
Abstract

Significance Statement
This case highlights a rare instance of imatinib-associated temporal bone osteonecrosis, expanding awareness of potential adverse effects of long-term tyrosine kinase inhibitor therapy. It underscores the diagnostic challenge of persistent otological symptoms and the importance of considering medication-related bone complications in differential diagnoses. By documenting this uncommon presentation, the report contributes valuable clinical insight for otolaryngologists managing patients on targeted cancer therapies.
A 58-year-old man with chronic myelogenous leukemia (CML) presented with a 3-month history of persistent bilateral ear itching and otorrhea. He had been taking 400 mg of imatinib daily for 5 years, with no prior history of radiotherapy or bisphosphonate use. His medical history was otherwise unremarkable, and he had no known predisposing factors for osteonecrosis.
Otoscopic examination revealed bilateral bony erosion and necrosis of the inferior walls of the external auditory canals (EACs), accompanied by purulent discharge. The tympanic membranes appeared intact without evidence of perforation. There were no significant signs of acute mastoiditis, although the EACs were markedly inflamed and eroded (Figure 1).
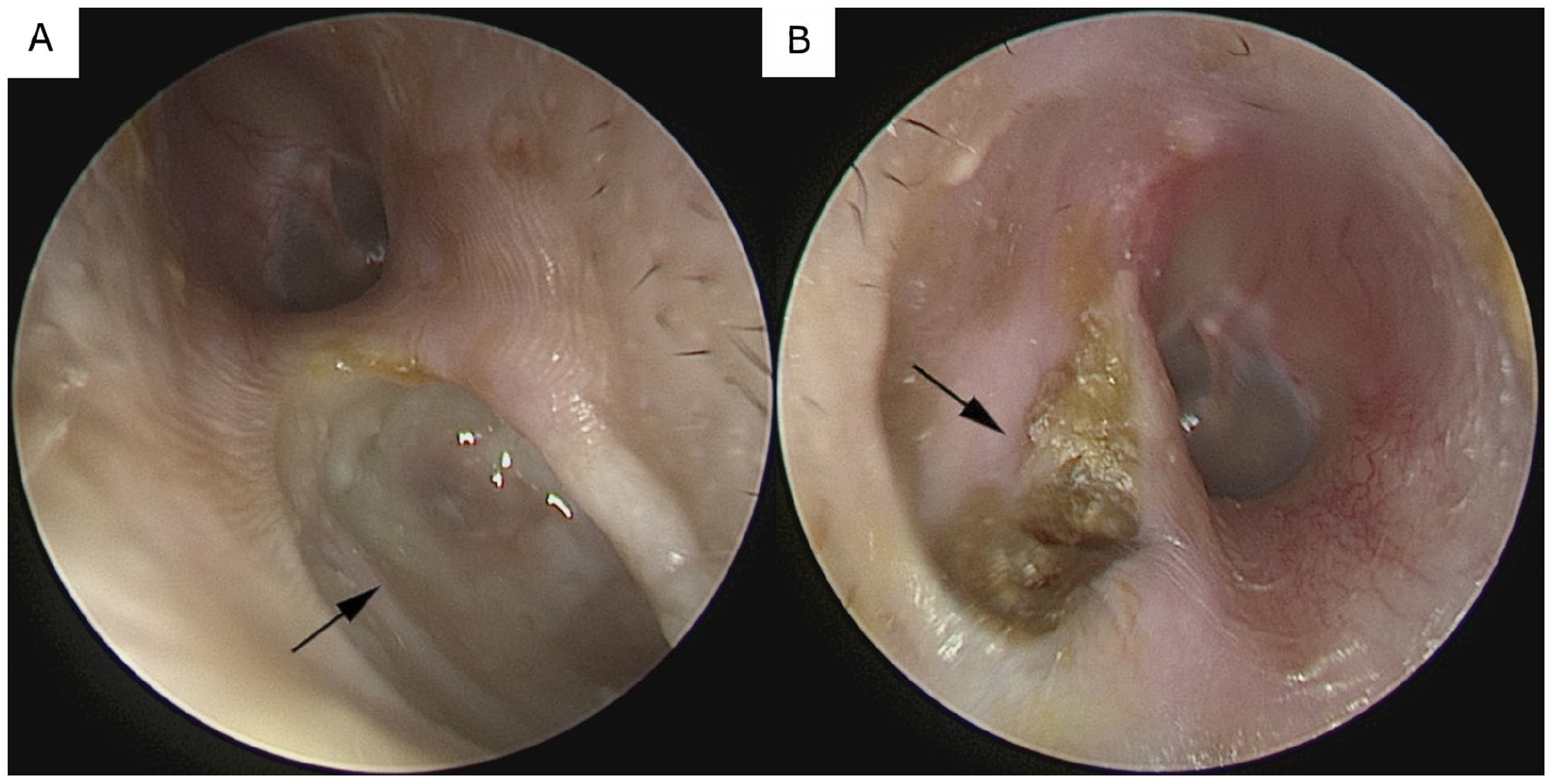
Endoscopic views of the bilateral external auditory canals. (A) Right ear: Focal erosion of the inferior bony canal wall with adherent necrotic tissue and mucopurulent discharge. (B) Left ear: Displays superficial bony exposure along the canal floor, with scattered necrotic debris and purulent secretion.
