
Abstract

Significance Statement
Primary cutaneous follicle center lymphoma (PCFCL) can masquerade as systemic lymphoma with skin involvement. Careful hematopathology evaluation differentiates PCFCL from other cutaneous lymphomas: positive for B-cell markers (CD19, CD20, and CD79a) and follicle center markers (CD10 and BCL-6), while negative or weakly positive for BCL-2 without t(14;18) translocation. It commonly occurs in the head and neck region and is radiotherapy sensitive with an excellent prognosis. Accurate diagnosis is critical to avoid potential invasive surgery or systemic chemotherapy.
An 82-year-old male presented with an enlarging left preauricular firm and violaceous mass. He has embedded metal fragments from a prior blast injury in the same region as the new lesion. His past medical history was notable for hypertension, coronary artery disease, diabetes, and hyperlipidemia. He had no personal or family history of malignancy. A maxillofacial computed tomography (CT) with contrast and fine-needle aspriation biopsy (FNA) was obtained during the initial consultation.
CT scans demonstrated a 2.7 × 2.2 cm hyperdense lesion in the left cheek superficial to the masseter muscle with thickened skin and retained ballistic fragments (Figure 1A). Initial FNA showed a small lymphoid population but was non-diagnostic. Given rapid growth, concern of lymphoma, and to evaluate for distant disease, a PET/CT was obtained and showed an FDG avid left cheek lesion with interval growth to 5.0 × 3.4 cm over 2 months (Figure 1B). Concurrently, core biopsy revealed a mixed follicular and diffuse lymphocytic infiltration with immunohistochemical stains positive for CD20, BCL-6, CD23, and negative for CD10, CD30, MUM-1, c-MYC, CD43, and cyclin D1; BCL-2 was noted to be weakly positive (Figure 2). Flow cytometry did not identify immunophenotypic evidence of B-cell or T-cell non-Hodgkin lymphoma, though the sample was noted to be pauci-cellular. Immunoglobulin gene rearrangement testing revealed a monoclonal population of B lymphocytes, while T-cell receptor gamma rearrangement demonstrated polyclonal T lymphocytes. Fluorescence in situ hybridization studies did not demonstrate canonical B-cell lymphoma translocation t(14;18). Given the