
Abstract
Isolated unilateral temporalis muscle hypertrophy (IUTMH) is a rare clinical entity, with fewer than 20 cases reported globally. This case report and literature review aimed to expand the understanding of its diagnosis, management, and outcomes. A 44-year-old Arab Asian woman presented with a 12 month history of progressive left temporal swelling and pain during mastication. Clinical examination revealed a firm, non-tender mass. Imaging [computed tomography (CT) and ultrasonography] confirmed isolated left temporalis muscle hypertrophy without neoplastic or inflammatory features. Botulinum toxin type A (Btx A, 25 U) injection led to symptom improvement and partial muscle reduction at 3 month follow-up. A literature review of 16 published cases (including ours) demonstrated a slight female predominance (10/16), variable symptom profiles (painless swelling to masticatory dysfunction), and diverse management strategies. Minimally-invasive Btx A achieved favorable outcomes in 6/16 cases, with lower doses (25 U) showing efficacy comparable with higher doses. Surgical intervention, although effective, was associated with recurrence in 1 case. Diagnostic reliance on imaging (CT/magnetic resonance imaging) and histology (when performed) confirmed hypertrophy without malignancy. While bruxism and stress were implicated in some cases, 7/16 lacked identifiable triggers, suggesting multifactorial etiology. Long-term follow-up data remain limited, underscoring the need for vigilant monitoring. This case reinforces Btx A as a primary therapeutic option and highlights the importance of individualized management in IUTMH. Further research is warranted to elucidate pathogenesis and optimize treatment protocols.
Keywords
Introduction
Isolated unilateral temporalis muscle hypertrophy (IUTMH) is a rare clinical condition characterized by the unilateral enlargement of the temporalis muscle without concurrent involvement of other masticatory muscles. Initially reported by Wilson and Brown in 1990, this entity has since been documented in only a limited number of cases, highlighting its exceptional rarity. 1 With fewer than 20 cases reported in the literature over the past 3 decades, IUTMH stands out as an uncommon cause of temporal swelling that warrants careful diagnostic consideration. 2 The condition typically manifests as a localized swelling in the temporal region, which may be painless or associated with discomfort, and occasionally presents with headaches or masticatory difficulties. 3 The etiology of IUTMH remains poorly understood, with proposed mechanisms including compensatory hypertrophy, stress-induced changes, and parafunctional habits such as bruxism.2,3 While bruxism has been identified as a potential contributing factor in several cases, including those with dental wear or a history of stress, the precise cause often remains elusive. 4 This ambiguity underscores the importance of a thorough diagnostic approach, typically involving imaging modalities such as computed tomography (CT) and magnetic resonance imaging (MRI) to confirm muscle enlargement and exclude alternative pathologies like neoplasms or inflammatory processes. 5 In some instances, muscle biopsy is employed to verify the diagnosis, revealing normal muscle architecture or hypertrophic changes without evidence of underlying disease. 2 Management of IUTMH varies widely, ranging from conservative strategies—such as observation or symptomatic relief with analgesics—to more invasive interventions like botulinum toxin (Btx) injections or surgical reduction, tailored to the patient’s symptoms and preferences.2,3 Given the scarcity of IUTMH, each reported case provides valuable insights into its clinical spectrum and therapeutic options.
This case report presents a detailed account of a woman with IUTMH, complemented by a comprehensive literature review, aiming to enhance the understanding of this rare condition and inform future clinical decision-making.