Computed tomography of the temporal bones demonstrated soft tissue masses occupying both EACs, with more pronounced bone erosion on the right side, extending into the inferoanterior cells of the right mastoid (Figures 2 and 3). There was no evidence of intracranial extension or sigmoid sinus thrombosis. Based on these imaging and clinical findings, a diagnosis of imatinib-associated temporal bone osteonecrosis was established.
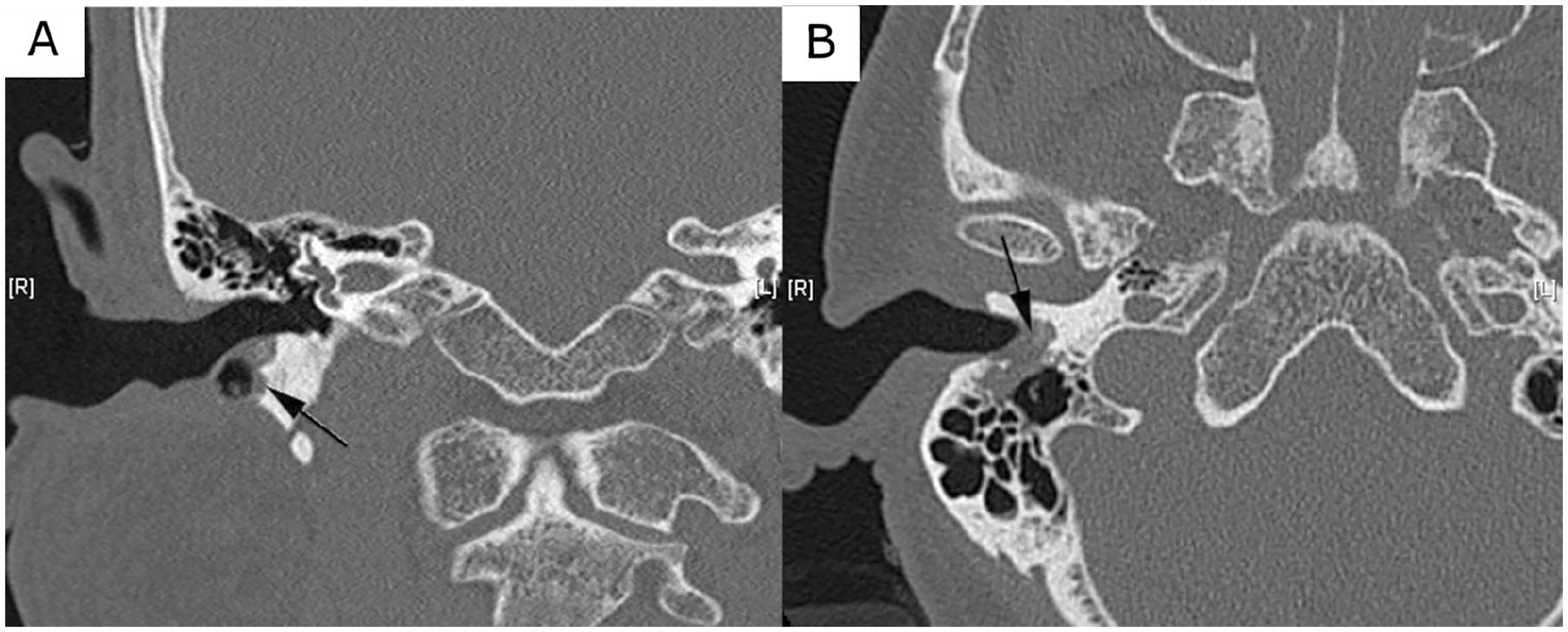
Temporal bone computed tomography demonstrating right external auditory canal and mastoid changes. (A) Right ear, coronal view: The image shows bony erosion of the inferoanterior mastoid air cells with adjacent soft tissue involvement extending toward the external auditory canal. (B) Right ear, transverse view: Arrow indicates subtle cortical irregularity along the inferior wall of the external auditory canal with adjacent soft tissue thickening, suggestive of bony involvement.
