
Abstract
Objectives:
Due to its generally-poor prognosis and varied clinical presentation, cervical cancer of unknown primary (CUP) poses particular challenges for clinical and imaging diagnosis. Differential diagnoses of CUP syndrome may also include lateral cervical cysts. When a benign neck cyst is initially suspected, squamous cell carcinoma is often diagnosed after receiving histopathology. Our study investigates the risk factors to differentiate between CUP syndrome and lateral neck cysts (LNC) to possibly improve the prognosis.
Methods:
Between 2013 and 2023, 244 patients with an initial diagnosis of LNC (n = 121) or CUP (n = 123) were recruited from the Department of Otorhinolaryngology of Heidelberg University Hospital and underwent panendoscopy with lymph node removal. In general, disease- and progression-free survival, prognostic relevant risk factors, and treatment data were recorded and analyzed.
Results:
The mean age of patients with CUP was significantly higher at 65 ± 13.2 years than that of patients with LNC (41 ± 15.8 years; P = .000). The calculated cutoff value was 50 to 59 years for a 50% chance of CUP syndrome or other malignant neck mass. Alcohol and tobacco consumption were not found to be risk factors. Previous tumor diseases were diagnosed more frequently in patients with CUP than in patients with LNC (P = .045). The 5 year overall survival for patients with CUP was 77.0% and did not differ significantly between the other various tumor entities (P = .423).
Conclusions:
The consideration of patient-specific factors such as age or synchronous/asynchronous malignancies is crucial in the diagnostic decision-making process. In the age group of 50 to 59 years, there is ~50% probability of diagnosing CUP syndrome with unilateral painless neck swelling. A thorough clinical examination using panendoscopy with at least 1 unilateral tonsillectomy and biopsies from the base of the tongue is essential to detect a possible primarius early and improve the prognosis.
Keywords
Introduction
Treatment for and diagnosis of patients with cervical lymph node metastases without a detectable primary tumor remains a major challenge. Criteria for cancer of unknown primary (CUP) syndrome are met if a histologically- or cytologically-confirmed malignancy is present after the primary diagnosis is completed without a detectable primary tumor. Due to the generally-poor prognosis and the wide variety of manifestations, cervical CUP syndrome places particular demands on clinical and imaging diagnostics. Smokers have a higher risk of developing CUP syndrome. 1 The 1 year survival probability after a CUP diagnosis is about 20% and has not improved significantly over time. 2
For the differential diagnosis of CUP syndrome, lateral neck cysts (LNC) are considered congenital and benign anomalies of the second or third branchial arch. They are the most common congenital cause of a tumor-like mass in the neck. According to the literature, 11% to 21% of patients with LNC have squamous cell carcinoma (SCC), originally considered benign neck cyst. 3 Other authors suggest a secondary malignancy of LNC. 4 In adults treated for a cystic laterocervical mass according to the initial diagnosis, malignancy can only be ruled out after the histological result is available. In the event of malignancy, targeted biopsies of Waldeyer’s ring and, as a rule, bilateral tonsillectomy should be performed for further diagnostic clarification. The preoperative differential diagnosis of CUP syndrome from LNC remains a challenge and is the subject of this study.
The purpose of this study was to identify prognostic factors for the 2 differential diagnoses, CUP syndrome and LNC. In addition, diagnostic procedures for pretherapeutic imaging and surgical interventions will be compared and analyzed. Another focus is on the presentation of cases in which a primary tumor, initially diagnosed as LNC or CUP syndrome, was later discovered.
Patients and Methods
Ethical Considerations
The Ethics Committee of the Medical Faculty of the University of Heidelberg granted permission to conduct the study (Project No. S-507/2023) according to the Declaration of Helsinki on biomedical research involving human subjects. All data were pseudonymized before analysis.