Case Presentation
A 44-year-old woman presented to the otorhinolaryngology department with a 1 year history of progressive left temporal swelling accompanied by localized pressure and discomfort. The swelling initially arose without associated numbness, pruritus, purulent discharge, or inflammatory signs. However, recent exacerbation of pain during mastication and bruxism correlated with noticeable enlargement of the lesion. The patient denied relevant medical, surgical, familial, or traumatic history, with no identifiable triggers for her symptoms. Clinical examination revealed a firm, non-fluctuant, and non-tender mass in the left temporal region, measuring ~3 cm in diameter. The overlying skin exhibited no erythema, warmth, or textural changes (Figure 1). Contrast-enhanced CT demonstrated marked thickening of the anterior left temporalis muscle (2.1 × 2.8 × 3.9 cm), characterized by ill-defined margins and homogeneous attenuation. No fluid collections, abnormal contrast enhancement, or lymphadenopathy were observed (Figure 2). Subsequent ultrasonography corroborated these findings, revealing muscular hypertrophy with preserved architecture and homogeneous echotexture. A diagnosis of temporalis muscle hypertrophy was established based on the concordance between clinical history, physical examination, and imaging features. Differential diagnoses, including neoplastic or inflammatory processes, were deemed unlikely due to the absence of aggressive radiological markers. After a detailed discussion of diagnostic and management options, the patient declined confirmatory biopsy. Subsequently, the patient was administered 25 units of Btx type A (Btx A) into the left temporalis muscle. Her symptoms improved, with partial reduction in temporalis hypertrophy observed over a 3 month follow-up period. The patient expressed satisfaction with the treatment outcome and opted for continued monitoring without pursuing any additional interventions. Emphasis was placed on educating the patient about the recurrence or progression of symptoms.

Anterior view of the patient’s face showing swelling in the left temporal region.
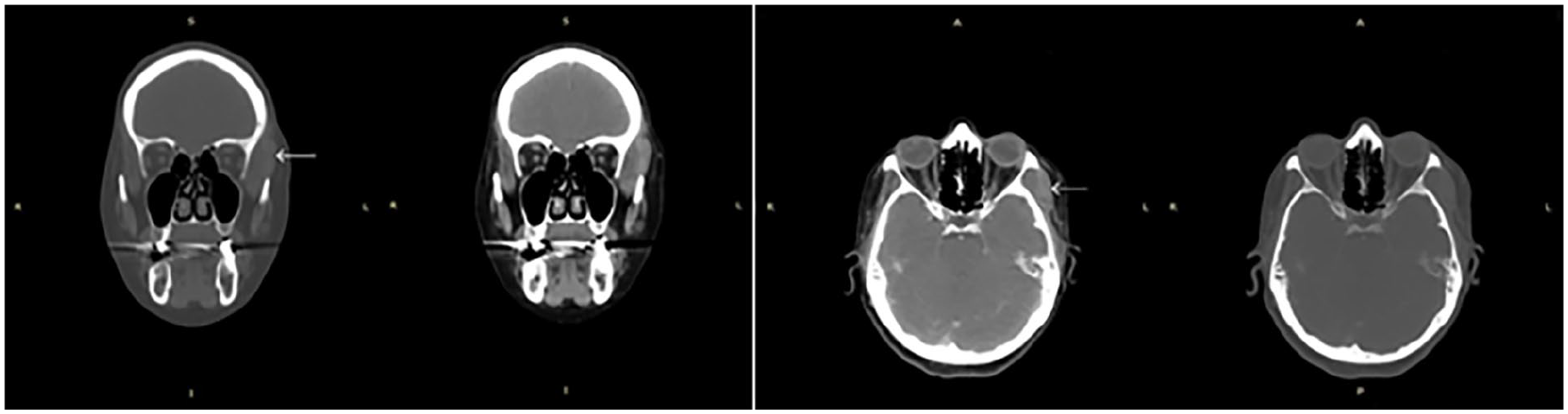
Contrast-enhanced CT scan with soft tissue window, axial, and coronal planes, demonstrating marked enlargement of the left temporal muscle, clearly evident compared with the contralateral side, and showing normal and homogeneous density. CT, computed tomography.
