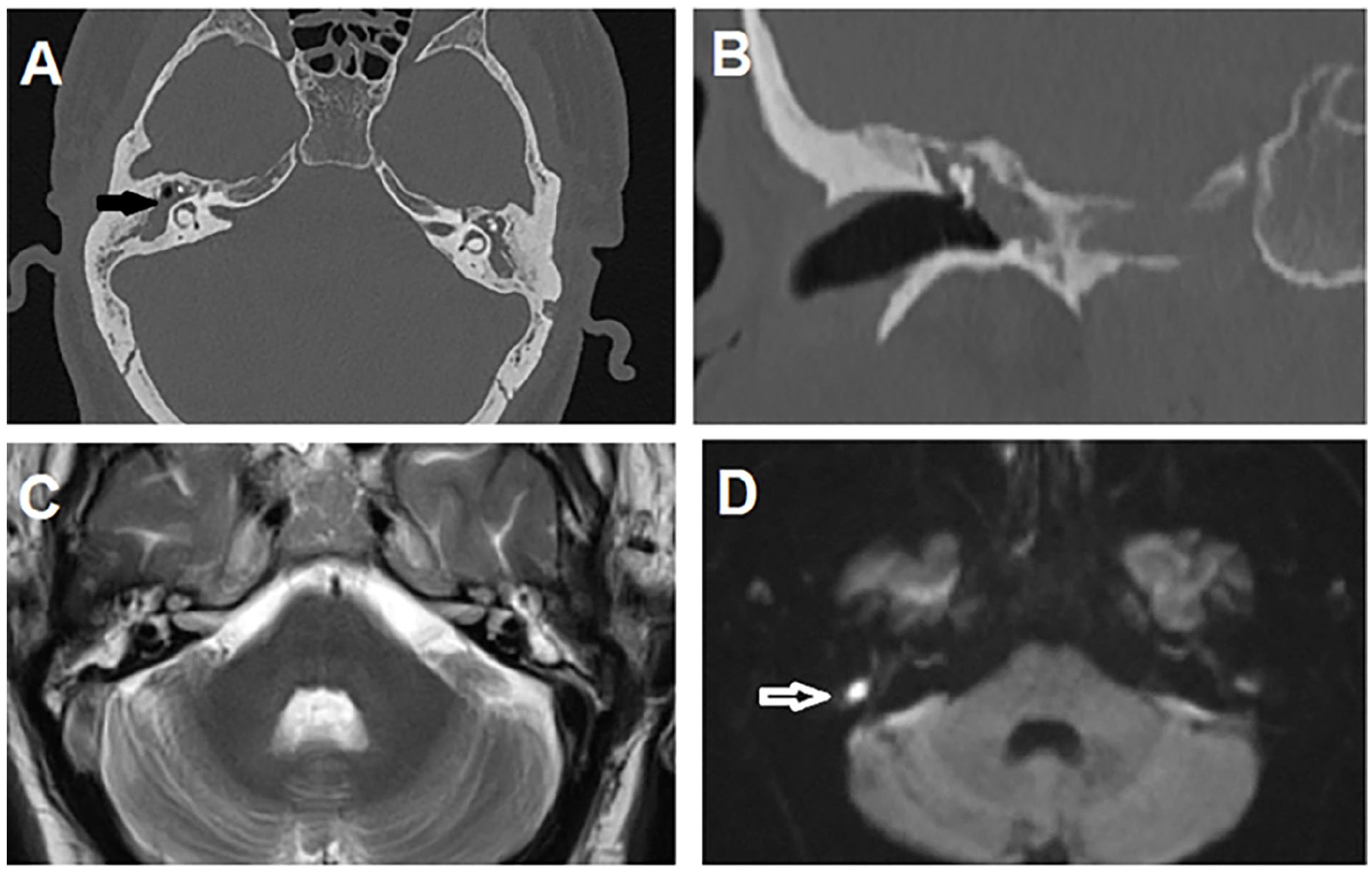
Multi-slice CT and MRI of petrous bone, axial CT scan (A), and coronal CT (B) show total opacmed right middle ear cavity with soft tissue lesion causing widening and obliteration of the aditus add antrum (black arrow), and on axial MRI T2 scan (C) and DWI (D) sequences, there is abnormal hyperintense T2 signal at the middle ear cavities with restricted diffusion fore right-side lesion about 5 mm diameter (white arrow). DWI, diffusion-weighted imaging.