Recruitment
Between 2013 and 2023, a total of 244 patients with an initial diagnosis of LNC (n = 121) or CUP syndrome (n = 123) were recruited in the Department of Otorhinolaryngology of Heidelberg University Hospital and underwent panendoscopy with lymph node removal. Exclusion criteria for the study were patients under 18 years of age, patients with lateral neck fistulas, median neck cysts or fistulas, and patients with a CUP syndrome not localized in the cervical region (eg, thoracic or intracranial).
All patients underwent a pretherapeutic staging, which included a comprehensive clinical examination by an ears, nose, throat (ENT) specialist. For imaging, patients underwent contrast-enhanced computed tomography (CT) of the head/neck and thorax or contrast-enhanced magnetic resonance imaging (MRI) of the neck and abdominal ultrasound. The subsequent staging included a panendoscopy to rule out a primary tumor. Furthermore, positron emission tomography (PET)-CT was performed in almost half of the patients. The International Union Against Cancer classification was used for the TNM classification. 5 The results were evaluated retrospectively by reviewing medical records. Patient data were documented using the IS-H software (SAP, Walldorf, Germany). Patient- and treatment-specific data, such as age, gender, and treatment strategy, were assessed. Furthermore, the time to therapy, the risk of an initial false differential diagnosis, and tumor-specific data were also examined. These were the date of diagnosis, complete staging parameters, and staging according to the TNM classification. For a meaningful evaluation, the status of human papillomavirus (HPV) was routinely checked.
Overall survival (OS) was calculated as the time from diagnosis to death. Disease-free survival (DFS) was calculated from complete remission after treatment to recurrence, the occurrence of a second cancer, or death. Progression-free survival (PFS) was defined as the time from stabilization of the disease to the recurrence or appearance of a new metastasis.
Statistical Analysis
The underlying analyses of this study were performed using R, Version 4.0.2 (R Core Team (2022); R Foundation for Statistical Computing, Vienna, Austria). Unless otherwise stated, the values in brackets after the variables represent the mean value. Within the table, the metric variables are presented as means ± standard deviation, while the categorical variables are presented as absolute numbers and percentages. Potential differences between groups were examined using the Wilcoxon test for nonparametric data and Student’s t test for metric data. A P < .05 was considered statistically significant. Patient data were analyzed and compared. Visualizations and graphical analyzes were performed using R’s ggplot library.
Results
The 121 patients with a suspected LNC presented to our clinic on average 36.8 ± 93.6 weeks after the onset of the first symptoms. In 19 patients, the time of first symptoms was not documented. The female patients presented at 21.6 ± 38.4 weeks, which was not significantly earlier than the male patients (52 ± 126.6 weeks; P = .095). Patients with a working diagnosis of CUP syndrome presented to our clinic on average 14.4 ± 21.8 weeks after the first symptoms. In 50 patients, the time of the first symptoms was not documented. There were no significant differences between the genders: 15.4 weeks in female patients and 14.1 weeks in male patients (P = .834). Patients with suspected LNC presented significantly later until diagnosis was made in our clinic (P = .022; Table 1).
Patient Characteristics.

Abbreviations: CUP, cancer of unknown primary; LNC, lateral neck cyst; SD, standard deviation.
The mean age of patients with a suspected LNC was 41.0 ± 15.8 years (range: 18.1-86.4). Women were, on average, 38.1 ± 14.6 years (range: 18.1-80.6) and therefore 6 years younger than male patients (44.2 ± 16.4 years; range:18.1-86.4; P = .033). On the contrary, the age of patients with suspected CUP syndrome was 65.0 ± 13.2 years (range: 18.6-93.9). In this group, the women were, on average, 66.5 ± 13.2 years old (range: 34.2-81.8) and therefore slightly older than male patients (64.5 ± 13.3 years; range: 18.6-93.9; P = .468). Regarding the 2 groups, patients with a suspected diagnosis of LNC were significantly younger than patients with suspected CUP (P = .000). The same significant difference was observed with the histopathologically-confirmed diagnosis (mean LNC: 40.1 vs mean CUP: 66.2, P = .000).
