
Abstract
This article presents the case of a 37-year-old female patient who was admitted to the hospital with a sore throat after accidentally ingesting a chicken bone. Multiple computed tomography scans revealed a striated hyperdense shadow along the posterior pharyngeal wall, which was initially misdiagnosed as an esophageal foreign body. However, subsequent endoscopic evaluations failed to identify any foreign object. After further imaging studies and multidisciplinary consultation, the final diagnosis was physiologic calcification of the posterior lamina of the cricoid cartilage. This case highlights the importance of distinguishing between laryngeal cartilage calcification and esophageal foreign bodies on imaging to avoid unnecessary interventions.
Introduction
Cricoid cartilage calcification is a physiological change in the laryngeal cartilage that occurs with aging and may be misinterpreted as a pathological finding due to its imaging similarity to esophageal foreign bodies. 1 Esophageal foreign bodies, often caused by ingestion of sharp food items such as poultry bones or fish spines, typically become lodged in the narrower segments of the esophagus and can lead to serious complications if not promptly managed. Radiologic imaging plays a pivotal role in differentiating these 2 entities. Calcification of the cricoid cartilage typically appears as a dense, well-defined structure confined within the anatomical boundaries of the cartilage, with regular morphology and no signs of surrounding inflammation. In contrast, esophageal foreign bodies usually display irregular shapes that extend beyond the cartilage margin and are often accompanied by mucosal edema or other inflammatory changes. Despite these distinctions, misdiagnoses still occur, as evidenced by reports in the literature. In this article, we present a case involving strip-like calcification of the posterior lamina of the cricoid cartilage that was initially misdiagnosed as an esophageal foreign body.