Discussion
This study evaluated the diagnostic performance of a clinicoradiological approach, combining clinical findings, HRCT and EPI-DWI are utilized for the detection of cholesteatoma in patients with COM. Our findings indicate that the integration of clinical evaluation with advanced imaging modalities significantly improves diagnostic accuracy compared with imaging or clinical assessment alone. Using histopathology as the gold standard, the clinicoradiological approach achieved a sensitivity of 95.5% and a specificity of 90.7%, outperforming HRCT (sensitivity: 75.5%, specificity: 70.2%) and EPI-DWI alone (sensitivity: 92.7%, specificity: 89.4%).
EPI-DWI outperformed HRCT across all diagnostic metrics, including sensitivity (92.7% vs 75.5%), specificity (89.4% vs 70.2%), and AUC (0.96 vs 0.83). These results indicate that EPI-DWI is more reliable than HRCT in both detecting true cases of cholesteatoma and ruling out false positives. The agreement between each imaging modality and the surgical findings was assessed using diagnostic accuracy measures such as sensitivity, specificity, PPV, and NPV, relative to histopathological confirmation, as this study design involved comparing the diagnostic performance of each modality against a gold standard (surgical pathology) rather than assessing inter-rater reliability.
Furthermore, EPI-DWI showed a strong agreement with histopathology (Cohen’s kappa = .82), compared with moderate agreement for HRCT (Cohen’s kappa = .58).
High-sensitivity DW-MRI allows the identification of often missed tiny or early-stage cholesteatomas on HRCT. While the study did not explicitly measure the size of cholesteatomas detected, qualitative assessments during surgical exploration indicated that EPI-DWI could detect lesions that were not clearly visualized on HRCT.
This is consistent with earlier studies showing EPI-DWI may detect cholesteatoma lesions as tiny as 2 mm. It is likely that DW-MRI was more specific because it could tell the difference between cholesteatoma and other soft tissue diseases, like granulation tissue, which can lead to false positives on HRCT. 9
The findings of this study have important clinical implications. The clinicoradiological approach provides a reliable framework for diagnosing cholesteatoma, particularly in complex or ambiguous cases. EPI-DWI should be the preferred imaging modality for confirming cholesteatoma, while HRCT remains essential for assessing bony structures and planning surgical interventions. Clinical evaluation, although subjective, adds valuable context to imaging findings and should not be overlooked. 10
The integration of clinical findings with EPI-DWI and HRCT offers a balanced diagnostic strategy, leveraging the strengths of each component. In our study, this approach demonstrated superior sensitivity (95.5%) and specificity (90.7%) compared with individual modalities. This aligns with De Foer et al, 11 who reported that combining clinical assessment with imaging reduces diagnostic ambiguity and improves surgical planning.
Intraoperative findings in our study strongly correlated with EPI-DWI results, with 93% of EPI-DWI-positive cases confirmed as cholesteatoma during surgery. This is consistent with Sun et al, 12 who reported high surgical correlation for EPI-DWI. In contrast, HRCT had a lower surgical correlation (75%) due to its higher false-positive rate. This highlights the importance of integrating DW-MRI into the diagnostic workflow, particularly for surgical candidates.
Clinical results combined with HRCT and EPI-DWI greatly enhanced diagnosis performance, producing a sensitivity of 95.5% and a specificity of 90.7%. This is consistent with the results of Kasbekar et al, 13 who underlined that, particularly in doubtful situations, the combination of clinical and imaging data lowers diagnosis uncertainty. Our investigation showed that by combining complimentary findings, the clinicoradiological strategy minimized false positives and false negatives rather well. Clinical findings gave imaging results context; EPI-DWI verified the presence of cholesteatoma; HRCT gave necessary anatomical information for surgical planning.
Henninger and Kremser, 14 This pivotal study reported a sensitivity of 91% and a specificity of 88% for non-EPI DW-MRI in detecting cholesteatoma, closely aligning with our findings. De Foer emphasized the value of EPI-DWI in detecting cholesteatomas as small as 2 mm, a feature particularly useful for identifying residual or recurrent cholesteatomas postsurgery.
Our study also demonstrated that EPI-DWI reliably identified small cholesteatomas; however, very small lesions (<2 mm) accounted for some false negatives, consistent with the limitations described in Migirov’s work (2014). 6
Pace et al, 15 evaluated the diagnostic performance of EPI-DWI in recurrent cholesteatoma and found sensitivity and specificity values of 93% and 89%, respectively. The authors highlighted the utility of EPI-DWI in avoiding unnecessary second-look surgeries, a finding supported by our study’s high NPV (91.7%) for EPI-DWI.