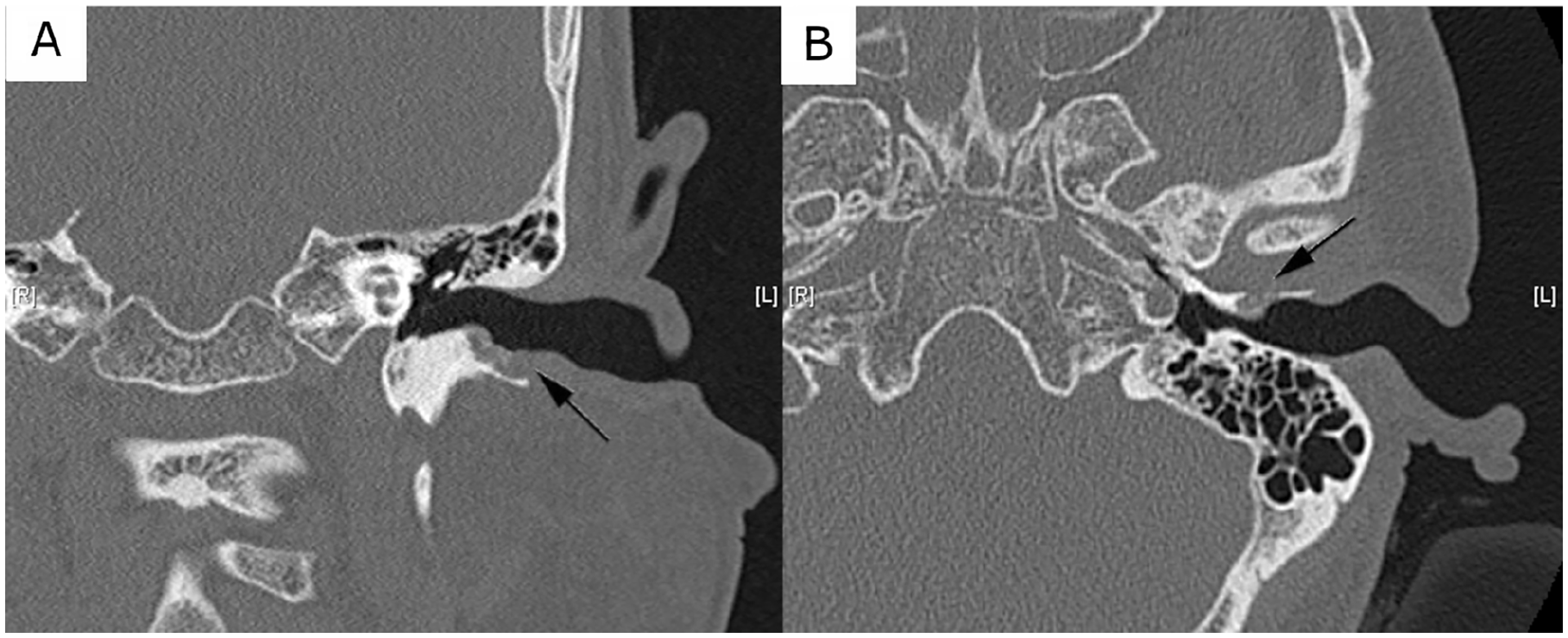
Temporal bone computed tomography demonstrating left external auditory canal and mastoid changes. (A) Left ear, coronal view: The image shows focal erosion along the inferior wall of the external auditory canal with adjacent soft tissue density. (B) Left ear, transverse view: The image reveals cortical disruption along the canal floor with early involvement of the anterior mastoid air cells.