Case Presentation
Patient You XX, female, 37 years old, after accidentally eating chicken bones, I experienced pain in the posterior pharyngeal wall and sought medical treatment at a local hospital on the same day. A computed tomography (CT) scan of the neck revealed a strip-like high-density shadow along the posterior pharyngeal wall, which, combined with the patient’s clinical history, was initially considered to represent a possible pharyngeal bony foreign body. The patient subsequently underwent gastroscopy under general anesthesia; however, no foreign body or mucosal injury was detected during the procedure (Figure 1). The patient was admitted for observation following the gastroscopy. Two days later, the patient’s pharyngeal pain persisted. A repeat CT scan showed a striated hyperdense shadow in the posterior pharyngeal wall, located at the same site as previously noted (Figure 2). A second gastroscopy was performed, yet again, no foreign body was found. Upon further analysis, it was noted that mucosal exposure in the posterior hypopharyngeal region during gastroscopy was insufficient. Therefore, the examination method was changed to direct laryngoscopy to improve visualization. Despite achieving adequate exposure of the posterior hypopharyngeal ring, no foreign body or mucosal disruption was identified.
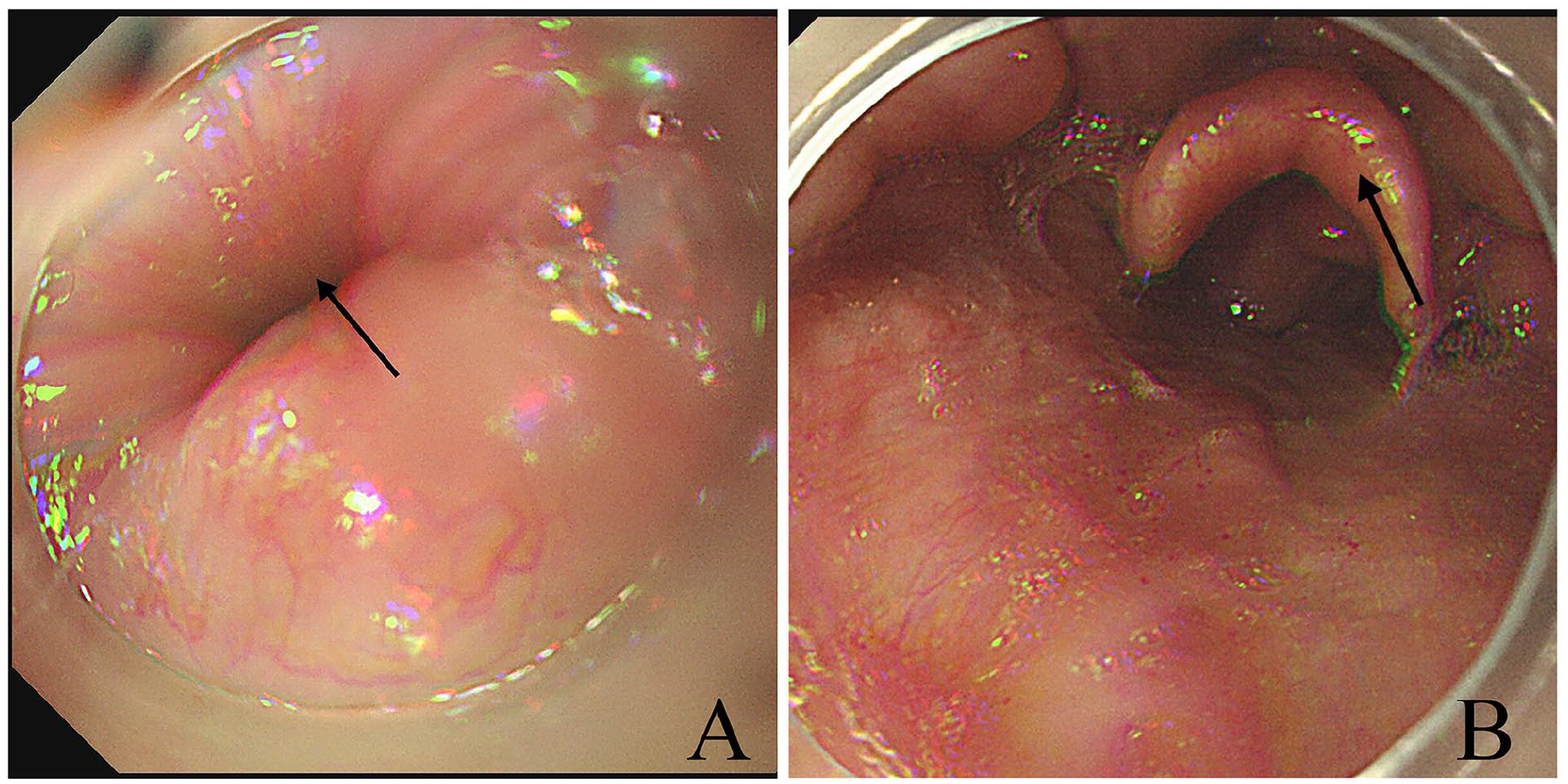
Gastroscopic image showing smooth esophageal mucosa with no foreign bodies or ulcers. (A) Black arrow shows the esophageal inlet; (B) black arrow shows the epiglottis.