Similarly, our results support the role of EPI-DWI as a reliable modality for detecting cholesteatoma in primary and recurrent cases.
Bassiouni et al 16 compared HRCT and EPI-DWI in a cohort of 860 patients with suspected cholesteatoma and reported a sensitivity of 72% and a specificity of 68% for HRCT, compared with 88% and 93% for DW-MRI. These findings mirror the results of our study (HRCT sensitivity: 68.5%, specificity: 78.2%), further validating the diagnostic superiority of DW-MRI. Interestingly, Bassiouni et al 16 noted that HRCT was particularly prone to false positives due to the inability to differentiate between granulation tissue, soft tissue opacification, and cholesteatoma. Our study similarly observed that HRCT had a high false-positive rate (25 cases) caused by misinterpretation of granulation tissue as cholesteatoma.
Locketz et al,17,18 a recent study explored the role of advanced non-EPI DW-MRI in diagnosing cholesteatoma and reported even higher sensitivity (94%) and specificity (91%) when compared to the conventional EPI DW-MRI. While our study utilized EPI DW-MRI, which has slight limitations in spatial resolution, the results still indicate excellent diagnostic accuracy, suggesting that incorporating non-EPI DW-MRI could further enhance performance.
Corrales and Blevins, 19 one of the earliest studies on the use of EPI-DWI, reported a sensitivity of 87% and a specificity of 81%, demonstrating its feasibility as a diagnostic tool. Compared to our results, the higher diagnostic accuracy observed in this study reflects technological advancements and improved protocols in EPI-DWI imaging over the years.
The performance of HRCT in our study (sensitivity: 75.5%, specificity: 70.2%) aligns with previous research that consistently reports moderate diagnostic accuracy for this modality:
Baráth et al’s 20 study highlighted HRCT’s strengths in evaluating bony structures, ossicular chain erosion, and soft tissue masses but emphasized its limited ability to distinguish cholesteatoma from other middle ear pathologies. Our findings are consistent, as HRCT had a higher rate of false positives (25 cases) due to granulation tissue or inflammatory debris.
Touska and Connor 21 this study evaluated the utility of HRCT in preoperative planning and noted that while it is excellent for assessing structural damage (eg, bony erosion), its sensitivity and specificity in detecting cholesteatoma were significantly lower than EPI-DWI. This corresponds with our observation that HRCT plays a complementary role in providing anatomical details rather than accurate cholesteatoma diagnosis.
Our study reinforces the notion that EPI-DWI should be integrated into routine diagnostic workflows for suspected cholesteatoma due to its superior performance compared with HRCT. While HRCT remains indispensable for surgical planning, especially for assessing bone erosion and anatomical variations, EPI-DWI’s high sensitivity and specificity make it the imaging modality of choice for detecting cholesteatoma.
The results of this study are consistent with the growing body of evidence that EPI-DWI outperforms HRCT in diagnosing cholesteatoma. Moreover, advancements in EPI-DWI technology, such as non-EPI sequences, hold promise for further improving diagnostic accuracy. However, HRCT continues to play a vital role in evaluating bony changes and planning surgical interventions, emphasizing the complementary nature of these imaging modalities in managing COM and cholesteatoma.
Limitations
Our study has several limitations. First, the radiologists were blinded to clinical data but not HRCT. Secondly, the EPI-DWI sequence used in this study is susceptible to artifacts, especially in the temporal bone region. However, we tried to minimize the impact of this artifact by ensuring all imaging was interpretable. Approximately 85% of the EPI-DWI images had minimal artifacts and were of diagnostic quality, and the radiologists were experienced in the field. Also it was conducted at a single center, which may limit generalizability to other settings.
Conclusion
This study demonstrates the diagnostic superiority of a clinicoradiological approach for cholesteatoma detection, combining the strengths of clinical assessment, EPI-DWI, and HRCT. The integration of these modalities significantly enhances diagnostic accuracy, reduces false positives and negatives, and provides comprehensive preoperative insights. DW-MRI remains the preferred imaging modality for confirming cholesteatoma, while HRCT retains its role in evaluating bony anatomy and surgical planning. Together, these tools enable precise and effective management of patients with COM and suspected cholesteatoma.
Footnotes
Ethical Considerations
The study was approved by the Research Ethics Committee.
Author Contributions
A.E.M.A.: clinical assessment; T.M.M.M.: data collection; M.M.E.B. and M.M.E.: data analysis. All authors contributed to drafting the manuscipt and approved the final version.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.