Discussion
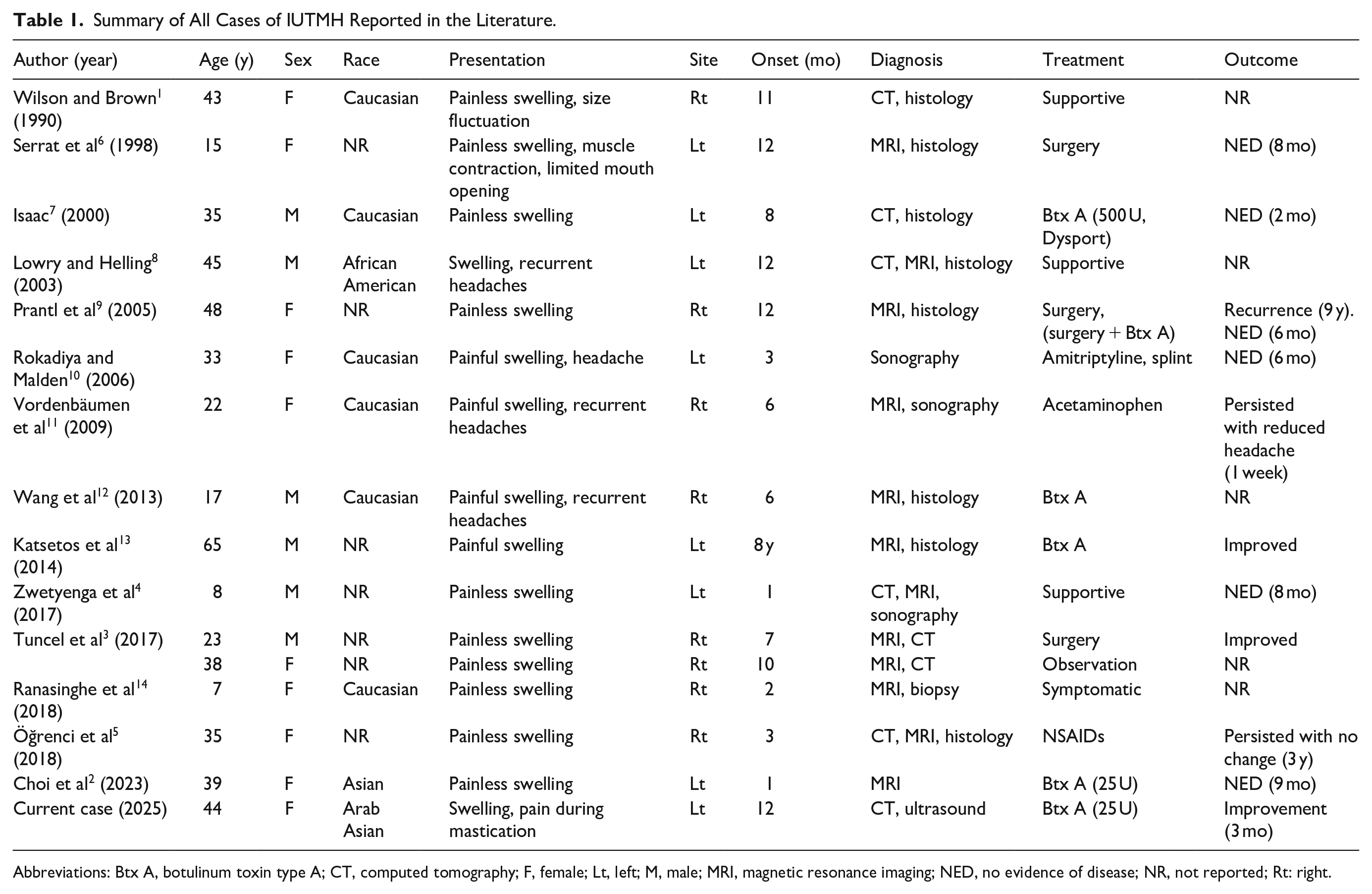
IUTMH is an exceptionally-rare condition, with only 16 cases documented in the literature, including the present report. A comprehensive review of these cases provides valuable insights into the clinical characteristics, diagnostic approaches, and therapeutic strategies for this uncommon entity.