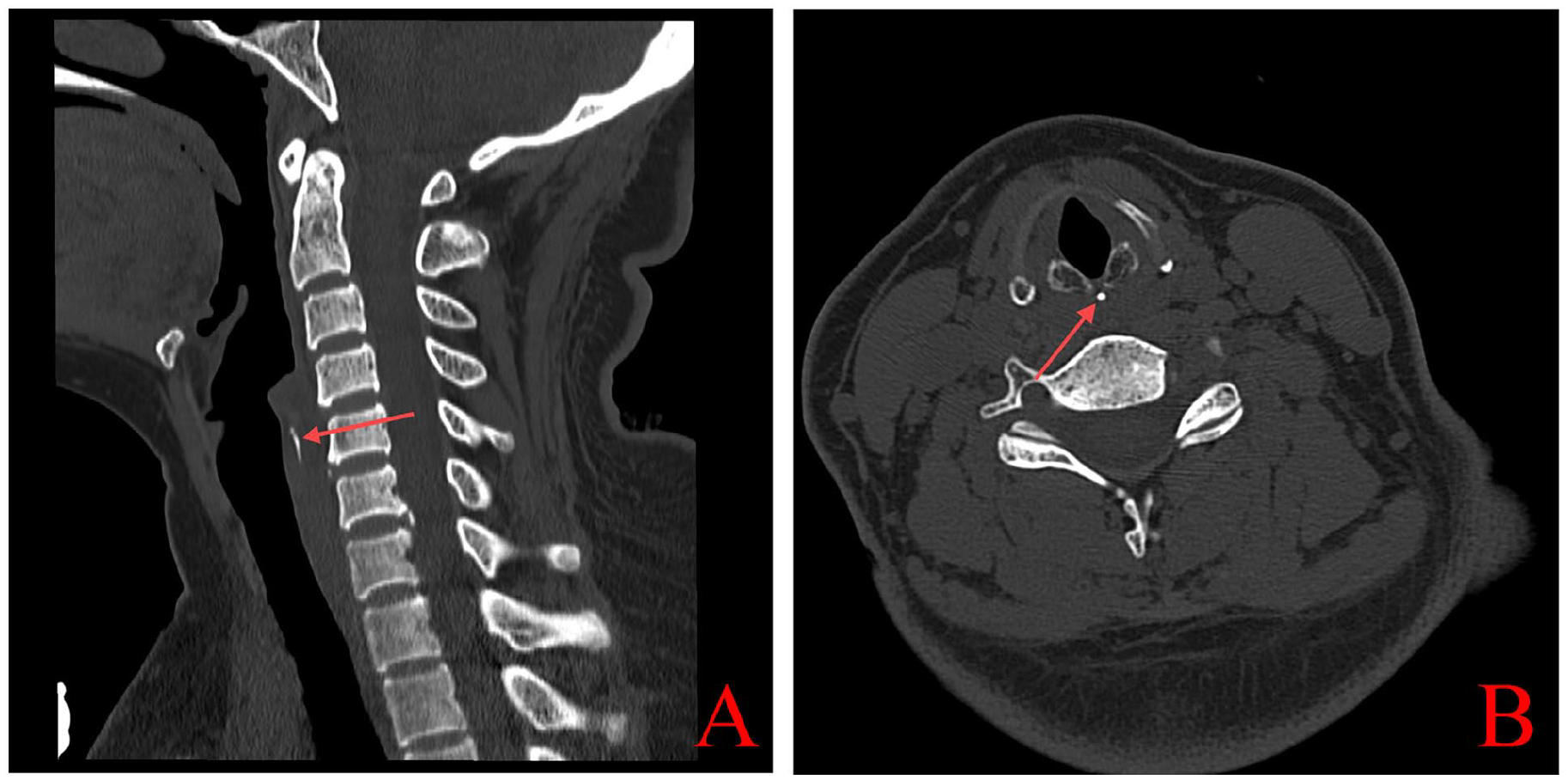
CT examination of the neck (A) sagittal view, calcified image of annular cartilage in the shape of a bar shown by red arrows; (B) horizontal view, calcified annular cartilage shown by red arrows. CT, computed tomography.
The patient was transferred to our hospital on the fifth day, for further diagnosis and treatment. A fiberoptic laryngoscopy was performed (Figure 3). When the endoscope reached the level of the arytenoid region, the patient was instructed to perform a balloon-blowing maneuver while pulling the anterior cervical skin to fully expose the posterior hypopharyngeal cricoid region. The endoscope was then advanced to probe the pyriform fossa on both sides. The mucosal membranes were observed during the “clothes” sound, revealing no foreign bodies, and there were no signs of local redness, swelling, or ulceration. To further clarify the diagnosis, a hypopharyngeal CT scan was performed, which revealed a longitudinal strip of high-density shadow posterior to the cricoid cartilage at the level of the fifth cervical vertebra. The remainder of the esophagus showed no abnormal density shadows, and there was no thickening of the bilateral soft tissue walls. After reviewing the imaging results and consulting with the imaging department, the final diagnosis was identified as calcification of the posterior cricoid cartilage, which was a physiological change rather than foreign body implantation. Following detailed discussions, the patient was discharged for observation, avoiding unnecessary surgery or interventions. Five days after discharge from the hospital, the patient experienced a significant reduction in pain. The patients were followed up and observed until the seventh day after discharge, during which no recurrence of pharyngeal pain was noted.