In the 50 to 59 age group, there is ~50% probability of diagnosing CUP syndrome with painless unilateral neck swelling (Figure 1).

Probability density function of age in dependency of suspected diagnosis.
The referral of patients to our clinic was not comprehensible for 21 patients. Most (n = 154, 69.1%) were referred by a private practice ENT specialist. Additionally, 27 patients (12.1%) were referred by their general practitioner. The remaining patients sought medical help on their own initiative or were referred by colleagues from other medical specialties.
Diagnostic Procedure
Diagnosis of Lateral Cervical Cyst
A total of 90 patients were referred with a suspected diagnosis of LNC. The average size of the LNC was 39.0 ± 15.3 mm (range: 8-90). The lateralization was distributed similarly (right: 46.3%; left: 53.7%). Cysts were found most frequently in level II (n = 72; 60%) and level III (n = 42; 35%). After gathering medical history and clinical examination, the working diagnosis of a LNC was made in a total of 121 patients. The working diagnosis of a LNC was confirmed in 95.9% (n = 116) of the patients. In 5 patients, a different diagnosis was established after histopathological examination, namely oncocytic papillary cystadenoma, lymphangioma, cystadenolymphoma, salivary gland cyst, and inflamed lymph node. A total of 12 patients with suspected CUP syndrome were referred, but then did not show signs of malignancy on histology.
All patients underwent surgery to treat the lesion and for histopathological confirmation. Furthermore, 12 patients underwent a panendoscopy, 7 of whom showed abnormalities. Two patients had simple vocal cord leucoplakia and 2 patients had asymmetry of the palatine tonsils. Other abnormalities included a cyst on the lateral pharyngeal wall, a vocal cord polyp, and unilateral tongue base hyperplasia.
In retrospect, panendoscopy was performed more frequently in older patients (mean, 50.0; range: 31.0-72.5) than in younger patients (39.0; range: 18.1-86.4; P = .017). All patients who underwent panendoscopy were smokers, and 1 patient had a history of malignancy.
In patients treated with a suspected LNC, the sensitivity was 90.1%, which means that 90.1% of them actually had a LNC. Specificity was 85.4%. The positive predictive value for the working diagnosis of a LNC was 85.8%, and the negative predictive value was 89.7%.
Diagnosis of CUP Syndrome
A total of 66 patients with suspected diagnosis of CUP syndrome were referred. After clinical examination, 123 patients finally received a working diagnosis of CUP, including 20 patients with only cystic lateral neck mass. This included 18 patients (14.6%) who were initially referred with the suspicion of LNC. However, after histologic confirmation, a malignant disease was diagnosed. The mean age of these patients was 57.7 ± 11.96 years (range: 34.2-77.8), including 13 male and 5 female patients. Nine of these patients underwent PET-CT after histological confirmation of metastasis/CUP. A standardized uptake value (SUV) of 2.5 or higher is generally considered an indicator of malignant tissue. However, it should be noted that there is a wide range of SUV values for similar diseases. An SUV around 2.5 can also be measured in nonmalignant regions. On the contrary, small tumors can also have a maximum SUV of <2.5. 6 Interestingly, in some cases, even when a primary tumor was detected on PET-CT with a higher SUVmax, no primary tumor was histologically confirmed (Table 2). All patients underwent panendoscopy, which was performed simultaneously in 8 patients and sequentially in the others. After complete staging, including CUP panendoscopy, the final diagnosis of CUP was confirmed in only 10 patients. Seven patients had oropharyngeal carcinoma and 1 patient had nasopharyngeal carcinoma. Two patients had a medical history of malignancy.
PET-CT Results of Primarily-suspected Lateral Neck Cysts That Were Malignant.