The reported cases of IUTMH span a wide age range, from 7 to 65 years, affecting both pediatric and adult populations without a clear age predilection. A slight female predominance is observed, with 10 of the 16 cases occurring in females. The condition has been documented across diverse racial groups, including Caucasians, African Americans, Asians, and Arab Asians, suggesting no specific racial predisposition. This demographic variability underscores the need for heightened awareness of IUTMH across all patient populations presenting with temporal swelling. The hallmark of IUTMH is unilateral swelling in the temporal region, observed consistently across all cases. This swelling may be painless or accompanied by discomfort, particularly during mastication, as seen in the current case. Additional symptoms, such as headaches, limited mouth opening, or muscle contraction during function, are reported in a subset of patients, reflecting the heterogeneous clinical spectrum of the condition. This variability necessitates a meticulous clinical evaluation to differentiate IUTMH from other causes of temporal enlargement, such as neoplasms or inflammatory processes. Diagnosis of IUTMH relies heavily on imaging modalities, with CT and MRI being the most frequently-utilized tools to confirm muscle hypertrophy and exclude alternative pathologies. Ultrasonography is employed in some instances, offering a noninvasive means to assess muscle architecture, as demonstrated in the present case. Histological examination, when performed, typically reveals normal muscle tissue or hypertrophic changes without evidence of malignancy or inflammation, reinforcing the benign nature of IUTMH. The combination of imaging and, where indicated, biopsy ensures diagnostic accuracy in this rare condition. Management of IUTMH is highly individualized, reflecting the diversity in symptom severity and patient preferences. Conservative approaches, including observation and symptomatic relief with analgesics (eg, acetaminophen or nonsteroidal anti-inflammatory drugs (NSAIDs)), are common in cases with minimal discomfort. Btx A injections have emerged as a favored minimally-invasive option, effectively reducing muscle bulk and alleviating symptoms, as evidenced by the improvement in our patient following a 25 U injection. Surgical intervention, involving reduction in the hypertrophied muscle, is reserved for cases refractory to other treatments or those with significant functional or aesthetic concerns. The range of therapeutic options highlights the importance of tailoring management to each patient’s clinical profile. Outcomes following treatment are generally favorable, with many patients achieving symptomatic improvement or complete resolution, as indicated by reports of no evidence of disease (NED) over follow-up periods ranging from 2 months to 9 years. However, recurrence has been documented, notably in 1 case after 9 years, necessitating subsequent surgery and Btx A administration. This potential for recurrence emphasizes the value of long-term monitoring and personalized treatment plans. In the present case, Btx A administration resulted in symptomatic improvement and partial reduction in muscle size at the 3rd month, aligning with the positive outcomes observed in prior reports.
The aggregated data from Table 1 reveal intriguing patterns in treatment outcomes. For instance, Btx A demonstrated favorable results in 6 of 16 cases, with symptom improvement or NED reported within 2 to 9 months. Notably, lower doses [eg, 25 U in Choi et al (2023) and the current case] achieved outcomes comparable to higher doses [eg, 500 U in Isaac (2000)], suggesting that dose optimization may reduce risks of overtreatment without compromising efficacy. Conversely, surgical intervention, while effective in achieving immediate muscle reduction, was associated with recurrence in Prantl et al (2005), necessitating adjunctive Btx A. This underscores Btx A’s role as both a primary and adjuvant therapy. However, the heterogeneity in follow-up durations (2 months-9 years) complicates direct comparisons, emphasizing the need for standardized outcome metrics in future studies. While bruxism and parafunctional habits are frequently implicated, the absence of such history in 7/16 cases (eg, Zwetyenga et al, 2017; Wang et al, 2013) points to alternative mechanisms. Hypertrophy secondary to neurogenic stimuli, such as aberrant trigeminal nerve signaling, could explain cases with concurrent headaches (eg, Vordenbäumen et al, 2009). Additionally, hormonal influences—given the female predominance (10/16 cases)—warrant exploration, particularly in premenopausal women where estrogen may modulate muscle plasticity. The pediatric case by Zwetyenga et al (2017) further challenges stress-related theories, suggesting congenital or