
Abstract
Significance Statement
A ranula can be confused with various pathologies in the neck. The most common differential diagnoses include malignancies when it presents as a mass effect and salivary gland inflammations when it becomes infected. Misdiagnosis may lead to unnecessary treatments and surgical interventions, which can have negative consequences for patient well-being.
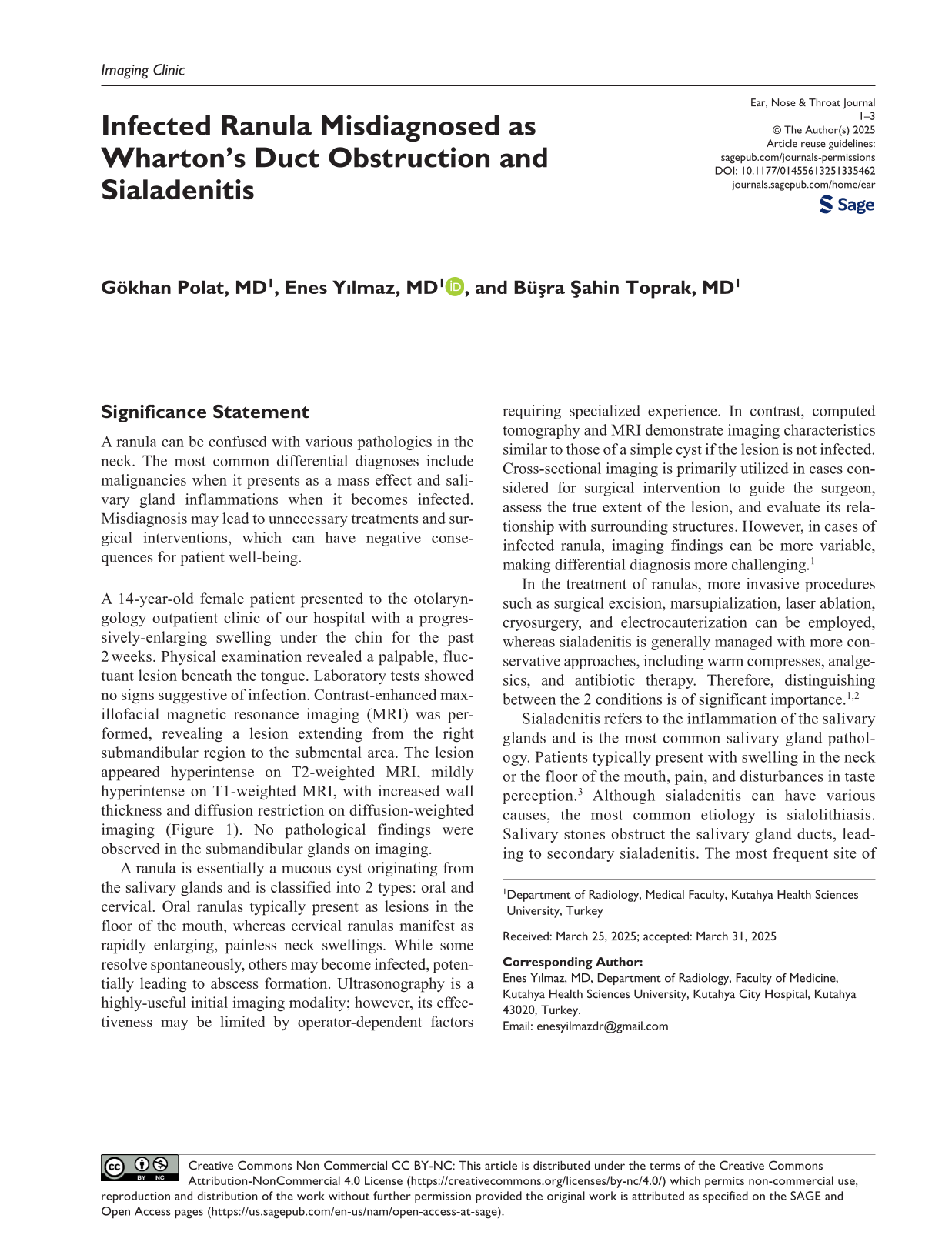
A 14-year-old female patient presented to the otolaryngology outpatient clinic of our hospital with a progressively-enlarging swelling under the chin for the past 2 weeks. Physical examination revealed a palpable, fluctuant lesion beneath the tongue. Laboratory tests showed no signs suggestive of infection. Contrast-enhanced maxillofacial magnetic resonance imaging (MRI) was performed, revealing a lesion extending from the right submandibular region to the submental area. The lesion appeared hyperintense on T2-weighted MRI, mildly hyperintense on T1-weighted MRI, with increased wall thickness and diffusion restriction on diffusion-weighted imaging (Figure 1). No pathological findings were observed in the submandibular glands on imaging.
On coronal T2-weighted MRI (A), a hyperintense lesion is observed (*). On axial diffusion-weighted MRI (B), the lesion demonstrates diffusion restriction (*). On axial T1-weighted MRI (C), the lesion appears hypointense, while on axial T2-weighted MRI (D), the hyperintense cystic lesion extends posteriorly and to the right lateral aspect of the floor of the mouth (red arrows). MRI, magnetic resonance imaging.
A ranula is essentially a mucous cyst originating from the salivary glands and is classified into 2 types: oral and cervical. Oral ranulas typically present as lesions in the floor of the mouth, whereas cervical ranulas manifest as rapidly enlarging, painless neck swellings. While some resolve spontaneously, others may become infected, potentially leading to abscess formation. Ultrasonography is a highly-useful initial imaging modality; however, its effectiveness may be limited by operator-dependent factors requiring specialized experience. In contrast, computed tomography and MRI demonstrate imaging characteristics similar to those of a simple cyst if the lesion is not infected. Cross-sectional imaging is primarily utilized in cases considered for surgical intervention to guide the surgeon, assess the true extent of the lesion, and evaluate its relationship with surrounding structures. However, in cases of infected ranula, imaging findings can be more variable, making differential diagnosis more challenging. 1
In the treatment of ranulas, more invasive procedures such as surgical excision, marsupialization, laser ablation, cryosurgery, and electrocauterization can be employed, whereas sialadenitis is generally managed with more conservative approaches, including warm compresses, analgesics, and antibiotic therapy. Therefore, distinguishing between the 2 conditions is of significant importance.1,2
Sialadenitis refers to the inflammation of the salivary glands and is the most common salivary gland pathology. Patients typically present with swelling in the neck or the floor of the mouth, pain, and disturbances in taste perception. 3 Although sialadenitis can have various causes, the most common etiology is sialolithiasis. Salivary stones obstruct the salivary gland ducts, leading to secondary sialadenitis. The most frequent site of stone formation is Wharton’s duct, the main drainage duct of the submandibular gland. When infectious processes complicate the inflammatory response, pyogenic abscesses may develop, contributing to swelling in the neck and floor of the mouth. 4
The cystic lesion in our case, initially evaluated as a ranula, may be mistaken for an abscess due to its fluctuation on physical examination. However, the absence of abnormalities in infection markers in laboratory tests should prompt the clinician to pursue imaging for differential diagnosis. Imaging can largely facilitate the identification of the primary pathology among the considered differential diagnoses.
Footnotes
Consent for Publication
We declare that written informed consent for the publication of patient information and images was provided by the patient’s legal representative.
Author Contributions
Gökhan Polat: writing—review and editing (lead), Enes Yılmaz: writing—review and editing (supporting), and Büşra Şahin Toprak: writing—review and editing (supporting).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.