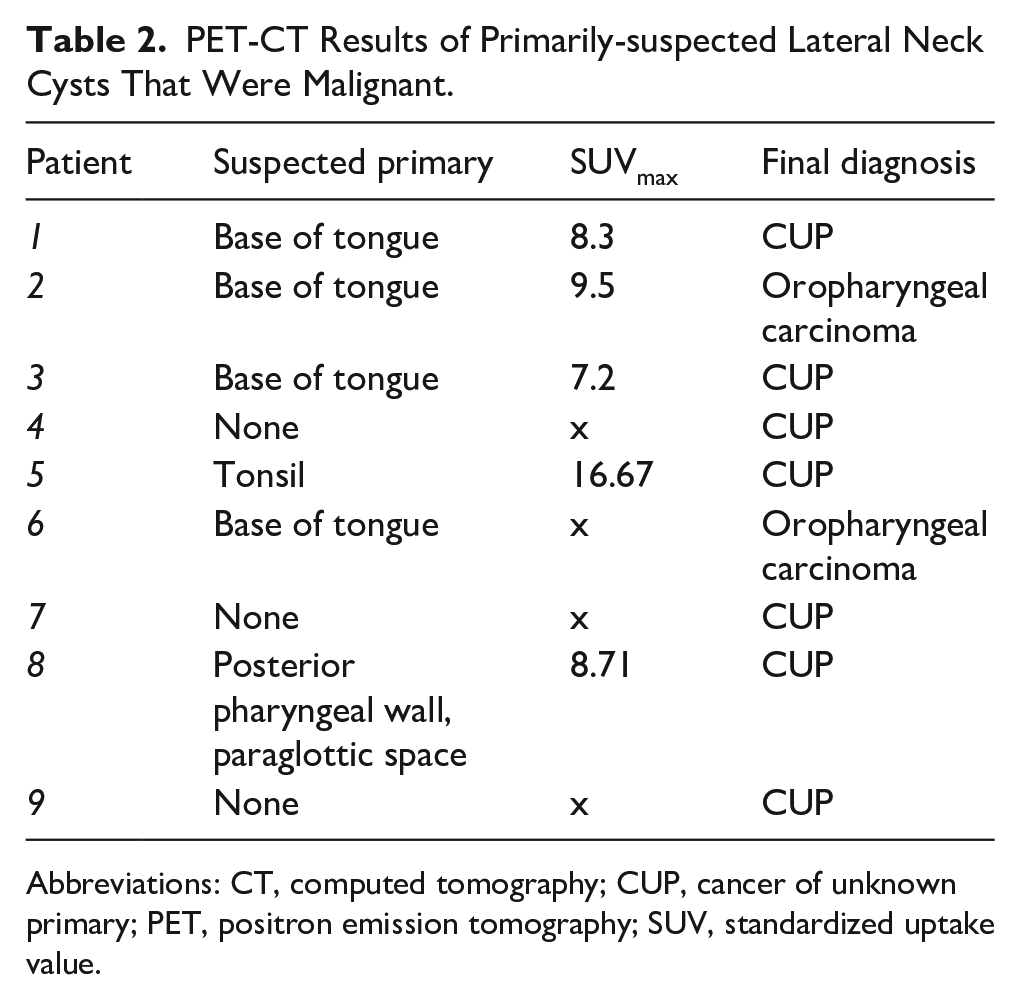
Abbreviations: CT, computed tomography; CUP, cancer of unknown primary; PET, positron emission tomography; SUV, standardized uptake value.