developmental factors. Muscle biopsy data, although sparse, could clarify these hypotheses by evaluating for denervation changes or receptor overexpression. Table 1 highlights that 4 cases utilized sonography, yet its diagnostic reliability remains underexplored. In the current case and Zwetyenga et al (2017), sonography confirmed hypertrophy but lacked specificity to exclude early neoplasms, necessitating complementary CT/MRI. Conversely, MRI’s superiority in delineating muscle architecture is evident in Katsetos et al (2014), where it identified reactive hypertrophy without mass effect. However, the reliance on imaging alone in 7 cases risks misdiagnosis, particularly in atypical presentations. A diagnostic algorithm incorporating risk stratification (eg, age, symptom progression) could guide judicious use of biopsy, balancing patient reluctance with diagnostic certainty. The aesthetic and functional burden of IUTMH is underreported. For instance, Serrat et al (1998) documented limited mouth opening, while the current case highlighted pain during mastication—both impacting quality of life. Patient-reported outcomes (eg, validated scales for pain, anxiety, or social function) are absent in existing literature but could refine therapeutic goals, particularly in electing invasive versus conservative approaches. The recurrence in Prantl et al (2005) after 9 years underscores the necessity for lifelong monitoring, even in “resolved” cases. Table 1 shows that only 3/16 cases reported follow-up beyond 1 year, creating a recurrences bias favoring short-term efficacy. Prolonged surveillance could identify late recurrences or compensatory hypertrophy in contralateral muscles, as hypothesized in Lowry and Helling (2003). Additionally, the pediatric case by Zwetyenga et al (2017) raises questions about growth-related progression, necessitating age-tailored follow-up protocols. Emerging therapies, such as ultrasound-guided Btx A or platelet-rich plasma injections, remain unexplored in IUTMH. Precision-guided Btx A may enhance targeting and reduce diffusion-related side effects. Furthermore, noninvasive modalities like physiotherapy or biofeedback—effective in other masticatory disorders—could be trialed in asymptomatic or minimally-symptomatic cases. Collaborative trials across centers could accelerate the evaluation of these novel approaches.
Summary of All Cases of IUTMH Reported in the Literature.
Abbreviations: Btx A, botulinum toxin type A; CT, computed tomography; F, female; Lt, left; M, male; MRI, magnetic resonance imaging; NED, no evidence of disease; NR, not reported; Rt: right.
The current case, involving a 44-year-old woman with progressive left temporal swelling and masticatory discomfort, mirrors the typical presentation of IUTMH. Diagnostic imaging via CT and ultrasound confirmed isolated hypertrophy of the left temporalis muscle, and Btx A treatment yielded a favorable response, consistent with findings from the literature. This case contributes to the limited body of evidence on IUTMH and reinforces the efficacy of Btx A as a therapeutic modality. IUTMH remains a rare but significant differential diagnosis in patients presenting with unilateral temporal swelling. Its broad clinical spectrum, reliance on imaging for diagnosis, and varied management options highlight the complexity of this condition. While outcomes are generally positive, the possibility of recurrence warrants ongoing vigilance. Continued reporting of cases like ours is essential to deepen the understanding of IUTMH’s etiology and optimize treatment strategies, ultimately improving patient care.
Conclusion
In conclusion, IUTMH remains a rare and intriguing clinical entity, as evidenced by the limited number of cases reported in the literature. This case underscores the importance of a meticulous diagnostic approach, leveraging imaging modalities like CT and ultrasound to confirm the diagnosis while ruling out alternative pathologies. The favorable response to Btx A in our patient aligns with emerging evidence supporting its efficacy as a minimally-invasive treatment option. However, the potential for recurrence and the unclear etiology of IUTMH highlight the need for a long-term follow-up and further research to elucidate its underlying mechanisms. By contributing to the growing body of knowledge on IUTMH, this report emphasizes the value of detailed case documentation to refine diagnostic and therapeutic strategies, ultimately enhancing patient outcomes in this uncommon condition.
Footnotes
Ethical Considerations
Our institution does not require ethics approval for reporting individual cases.
Consent for Publication
Written informed consent was obtained from the patient for publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the author or corresponding author upon reasonable request.