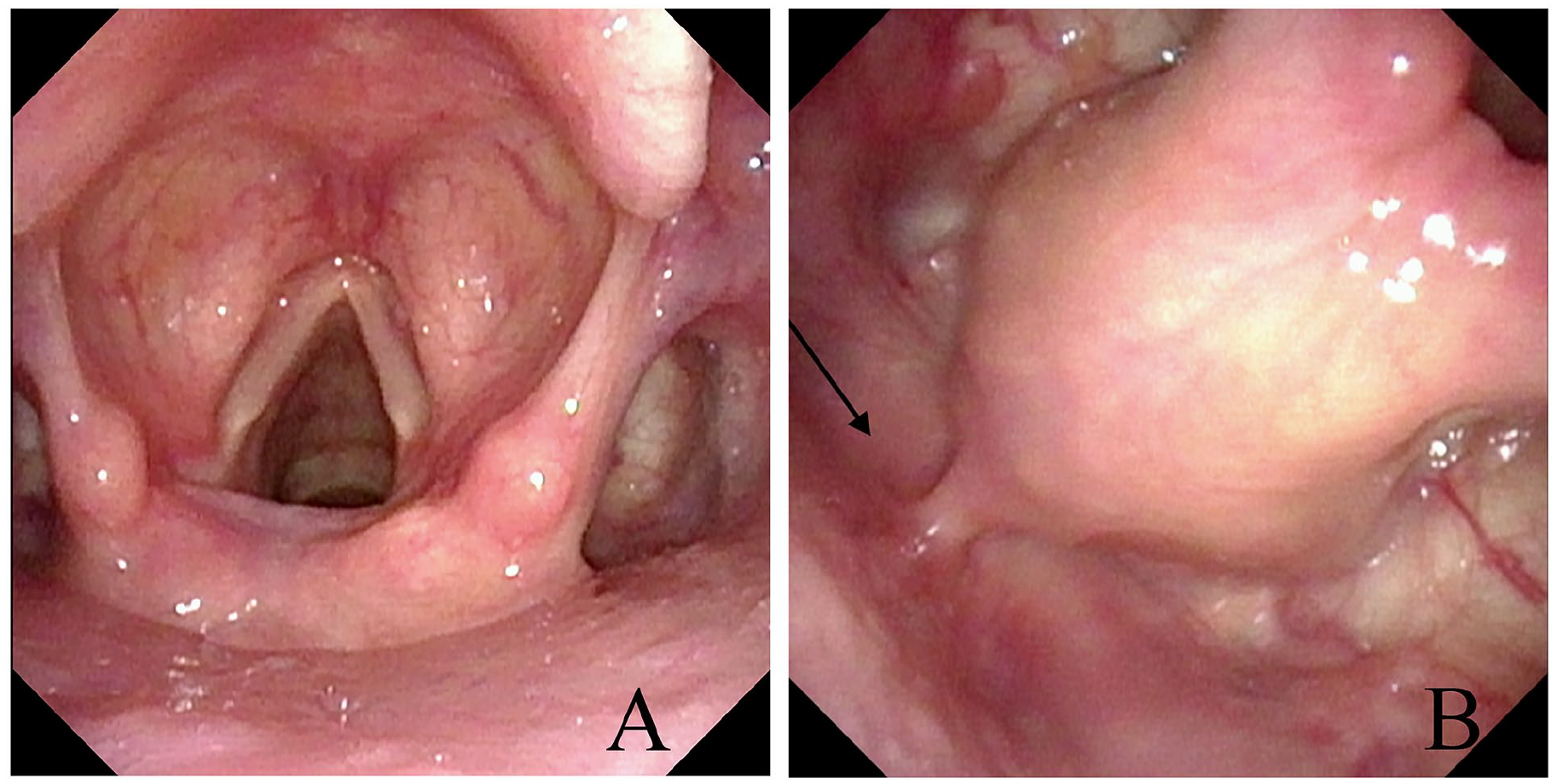
Electron fiberoptic laryngoscopy (A) overall view of the laryngeal cavity (B) posterior cricoid area shown by the black arrow, cricopharyngeal mucosa is intact and free of abnormality.