Risk Factors
Information on the consumption of harmful substances was not available in a total of 21 patients. Half of the patients with LNC had nicotine abuse. Of patients with a working diagnosis of CUP, 60.7% stated that they had never used nicotine, while another 7.5% of patients reported that they had stopped using nicotine. This showed a significant difference in nicotine history (LNC = 0.5; CUP = 0.34; P = .026). Alcohol consumption was reported as occasional or infrequent by 39.1% (n = 45) of patients with LNC and 29.6% (n = 32) of patients with CUP. Furthermore, 10.4% (n = 12) of patients with lateral cervical cysts and 12.0% (n = 13) of patients with CUP reported regular alcohol consumption. Three patients (2.6%) with neck cyst and eleven patients (10.25%) with CUP reported the ingestion of large amounts of alcohol to the point of abuse. The remaining 47.8% (n = 55; LNC) and 48.1% (n = 52; CUP) stated that they abstained from alcohol. In this respect, there were no significant differences between the 2 groups (P = .213). Of the patients with a working diagnosis of lateral cervical cyst, only 9.1% (n = 11) had a history of a malignant tumor. Four of these patients had a history of breast cancer, and another 4 had a history of hematologic neoplasia. Other malignancies included testicular carcinoma, osteosarcoma, and glioblastoma. A part of 17.9% (n = 22) of patients with a working diagnosis of CUP had a history of malignancy. Six of these patients had prostate cancer, 3 had hematologic neoplasms, 2 aurothelial carcinomas, and 1 each pancreatic carcinoma or breast cancer. The other malignancies included malignant melanoma, Leydig tumor, non-small cell lung cancer, as well as carcinoma of the mouth and tongue floor. There was a significant difference between the 2 groups (LNC = 0.09; CUP = 0.18; P = .04; Figure 2).

Potential risk factors for malignancy.
As part of the additional staging diagnostics for suspected CUP syndrome, PET-CT or PET-MR was performed in around half of the patients (51.6%). The working diagnosis of CUP was confirmed in 73.2% (n = 90) of the patients. In 20 patients (16.3%), histopathological examination and completed staging revealed oropharyngeal carcinoma, and in 4 further patients (3.3%) nasopharyngeal carcinoma. A total of 9 patients had other diagnoses, such as primary parotid carcinoma, oral floor carcinoma, or metastases of SCC of the skin. One patient had a thymoma (Table 3).
Definitive Diagnosis After Working Diagnosis CUP.
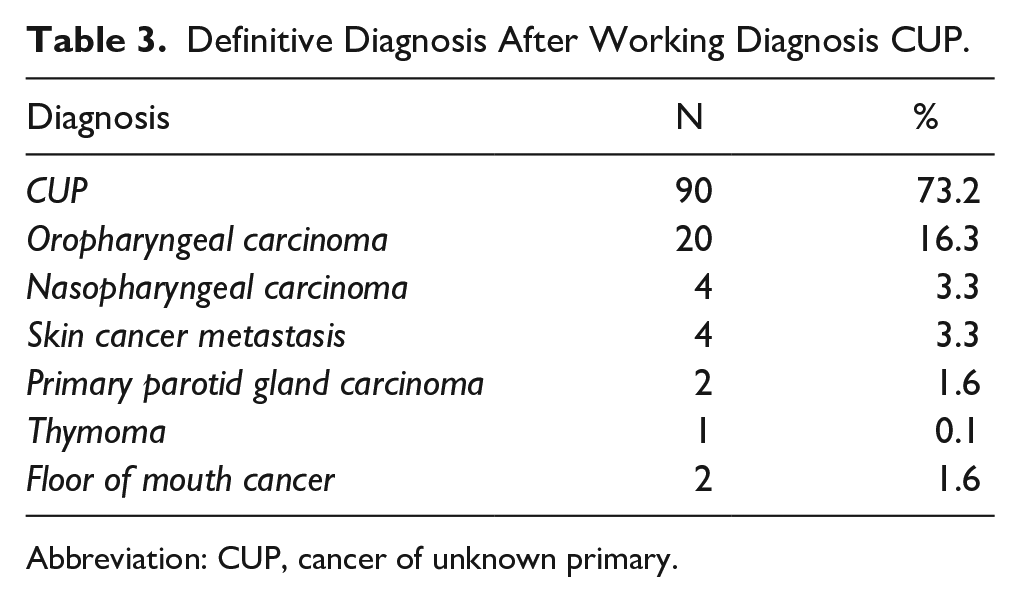
Abbreviation: CUP, cancer of unknown primary.
