
Abstract
Background:
Retained wooden foreign bodies in the maxillary sinus, particularly with prolonged latency, pose significant diagnostic, and therapeutic challenges due to their low radiodensity and resemblance to fungal infections on imaging. This case highlights the role of electromagnetic navigation-guided endoscopic sinus surgery (ENG-ESS) in managing complex long-latency foreign bodies.
Case Presentation:
A 31-year-old man presented with recurrent right infraorbital abscesses and facial swelling for over a year and was initially misdiagnosed with fungal sinusitis. Conventional treatments, including multiple abscess drainage and endoscopic sinus fenestration, failed to resolve the symptoms. Imaging revealed a high-density maxillary sinus shadow, which was later identified as a 4.5 cm wooden fragment retained for 5 years post-trauma. The initial endoscopic removal of a smaller fragment provided transient relief. ENG-ESS subsequently localized and removed the residual migratory fragment extending to the orbital wall, leading to complete resolution of the infection.
Conclusion:
This case underscores the diagnostic pitfalls of wooden foreign bodies and advocates for integrating trauma history with advanced imaging. ENG-ESS demonstrated superior precision in navigating complex anatomy and reducing the risk and complications of residual foreign bodies. We propose a trauma history dynamic imaging-navigation surgery framework for long-latency refractory cases.
Keywords
Introduction
Nonodontogenic retained foreign bodies, such as wood, are rare in the maxillary sinus, 1 particularly those with a prolonged latency exceeding 5 years. The low radiodensity and overlapping imaging features often lead to misdiagnosis as fungal balls or chronic sinusitis. While conventional endoscopic surgery faces limitations in visualizing deeply embedded foreign bodies, electromagnetic navigation-guided endoscopic sinus surgery (ENG-ESS) integrates preoperative 3-dimensional (3D) imaging with real-time intraoperative tracking, 2 significantly improving precision in complex anatomical regions and reducing mucosal injury and operative time. This is the first systematic evaluation of the ENG-ESS for managing migratory wooden foreign bodies.
Case Presentation
A 31-year-old man initially presented with swelling of the right lower eyelid without an obvious cause 1 year ago, followed by swelling and pain on the right side of the face. Previous treatments included multiple drainage of the lower eyelid abscess, resection of a skin sinus in the right lower eyelid, and endoscopic multiple sinus fenestration. 3 Initial endoscopic surgery partially removed a 2.5 cm wooden fragment, leading to transient symptom relief. However, recurrence occurred 3 months postoperatively because of a residual foreign body. The details of the patient’s 2 visits are provided below.
First Admission
The patient presented with pain and swelling of the right lower eyelid with recurrent purulent discharge for 1 year without obvious inducement. Physical examination revealed no deformity of the external nose, no abnormal secretions or neoplasms in the bilateral nasal cavities, and tenderness in the sinus region. A 0.5 × 0.5 cm skin ulcer was observed on the right lower eyelid, with yellow purulent secretion communicating with the maxillary sinus and a surrounding depression and deformity. Additionally, a 2 cm incision at the right eyebrow tail was noted to heal well. Computed tomography (CT) and contrast-enhanced CT revealed right maxillary sinus and sphenoid sinusitis with partial retention of sinus secretions and a high-density shadow in the right maxillary sinus, suspected to be a fungal ball in the paranasal sinuses (Figure 1a). Endoscopic sinus drainage was performed after excluding contraindications. Intraoperatively, a 2.5 cm wooden fragment was found in the maxillary sinus cavity, and pathological examination of the tissue fragment confirmed inflammation (Figure 1b). The symptoms of skin infection of the right lower eyelid significantly improved after surgery, and the patient was subsequently discharged.