Discussion
Foreign body impaction due to food ingestion is a common yet potentially serious acute condition in otolaryngology. Delayed or inappropriate management can result in severe complications, including life-threatening outcomes. 2 Sharp foreign bodies such as fish bones or poultry bones are frequent culprits and often become lodged in anatomically narrow regions, including the tonsils, base of the tongue, pyriform fossa, or upper esophagus. Esophageal foreign bodies are more commonly seen in children, the elderly, individuals with intellectual disabilities or psychiatric disorders, and those under the influence of alcohol. Without timely intervention, complications such as mucosal ulceration, esophageal perforation, peri-esophageal abscess, bronchoesophageal fistula, pneumothorax, mediastinitis, vascular injury, pseudoaneurysm, and pericarditis may occur. 3 Therefore, prompt and accurate diagnosis of esophageal foreign bodies is crucial in clinical practice.
The cricoid cartilage is the only complete ring-shaped cartilage in the larynx. It provides structural support for the larynx, serves as an attachment site for muscles and ligaments, and plays an essential role in phonation and swallowing. Research has shown that the cricoid cartilage undergoes progressive physiological calcification or ossification with age. Arasaratnam et al described a developmental pattern of laryngeal cartilage calcification in which the hyoid, thyroid, and tracheal cartilages show calcification in infancy; the thyroid cartilage begins calcifying around the ages of 20 to 30 years, and the cricoid cartilage calcifies either concurrently with or prior to the thyroid cartilage. 4 In the cricoid cartilage, calcification typically starts in the posterior lamina and progresses along the cartilaginous arch. 5 Although the exact cause of this calcification remains unclear, MS proposed an embryological hypothesis suggesting that the right and left sixth branchial arches fuse at the midline to form the posterior lamina of the cricoid cartilage. 6 The midline region may represent a zone of relatively poor blood supply during embryonic development, leading to localized hypoxia and accumulation of metabolic by-products, which promote calcium salt deposition. This hypothesis may explain why calcification tends to begin at the midline of the posterior plate and extend anteriorly toward the cricoid arch.
The differential diagnosis between linear calcification of the cricoid cartilage and esophageal foreign bodies remains a significant clinical challenge. On CT imaging, several distinguishing features can aid in accurate identification. First, physiologic linear calcification of the cricoid cartilage typically appears as a thin, well-defined hyperdense structure confined strictly within the boundaries of the cartilage, not extending beyond its superior or inferior margins. In contrast, hyperdense, irregular, or heterogeneous shadows caused by impacted esophageal foreign bodies often extend beyond the anatomical confines of the cricoid cartilage and exhibit irregular morphology. 7 Second, esophageal foreign bodies are frequently associated with signs of surrounding mucosal edema or exudation on CT, whereas cricoid cartilage calcification usually presents without any such inflammatory changes.