The lateralization was evenly distributed (right: 40.7%; left: 52.8%), with 7 patients (5.7%) having manifestations on both sides and another patient centrally. The most frequent location was in level II (n = 61; 49.6%) and level III (n = 31; 25.2%). In 20 patients (16.5%), a cystic mass was observed on initial imaging. The nodal (N) stage at the time of diagnosis was most commonly cN2 (41.8%), followed by cN1 in 29.5% and cN3 in 27.9% of the cases. The N stage could not be further determined after external diagnostics in 1 patient. In another patient, a stage N0 was present after a change in diagnosis to a primary extensive floor of mouth carcinoma. Ten percent of the patients initially had distant metastases.
Therapy of CUP Syndrome
A total of 111 patients (90.2%) underwent panendoscopy. In the remaining patients, panendoscopy was refused after the confirmation of the diagnosis for further staging or was considered unnecessary for various reasons, especially after the diagnosis of another tumor entity, such as cutaneous metastases of SCC. In 48.8% (n = 60) of the patients, panendoscopy was performed at the same time as histological confirmation of suspicious cervical lymph node. In 41.5% (n = 51), the panendoscopy was performed sequentially, that is, after biopsy or excision of the cervical lymph node.
Bilateral tonsillectomy was performed in 40.7% of the patients (n = 50). Another 23.6% (n = 29) did not undergo tonsillectomy. Unilateral tonsillectomy was performed in 3 patients. In 10.6% of the patients, only a tissue biopsy was taken from the tonsils. In 22.8%, a tissue biopsy was performed in the region after a previous tonsillectomy.
In a total of 4 patients, primary treatment could not be pursued further. A part of 25.2% (n = 30) of patients with CUP received definitive radiochemotherapy. The other 17.6% (n = 21) patients underwent primary surgical treatment. Most of the patients (52.1%) underwent surgery with adjuvant (chemo-) radiotherapy. Approximately 5% (n = 6) of patients with CUP received palliative/systemic treatment.
Survival Rates
The 5 year OS for patients with CUP was 77.0%. OS curves did not differ significantly between the various tumor entities in our cohort (P = .423). The 5 year DFS for patients with CUP was 75.6%. Similarly, there were no significant differences in the initial suspicion of CUP compared with other tumor entities (P = .198). The median PFS for patients with CUP was 0.81 years, with no significant differences compared with other entities (P = .077). Looking at the PFS of all patients with a working diagnosis of CUP, regardless of the final diagnosis, the median PFS was 0.66 years (Figure 3). A total of 28 patients with CUP (22.8%) experienced recurrence or tumor progression during the course of therapy.

Overall survival, disease-free survival, and progression-free survival. CUP, cancer of unknown primary; OCA, oropharyngeal cancer; NCA, nasopharyngeal cancer.
Discussion
Cystic neck lesions pose a relatively-uncommon scenario in the routine practice of head and neck specialists or hematologists. Enhancing therapeutic effectiveness hinges on accurately discerning whether the lesion is a benign branchial cleft cyst or a malignant, potentially-metastatic condition. This diagnostic challenge underscores the need for precise assessment and management strategies to optimize patient outcomes.
As an important result of our study, we were able to establish that age appears to be a decisive risk factor for CUP syndrome. The mean age of patients with a histopathologically-confirmed LNC was significantly younger than in patients with CUP (mean LNC: 40.1 vs mean CUP: 66.2, P = .000). Other authors have also described the age differences in the differential diagnosis of a lateral cystic neck mass and malignant findings. 7 In patients older than 40 years, a risk of malignancy of 56% was reported. However, other authors report a lower proportion of malignant pathological findings, ranging up to 31% in this age.8,9 The calculated cutoff value here was 50 to 59 years for a 50% chance of CUP syndrome or other malignant neck mass and should be considered in the future when treating prominent neck swellings.