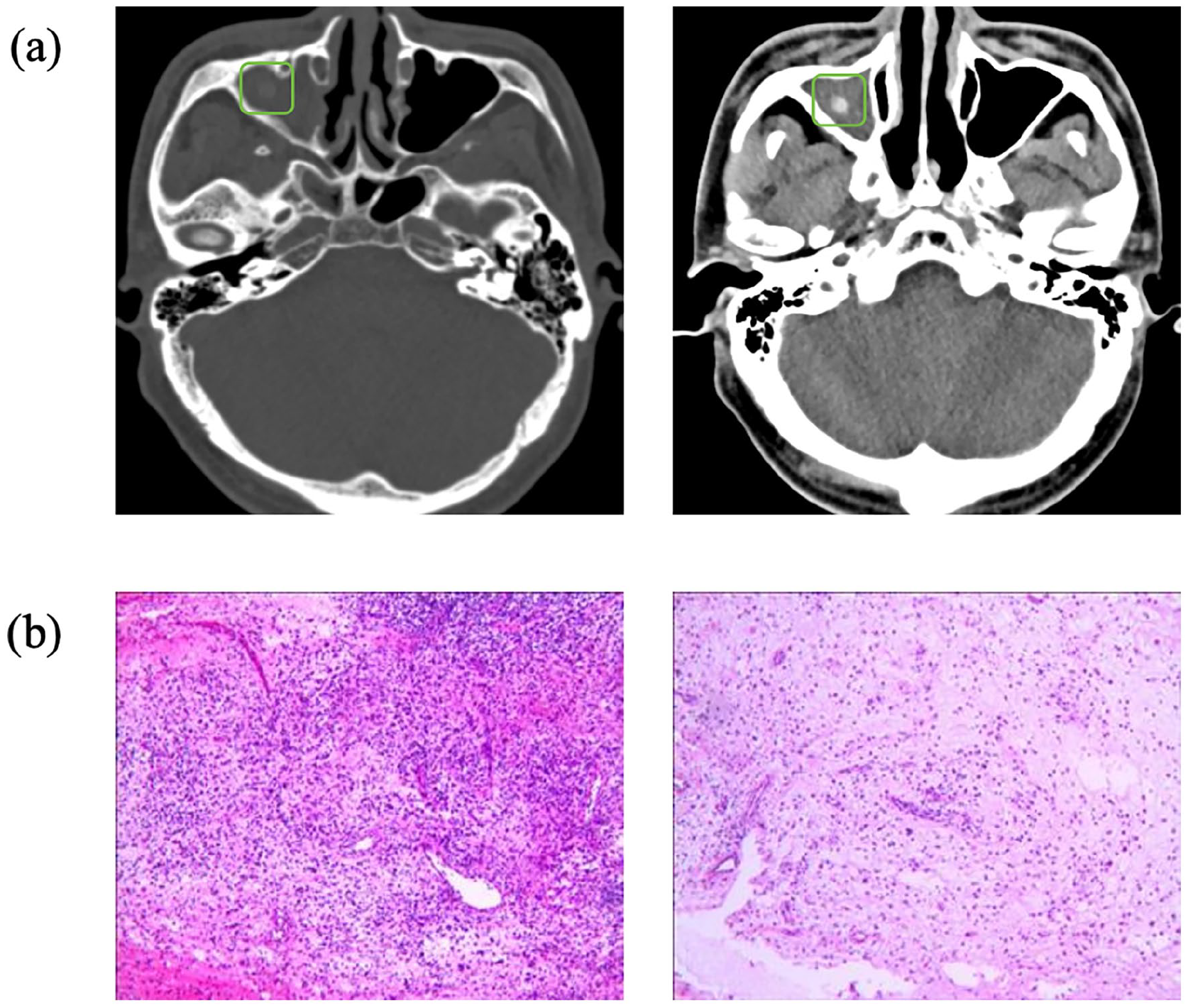
(a) CT shows: bilateral frontal, ethmoid, right maxillary, and sphenoid sinuses with partial sinus secretion retention (right maxillary sinus may have a fungal infection). (b) Pathological examination of the tissue fragment confirmed inflammation: many inflammatory cells infiltration in the fibrous connective tissue, focal hemorrhage, combined with clinical changes consistent with inflammation. CT, computed tomography.
Second Admission
Three months postoperatively, the patient experienced a recurrence and aggravation of the skin infection on the right lower eyelid, which persisted for 2 weeks. Considering that the patient’s repeated ulcer and infection of the infraorbital skin were related to the maxillary sinus foreign bodies, combined with the patient’s medical history, the possibility of residual foreign bodies could not be excluded. A follow-up navigation sinus CT revealed an abnormal density in the right maxillary sinus extending into the right orbit through a defect in the upper wall of the sinus (Figure 2a). After excluding surgical contraindications, ENG-ESS was performed for foreign body removal. During surgery, the maxillary sinus cavity was exposed and white pus was observed. After cleaning, a 4.5 cm long stick was found lodged vertically in the nasal cavity and surrounded by significant granulation tissue. The foreign body was successfully removed using intact forceps (Figure 2b).