As a noninvasive and rapid diagnostic method, CT imaging is currently the first choice for detecting esophageal foreign bodies, particularly bony foreign bodies, which it can identify with significant advantages. 8 Additionally, CT plays a crucial role in assessing complications such as esophageal perforation and mediastinal emphysema. 9 CT can provide direct evidence of foreign bodies, such as the presence of stripes or irregular high-density shadows in the esophagus. However, inexperienced physicians may misinterpret the calcification of various tissues as an esophageal foreign body. Several cases of such misdiagnosis have been documented, including the misidentification of arterial ligament calcification as an esophageal foreign body, thyroid cartilage calcification as an esophageal foreign body, and calcification of the lingual ligament in children as an esophageal foreign body.10-12 Despite its strengths, CT can sometimes struggle to detect smaller foreign bodies, such as small fishbones, which may appear as faint, dense shadows and can be difficult to differentiate from surrounding artifacts. 13 Electrogastroscopy is also an important tool for foreign body detection, offering direct visualization and the ability to remove foreign bodies. However, its limitation lies in its ability to visualize only the foreign body within the esophageal lumen, especially when the object is located near the cricoid cartilage, making it significantly harder to detect via gastroscopy. 14
In this case, the patient had a clear history of accidentally ingesting a chicken bone and presented with symptoms of dysphagia and throat pain. Plain radiography of the neck revealed a calcium-dense structure approximately 5 mm in length at the level of the cricopharyngeal muscle, positioned outside the esophageal lumen an appearance that, at first glance, could easily be mistaken for a chicken bone. However, further CT imaging demonstrated that the calcification was located between the esophageal lumen and the posterior plate of the cricoid cartilage, closely associated with the midline region of the posterior cricoid plate. This imaging appearance is particularly prone to being misdiagnosed as a penetrating esophageal foreign body. 6
The misdiagnosis in this case highlights the limitations of a “history-first” diagnostic mindset in clinical practice. The patient’s clear history of swallowing a chicken bone, combined with throat pain, may have led clinicians to overlook key imaging features and prematurely conclude the presence of an esophageal foreign body. Studies have shown that approximately 1% of suspected esophageal foreign body cases are ultimately identified as normal anatomical variations or calcifications, with cricoid cartilage calcification accounting for the majority . Additionally, primary care institutions often lack sufficient awareness of the imaging characteristics of laryngeal cartilage calcification. In particular, they may fail to appreciate the anatomical distinction between calcifications seen at the level of the fifth cervical vertebra more typical of cricoid cartilage and true esophageal foreign bodies, which are usually located below the sixth cervical vertebra. 