Diagnostics
A detailed medical history and an investigation of the patient’s medical records are essential for the differential diagnosis of a LNC and a CUP syndrome. Medical history should include symptoms related to the upper respiratory tract, as well as a history of exposure to toxins and previous malignancies. Additionally, it is crucial to inquire about the onset of the mass and the subjective changes in its size over time. Interestingly, the 121 patients diagnosed with a LNC presented significantly later at 36.8 weeks after the onset of symptoms compared with the patients diagnosed with CUP syndrome at 14.3 weeks. In these patients, the laterocervical mass was the only-noticeable symptom in each case. The next step focuses on a comprehensive clinical examination by an ear, nose, and throat specialist, which should include ear examination, nasal endoscopy, complete pharyngoscopy, and laryngoscopy. Palpation of the neck should also be performed to further clarify the differential diagnosis. Most of patients with LNC (95%) exhibited a mass at levels II and III.
Seven patients with suspected LNC diagnosis showed clinical abnormalities on physical examination, but the malignancy was later ruled out on panendoscopy. All patients underwent imaging, which included ultrasound in each patient, and sometimes additionally included cross-sectional imaging with CT or MRI. Cross-sectional imaging was always performed in patients suspected of having a malignant lesion. However, even the use of CT and MRI could not reliably distinguish between malignant and nonmalignant lesions. The introduction of ultrasound, CT, and MRI has remarkably improved diagnostic accuracy in terms of anatomical location and diagnostic certainty. 10 Especially for superficial lesions, ultrasound is the diagnostic method of choice due to its noninvasiveness, cost-effectiveness, and the absence of radiation exposure. 11 A CT scan is particularly useful in cases of infected neck cysts to rule out deeper neck infections. While potential signs of malignancy can be accurately described by CT and MRI, the differentiation between benign and malignant lesions remains a challenge and must be made in conjunction with clinical findings and medical history.3,12 Newer imaging modalities such as PET-CT are recommended for primary site detection in cases of histologically-confirmed SCC metastases in the head and neck region, 13 but not yet in suspicion of LNC. Some suggest that 18F-FDG PET-CT could offer greater accuracy for head and neck SCC, given its reputation as a more sensitive technique than other imaging modalities.14,15 Abadi et al demonstrated in their study on PET-CT as the primary imaging modality for cystic neck lesions a sensitivity of 95% in detecting malignancy in such cases. However, in 26% of the patients, suspicion of malignancy was raised due to increased metabolism, which was later disproven by histological examination. 16
In our study, half of the 18 patients who were initially referred with a suspected diagnosis of LNC and later confirmed to have a malignant finding received a PET-CT after a interdisciplinary tumor board decision. Subsequently, all patients underwent a panendoscopy. PET-CT was particularly helpful in detecting a primary tumor in the base of the tongue by enabling targeted biopsy and confirmation of a primary tumor. However, in most cases, despite increased metabolic activity and elevated SUVmax in PET-CT, no primary tumor could be histologically confirmed in the examination area. This goes along with the work of Albertson et al, who described a lower spatial resolution in the head and neck region, as well as several normal structures, such as the Waldeyer’s ring, with physiological FDG uptake. 17 One meta-analysis indicated that PET-CT has a false positive-rate of 39% for tonsillar lesions and limited sensitivity in the tongue base. 18 Another common cause of false-positive findings on 18F-FDG PET-CT is reactive tonsillar hyperplasia or reactive adenopathy, which is prevalent in these patient populations. 19
Risk Factors
Alcohol consumption and tobacco use are well-known risk factors for the development of head and neck squamous cell cancer (HNSCC). 20 In our cohort, there was a generally-higher prevalence of smoking and increased alcohol consumption among patients with LNC, although without statistical significance.
Furthermore, a history of carcinoma was identified as a significant risk factor for the occurrence of a CUP syndrome (P = .04). Even when HNSCC was excluded from the medical history, patients with a history of carcinoma more frequently presented a malignant finding in unilateral neck swelling. However, this observation is probably mainly attributed to age, as carcinomas occur in 60% of patients over the age of 65 years. 21 However, HPV infections also contribute to the oncogenesis in HNSCC, although, in our cohort, no patient had an HPV-associated tumor in their medical history.