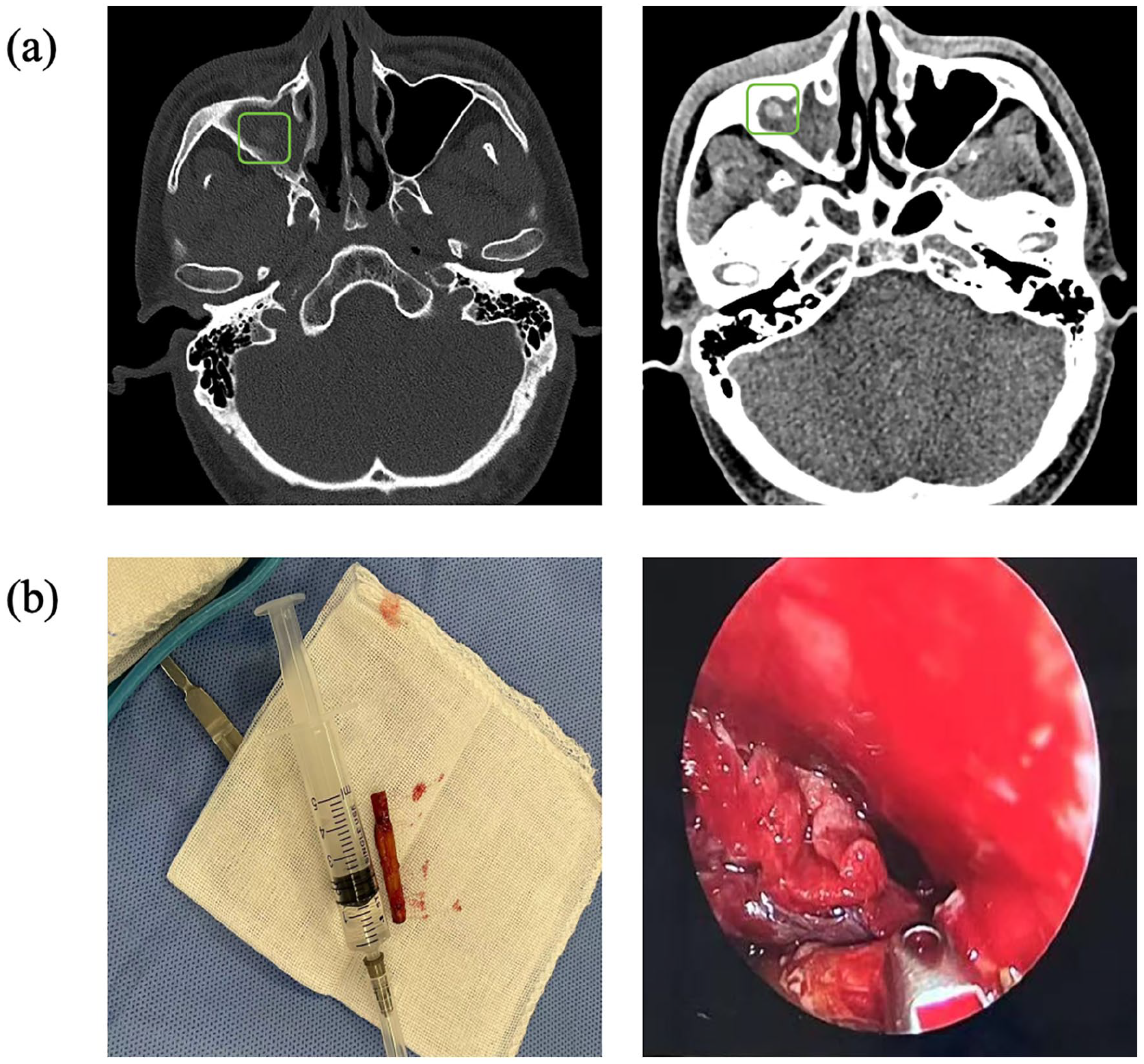
(a) Navigation sinus CT revealed. (1) The abnormal density in the right maxillary sinus extended to the right orbit through a local defect in the upper wall, and the lower eyelid was swollen with pneumatosis. Based on the medical history, infectious lesions, and sinus formation were considered. (2) Bilateral frontal, ethmoid, and sphenoid sinusitis. (b) White pus was observed in the maxillary sinus cavity. A white wooden stick was placed vertically in the nasal cavity, and a large amount of granulation tissue hyperplasia was observed around it. CT, computed tomography.
Considering the complex nature of the patient’s condition and the specific nature of the foreign body removed during surgery, the patient’s medical history was re-evaluated. The patient recalled that 5 years earlier, after an inebriated altercation, a chopstick was inserted into the right side of his cheek, but he could not remember the incident. The chopstick was removed without any medical intervention. Therefore, we considered that the foreign body retained in the right maxillary sinus after trauma caused recurrent infection on the right side of the face. The proximity of the foreign body to the orbit makes the anatomy complex and challenging. Therefore, we completely removed the foreign body using ENG-ESS and thoroughly cleaned the sinus cavity. Postoperatively, the infection symptoms improved, and the wound healed well without any complications. After 6 months of follow-up, the sinus tract of the right lower eyelid healed without any reinfection.