11 This misunderstanding further contributes to misinterpretation of imaging findings. In our clinical experience, we have encountered other forms of cricoid cartilage calcification (e.g., Figure 4), such as double-layer calcification, which is more easily distinguished from esophageal foreign bodies on imaging due to its characteristic bilateral symmetry and defined anatomical location.
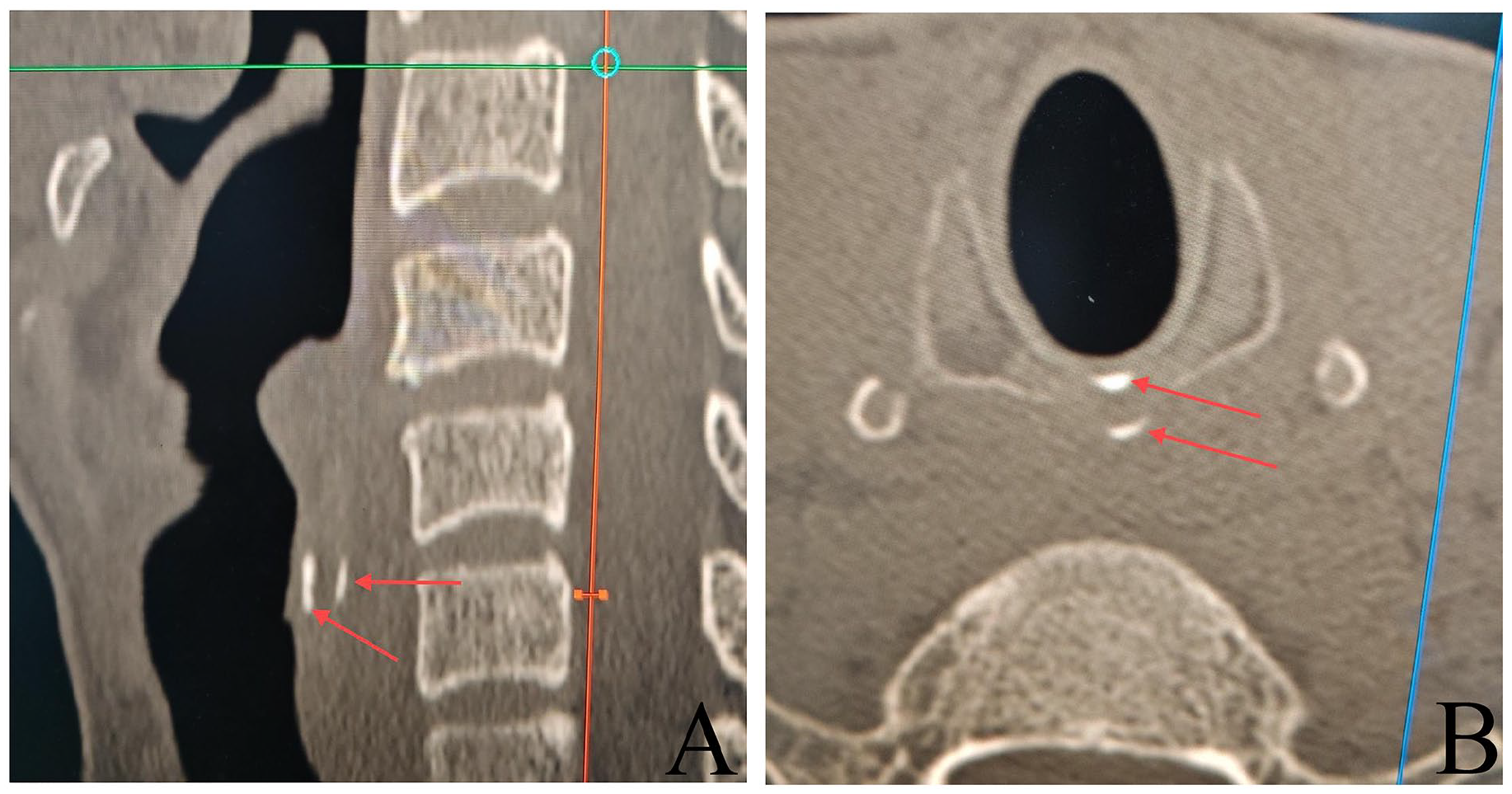
CT in a patient with bilayer calcification of the anterior and posterior plates of the cricoid cartilage (A) sagittal view, red arrows show bilayer calcification of the anterior and posterior plates of the cricoid cartilage; (B) horizontal position, red arrows show the cricoid cartilage bilayer. CT, computed tomography.
We summarize the following key points based on our experience: First, remain vigilant against empirical errors. Even when clinical history, symptoms, and auxiliary examinations suggest an esophageal foreign body, imaging should be carefully reviewed to avoid missed or incorrect diagnoses. Second, note that cricoid cartilage ossification on CT typically appears at the level of the fourth to fifth cervical vertebrae, whereas esophageal foreign bodies are usually located at the level of the sixth cervical vertebra or below. Third, thorough attention should be given to the patient’s medical history to correctly identify cricoid cartilage calcification, which may mimic a foreign body. Fourth, clinical decision-making should adhere to the principle of “imaging first, endoscopy second” to prevent unnecessary interventions.
Conclusion
Calcification of the cricoid cartilage is an important differential diagnosis in cases of misdiagnosis of esophageal foreign bodies. Clinicians must be aware of this physiological change, make full use of imaging techniques, and engage in multidisciplinary discussions to prevent unnecessary invasive procedures.
Footnotes
Acknowledgements
We would like to express our gratitude to the patient and his family for their cooperation and consent.
Consent for Publication
All authors approved the submitted version.
Consent to Publish
The patient’s written informed consent has been obtained, including the consent for publication.
Author Contributions
Responsible for paper writing and data collation: CSL; In charge of data collation and photo collection: QYC; Focused on data collation and provided paper guidance: DZS; Conducted case analysis and provided paper guidance: XQC; Developed writing ideas and design, and was responsible for paper guidance and revision: HQL. All authors contributed to manuscript revision, read, and approved the submitted version.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.