Therapy
The relatively-high percentage of malignant findings in patients suspected of LNC (14.6%) in the present series underscores the importance of early biopsy in patients with neck cysts to prevent delays in diagnosis and the initiation of treatment. All patients underwent surgery as single node excision to treat the lesion and for histopathological confirmation. Additionally, panendoscopy was performed in 9 of the 12 patients with initial referral as CUP, being an LNC after histopathological examination. A fine-needle biopsy is generally not performed at our center. The primary objective of our approach is to avoid the spread of tumor cells in the case of malignancy and to avoid the false-negative or inconclusive diagnosis in cystic lesions, as reported by Sira and Makura. 1 Furthermore, it has been demonstrated that open biopsies in the neck region, followed by subsequent neck dissection, do not alter the prognosis of patients with oropharyngeal carcinoma. 22
In the cohort diagnosed with CUP, 90.2% underwent a panendoscopy. Approximately half of the patients received this procedure as part of cervical histological confirmation, while the other half underwent it subsequently after receiving histology. The need to sample the tongue base and tonsillectomy became evident, despite a normal clinical examination, as the diagnosis changed to oropharyngeal carcinoma in a total of 20 patients (16.3%). Among these, 8 patients underwent PET-CT, which was unremarkable in 2 cases of subsequent tongue base and tonsillar carcinoma, emphasizing the importance of sampling from the tongue base and performing tonsillectomy. For the 12 patients without PET-CT, the diagnosis of CUP changed to oropharyngeal carcinoma after histopathological confirmation. The only basis for discussion is the question of bilateral tonsillectomy. Tonsillar carcinomas typically manifest ipsilaterally to the existing cervical swelling, although some authors recommend bilateral tonsillectomy due to the contralateral spread of metastatic cancer from occult tonsil lesions up to 10%. 23 However, in our study, no primary tumor was found contralateral to cervical mass, so a bilateral tonsillectomy should be reconsidered as a diagnostic focus search for CUP syndrome. As already mentioned, PET-CT cannot replace additional invasive measures to confirm the diagnosis, particularly in the area of the base of the tongue and tonsils.
Most of the patients (52.1%) underwent adjuvant radiotherapy (chemo) after the decision had been made at the interdisciplinary tumor conference. The estimated 5 year survival rate for patients with CUP was 77.0% and did not differ significantly from other tumor entities. Other authors described 5 year survival rates for patients with CUP from 42.7% to 63.2%24,25 and significantly-higher survival rates for patients without known primary. 25
Conclusion
The diagnostic decision-making process should consider patient-specific factors such as age or synchronous/asynchronous malignancies. As a conclusion of the study, we note here for the first time that in the age group of 50 to 59 years, there is ~50% probability of diagnosing CUP syndrome with painless unilateral neck swelling. Therefore, careful clinical examinations using panendoscopy with at least 1 unilateral tonsillectomy and biopsies from the base of the tongue are essential to detect a possible primarius at an early stage and improve the prognosis. Although PET-CT is generally recommended, it does not replace other invasive diagnostic procedures to confirm the diagnosis of CUP syndrome.
Footnotes
Acknowledgements
The study was carried out with the support of the faculty of medicine in Heidelberg.
Ethical Considerations
The Ethics Committee of the Medical Faculty at the University of Heidelberg granted permission to conduct the study (Project No. S-507/2023).
Consent to participate
Consent to participate of all patients was not necessary according to the Ethics Committee of the Medical Faculty of Heidelberg.
Author Contributions
All authors made substantial contributions to the study. C.S.: participated in data acquisition and analysis, interpreted the data, and drafted the manuscript. M.S.: participated in data interpretation and statistical analysis. K.P.: designed and coordinated the study. P.K.P.: revised the manuscript. M.P.: designed and coordinated the study, participated in data acquisition and analysis, and critically revised the manuscript for important intellectual content.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.