hematopathology findings of monoclonal B-cell lymphocytes in a follicle pattern in combination with the overall clinical picture and lack of systemic disease, he was diagnosed with PCFCL. Primary radiation was recommended after review by a multidisciplinary tumor board. The patient exhibited an excellent response to treatment and has no evidence of disease on surveillance visits to date.
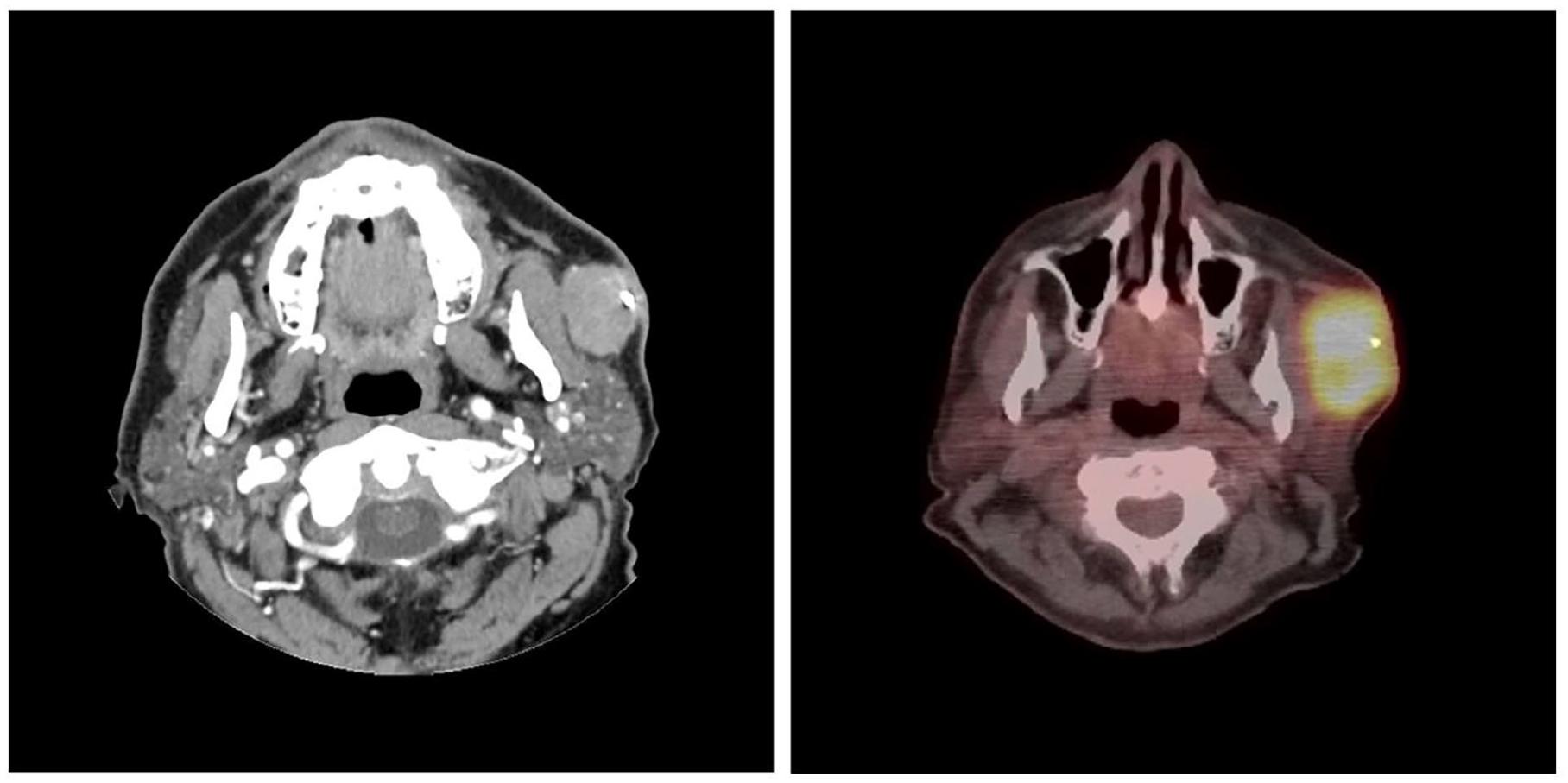
(A) CT maxillofacial with contrast shows a hyperdense lesion of the left cheek, superficial to the left masseter muscle and parotid gland, and retained ballistic fragments. (B) PET/CT shows intense FDG uptake in the known left cheek/preauricular mass with interval growth. CT, computed tomography.
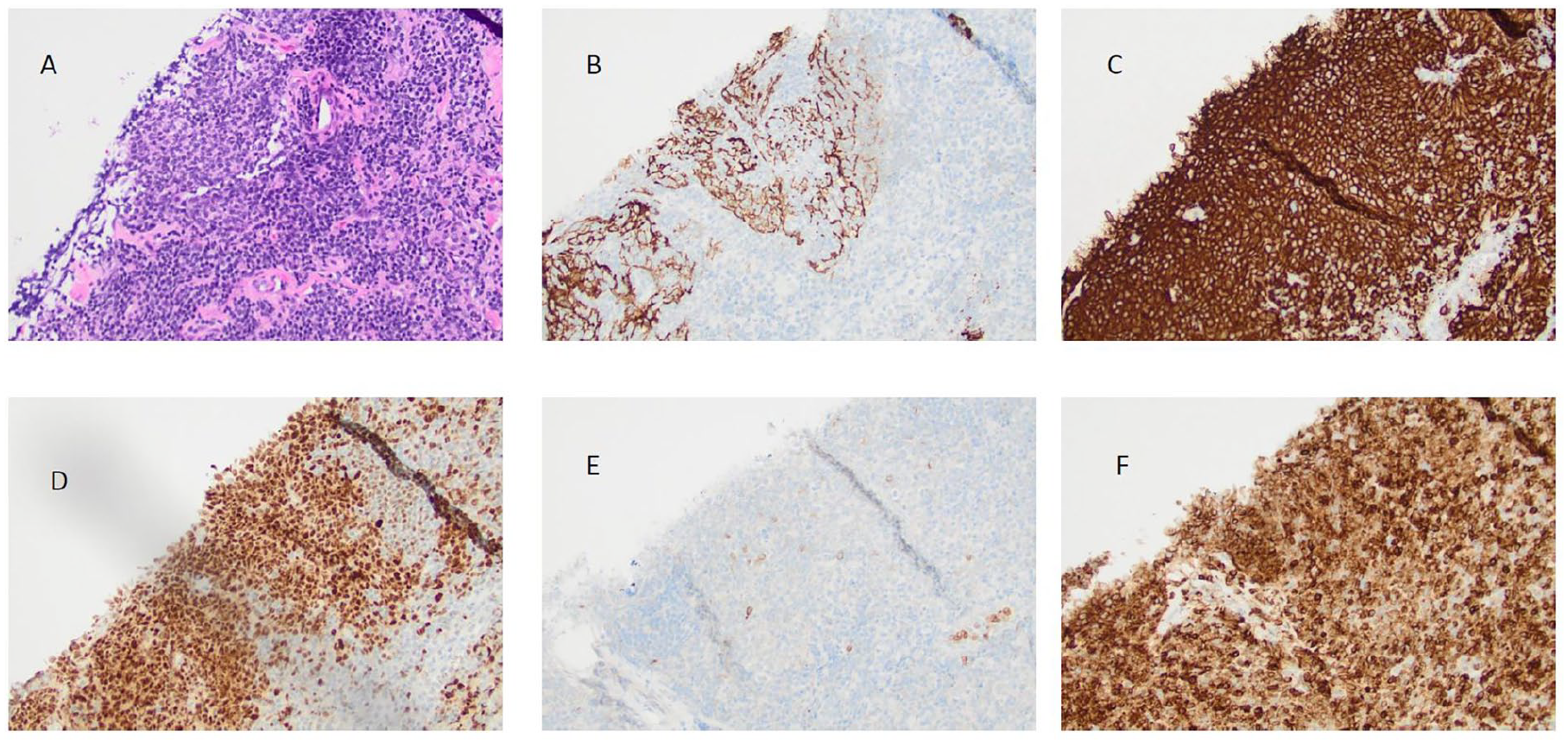
(A) Section shows a neoplastic follicle composed of centrocytes admixed with centroblasts (H&E, ×20). (B) The neoplastic follicle contains a dendritic cell mesh that works, as confirmed by IHC (CD21, ×20). Follicular cells are positive for CD20 (C), BCL-6 (D), BCL-2 (F), and negative for CD10 (E) as demonstrated by IHC (CD20, BCL-6, BCL-2, and CD10, ×20). H&E, hematoxylin; IHC, immunohistochemistry.
Though most cutaneous head and neck malignancies represent squamous cell carcinoma, basal cell carcinoma, and melanoma, cutaneous lymphoma must be on the differential when diagnosis is not immediately apparent. While overall rare, PCFCL is the most common primary cutaneous subtype of B-cell lymphoma, and, more importantly, typically presents as a papule or nodule on the head, neck, or trunk.1,2 It is a low-grade lymphoma of follicle center B cells with an exclusively cutaneous primary lesion without any systemic or nodal involvement. 2 Clinical presentation can mimic traditional cutaneous malignancies or parotid tumors depending on location, yet differentiating this entity from other primary cutaneous malignancies or systemic lymphoma with cutaneous involvement is crucial, given the differences in biology, prognosis, and management. Given the propensity for the head and neck region, otolaryngologists play a critical role in the workup and management of this entity. While traditional lymphoma is often in mind when working up an enlarging lymph node in the head and neck, primary cutaneous lymphoma must also be in the differential for cutaneous lesions.