Discussion
Foreign bodies in the maxillary sinus can be categorized based on their origin as endogenous, exogenous, 4 iatrogenic, 5 and biological. 6 In this case, the patient was misdiagnosed with an infraorbital abscess due to the presence of a wooden foreign body that had remained in the maxillary sinus for 5 years without obvious symptoms of chronic rhinosinusitis or other accompanying symptoms and a lack of a clear medical history. The patient underwent several abscess debridements, but the symptoms persisted without significant improvement. Subsequently, the patient was misdiagnosed with fungal sinusitis.7,8 After exploration of the maxillary sinus, a wooden foreign body was removed, and sinus CT was not reviewed after surgery, ignoring the possibility of residual and displaced foreign bodies, which resulted in recurrent suborbital infection without improvement. Finally, under the guidance of electromagnetic navigation, the foreign body was accurately located and completely removed. The patient recovered after an incubation period of 5 years, and the patient recovered. The occurrence and development of such cases are extremely rare. Only a few cases report concerning wooden foreign bodies,9,10 no analogous case has been reported previously that lacks nasal sinus symptoms for 5 years, exhibits a prolonged residual period, and extended to the orbital wall, which is rare in the literature. In addition, the diagnosis was difficult because of the unclear medical history and the foreign body was wrapped by the surrounding tissue. Compared to iatrogenic metallic implants, wooden foreign bodies exhibit isodense imaging characteristics owing to their low radiodensity. Unless accompanied by calcification or secondary inflammatory changes, they are prone to misdiagnosis as fungal ball 7 or mucocysts.
The maxillary sinus is anatomically close to the orbit, nasolacrimal duct, and pterygopalatine fossa. Therefore, infection, trauma, and tumors in this region are prone to lead to serious complications, such as osteolytic bone destruction, orbital cellulitis, and, rarely, intracranial dissemination. In this case, the foreign body extended to the right orbit through the local defect of the superior wall, yet the patient did not experience facial numbness, diplopia, decreased vision, or restricted eye movement, suggesting that the trauma did not damage the infraorbital canal 11 or optic nerve. The presence of right infraorbital involvement in the fifth year posttrauma indicates the risk of retention and displacement of foreign bodies in the maxillary sinus.
ESS is commonly employed to treat sinusitis and remove nasal foreign bodies. However, when lesions involve critical anatomical structures, such as the optic nerve, pterygopalatine fossa, and skull base, there is an increased risk of severe complications or residual lesions. This risk is influenced by several factors, including anatomical variation, lesion extent, surgical bleeding, and operator experience and technique. Traditional ESS is prone to incomplete removal of deeply buried or granuloma-wrapped foreign bodies. ENG-ESS12,13 enables preoperative 3D imaging and precise intraoperative localization of foreign bodies, which can be combined with real-time intraoperative tracking, helping to avoid the limitations of traditional nasal endoscopy, which cannot integrate preoperative imaging with real-time tracking. Compared with traditional endoscopy, ENG-ESS shortens the operation time, minimizes mucosal injury, and reduces the incidence of complications, providing a more precise and safer approach for minimally invasive nasal endoscopic surgery. In contrast to previous reports relying on traditional endoscopy, this study is the first to systematically apply ENG-ESS for the accurate localisation and complete removal of deeply embedded wooden foreign bodies, which avoids the limitations of foreign body removal under traditional nasal endoscopy.
Conclusion
This case underscores the diagnostic challenges and management complexities associated with nonodontogenic retained foreign bodies in the maxillary sinus, particularly those of organic origin. The prolonged latency period and migratory nature of the wooden fragment highlight the importance of a thorough patient history and advanced imaging techniques for removing refractory foreign bodies. This case emphasises the need for clinicians to maintain a high suspicion of retained foreign bodies in cases of refractory sinonasal symptoms, especially when there is a history of facial trauma. Furthermore, we propose a trauma history dynamic imaging navigation surgery framework for long-latency cases and illustrate the potential of ENG-ESS to enhance surgical precision and safety in complex sinonasal pathologies, reduce complications and improve patient outcomes.
Footnotes
Acknowledgements
We thank the patient in this study for his invaluable cooperation and our colleagues for their support.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Written consent was obtained from the patient to publish anonymized information in this article.
Author Contributions
S.W. and C.X.: designed the project. J.H. and X.L.: acquired and analysed the data. C.X.: drafted the manuscript. X.X. and S.W.: approved the final version for publication and agreed to be accountable for all aspects of the work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge the support from the Gansu Provincial Hospital Intra-Hospital Research Fund Project-Master Tutor Cultivation Plan (22GSSYB-1), the Natural Science Foundation of Gansu Province (25JRRA340), the Excellent Introduction of Talents and Doctoral Start-up Fund projects (RCBS-2023-001).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.