The patient underwent debridement of necrotic tissue under local anesthesia to remove nonviable bone and infected debris. A 4-week course of oral ciprofloxacin was prescribed to address secondary bacterial infection, and he was instructed to perform regular outpatient aural toileting to prevent further accumulation of purulent material. Close follow-up was arranged to monitor healing and assess for potential recurrence.
Imatinib, a tyrosine kinase inhibitor (TKI), is widely used as a first-line therapy for CML due to its targeted inhibition of the breakpoint cluster region–Abelson murine leukemia viral oncogene homolog 1 (BCR-ABL) fusion protein activity. By blocking this oncogenic tyrosine kinase, imatinib effectively suppresses leukemic cell proliferation and induces apoptosis, leading to high response rates, durable cytogenetic remission, and an overall survival rate exceeding 85%. 1 Despite its efficacy, imatinib is associated with various side effects, most commonly edema, nausea, muscle cramps, diarrhea, and rashes. These adverse effects are generally mild and reversible. However, long-term imatinib use has been linked to alterations in bone metabolism, raising concerns about potential skeletal complications.
While TKI-associated osteonecrosis is well documented in the jaw, reports of temporal bone involvement remain exceedingly rare. The pathophysiology underlying imatinib-related osteonecrosis is not fully understood but is thought to involve impaired bone remodeling due to inhibition of osteoclast function. TKIs such as imatinib disrupt the normal balance of bone resorption and formation, potentially predisposing patients to localized bone necrosis, particularly in areas of reduced vascular supply.
Medication-related osteonecrosis of the external auditory canal is an uncommon but recognized entity. Most reported cases are associated with bisphosphonates, 2 denosumab, 3 and agents known to affect bone turnover. The clinical presentation of external auditory canal osteonecrosis can range from asymptomatic bony exposure to severe necrosis necessitating extensive surgical debridement. Symptoms often include persistent otorrhea, ear pain, conductive hearing loss, and, in advanced cases, exposure of underlying bony structures.
In this case, the patient’s presentation posed a diagnostic challenge, as external auditory canal necrosis is rarely encountered in patients receiving imatinib. 4 Given the absence of other known risk factors such as prior radiation therapy, bisphosphonate exposure, or chronic infections, the temporal association with prolonged imatinib use suggests a possible causal relationship. This underscores the need for increased awareness among clinicians regarding potential bone-related complications in patients receiving long-term TKI therapy.
Management of imatinib-associated temporal bone osteonecrosis remains largely supportive, with an emphasis on local wound care, infection control, and, in severe cases, surgical intervention. Conservative measures such as topical or systemic antibiotics, regular aural cleaning, and close surveillance are often sufficient for mild to moderate cases. In more extensive disease, surgical debridement may be necessary to remove necrotic bone and promote healing. The decision to continue or discontinue imatinib therapy should be individualized, weighing the benefits of leukemia control against the risks of progressive osteonecrosis.
This case highlights the importance of recognizing rare medication-associated adverse effects and the need for vigilant, interdisciplinary monitoring of long-term TKI therapy. Clinicians managing patients on TKIs should maintain a high index of suspicion for atypical complications, particularly in those presenting with persistent otological symptoms. Further research is warranted to elucidate the mechanisms underlying TKI-related osteonecrosis and to establish guidelines for prevention and early intervention.
Footnotes
Ethical Considerations
This study was granted by the Chang Gung Medical Foundation institutional review board (IRB: 202401823B0).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.