PCFCL can be distinguished from other lymphoma subtypes through careful examination, systemic imaging, and in-depth pathological evaluation. The neoplastic cells stain positively for B-cell markers CD19, CD20, CD79a, and typically follicle center markers CD10 and BCL-6, though CD10 may be variably positive in follicular patterns and negative in diffuse pattern subtypes. It is negative or weak for BCL-2, but lacks the t(14;18) rearrangement.3-5
PCFCL is radiotherapy sensitive with a 99% complete response rate, 3 which is especially important given the potential functional or cosmetic impact resulting from tumor extirpation. Surgical resection is an acceptable alternative but suffers from a relatively high rate of recurrence. 4 Following treatment, outcomes remain excellent with 5-year survival exceeding 95%, though ongoing surveillance is required to monitor for recurrence.
As PCFCL masquerades as other benign and malignant tumors of the head and neck, precision diagnosis is essential and has a direct impact on treatment and outcomes. While traditional primary cutaneous malignancies are treated with surgery as a first-line option, PCFCL may be treated definitively with radiation. In this case, if surgery were entertained, it would have likely entailed distal facial nerve sacrifice and the need for reconstructive surgery for the defect created, whereas the diagnosis of PCFCL allowed for a primary radiation approach, sparing the potential disfigurement from surgery while retaining excellent oncologic outcomes.
This study was deemed IRB exempt by the Veterans Health Administration Office of Research and Development (VA ORD). A waiver for consent was obtained from the VA ORD as per institutional protocol for individual patient reports and series. All patient identifiers were removed, and data were anonymized with no unique identifying protected health information included.
Footnotes
Ethical Considerations
This study was deemed exempt by the Institutional Review Board.
Author Contributions
P.Z.: writing—original draft. Z.M.D.: writing—review and editing. Z.H.R.: writing—review and editing, supervision.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.